

 PDF
PDF ePub
ePub Citation
Citation Print
Print


We recommend Lin et al. (1) for their interesting article on a case of atypical pulmonary metastases from carcinosarcoma of the parotid gland, demonstrating the radiologic features of an air-space pattern and calcification. We concur with their study in considering this type of lesions a formidable diagnostic challenge in the patients with unknown extrapulmonary malignancies. We would like to lend more support to this study by offering our experience with a similar exceptional case of atypical pulmonary metastases from a different kind of primary tumor.
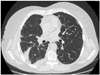
Recently, a 71-year-old afebrile female patient was admitted to our emergency department presenting 1-month history of chest pain and nausea. The chest radiography showed multiple small nodules throughout both lungs. The contrast-enhanced CT scan of the chest revealed the cavitating nature and a miliary pattern of the nodules (Fig. 1). The patient was suspected for the advanced pulmonary tuberculosis, but the quantiferon blood test resulted negative. A body CT was performed to better understand the overall clinical condition, and a solid mass was detected in the pancreatic isthmus (Fig. 2). At this point, a bronchoalveolar lavage was ordered in order to clarify the nature of the lung lesions. Some neoplastic cells testing positive for CK17 and CK19 were retrieved and the conclusive diagnosis was the metastases of pancreatic adenocarcinoma.
The cavitating pulmonary metastases from pancreatic adenocarcinoma are extremely rare; only 7 cases have been published so far (2, 3). Generally, their typical imaging appearance consists of consolidation, peripheral nodules, thickening of the interstitium or pleural effusion (2). The parenchymal cavitation represents a phenomenon, which is still understood very little. According to some authors, it could result from the proteolytic and lipolytic action of pancreatic enzymes produced by the metastases themselves, whereas others could result from their tendency to cystic degeneration. Furthermore, a miliary pattern has been described only twice, making the differential diagnosis from other benign conditions, mostly tubercolosis, even more difficult (2). The chest pain is clinical presentation of this condition representing another exceptional feature of this case. Our concern is that a thorough investigation should always be done, when coping with an apyrexial patient presenting with excavated lung lesions, in order to rule out a primitive gastrointestinal cancer.

 XML Download
XML Download