

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ultrasonography (US) plays an important role in the diagnosis and management of thyroid-related diseases. The development of high resolution US equipment has greatly influenced the management of thyroid nodules; indeed, currently US is frequently used as a first-line diagnostic tool, in both guidance of fine needle aspiration biopsy (FNAB) and for post-operative follow-up imaging. Since 1985, there have been numerous reports about thyroid US. However, most reports focus on the information gained from the actual imaging itself, such as results from assessment of the nodule, FNAB, or volumetry (1-10). To our knowledge, there is currently a paucity of articles presenting tips or pitfalls related to utilizing this modality (11, 12).
The intent of this pictorial review was to provide a framework for sharing interpretative and technical recommendations regarding thyroid US. We will detail normal thyroid and peri-thyroid anatomy, and then attempt to address common pitfalls associated with US equipment, examination skills, anatomy, interpretation, and extrathyroidal abnormalities (Table 1).
Go to : 
Normal Anatomy
The thyroid gland is a butterfly-shaped organ located in the midline of the anterior neck. It has two elongated lateral lobes (right and left), and is connected by the isthmus (Fig. 1). Approximately 40% of individuals have a pyramidal lobe arising from the isthmus that extends towards the hyoid bone (8, 13); this may be misinterpreted as a mass when it is enlarged (Fig. 2).
 | Fig. 1
Normal transverse US of thyroid gland. Cross-sectional US shows normal thyroid glands and surrounding structures. Both thyroid glands show homogeneous parenchymal echogenicity higher than anterior strap muscles. Both CCAs run laterally adjacent to both thyroid lobes and infrahyoid strap muscles overlie thyroid gland. Both SCM muscles are located antero-laterally and longus colli muscles are seen posterolaterally to thyroid gland. US = ultrasonography, SCM = sternocleidomastoid muscle, CCA = common carotid artery, IJV = internal jugular vein, Ant. Strap m = anterior strap muscle, Longus Colli m = longus colli muscle
|
 | Fig. 2Pyramidal lobe in 49-year-old woman with hypothyroidism.
A. On transverse ultrasonography small isoechoic mass (arrows) was seen at superior aspect of left thyroid lobe. B. Lesion (arrows) had same echogenicity as surrounding thyroid gland; thus, providing important diagnostic clue on longitudinal view.
|
The length of the lateral lobes is approximately 4-5 cm, with the transverse and antero-posterior diameter of the lateral lobes being approximately 2 cm and the thickness of the isthmus being less than 0.5 cm (8, 13, 14). The parenchymal echogenicity of a normal thyroid gland is homogeneous and higher than the overlying strap muscles of the neck. On a cross-sectional image, common carotid arteries and the internal jugular veins are typically visualized laterally adjacent to both thyroid lobes (Fig. 1). The esophagus is usually located to the left of the trachea. The parathyroid glands lie close to the deep surface of the thyroid gland but are generally unseen on US when they are normal. Some level VI lymph nodes can be seen adjacent to the lower poles.
Go to :
Pitfalls Associated with Equipment
For proper thyroid examination, a high frequency (10-15 MHz, at minimum more than 7.5 MHz) linear transducer is recommended (8, 15, 16). During thyroid US, transverse and longitudinal images should be obtained, while color Doppler images may be useful in selective cases (6). The convex transducer may be used in particular cases such as intrathoracic goiter.
Go to :
Pitfalls Associated with Examination Skills
When performing thyroid US, proper compression is essential: insufficient force may lead to imaging artifacts due to the round, protruding structure of the neck. The first such artifact discovered that can be linked to morphologic change is caused by inadequate pressure of the probe and it is associated with lesion location (Fig. 3). Failure to apply adequate pressure results in deeper lesions appearing more indistinct because of ultrasound attenuation. The attenuation is in proportion to frequency and is mainly caused by absorption (17). This can be controlled with time-gain-compensation (TGC) and gentle but proper probing pressure. Thus, the US performer should apply more force to the transducer and trim the focusing or TGC curve.
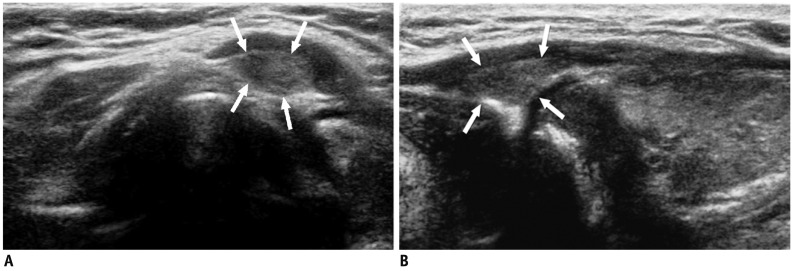
 | Fig. 3Deep located lesion in left thyroid lobe in 35-year-old man.
A. Without compression, ill-defined, taller-than-wide hypoechoic nodule (small arrows) suggesting suspicious nodule is visible. B. Following compression, margin of nodule can be seen more easily and carotid artery (large arrows) is also compressed.
|
The second type of artifact commonly encountered is posterior shadowing related to muscle interface. The shadowing is associated with sound transmission and different sound attenuation causes shadowing and enhancement. Unfortunately, artificial acoustic shadowing can result from the critical angle created by a steeply obliquely oriented tissue plane but it can be eradicated with firmer compression (18, 19). Such a shadow, mistakenly deemed a lesion, is sometimes referred to as a pseudolesion (Fig. 4). In the case of thyroid US, the interface between the sternocleidomastoid muscle and infrahyoid muscles may mimic an ill-defined hypoechoic lesion. To avoid misdiagnosis, the US performer must compress the transducer appropriately and confirm lesions on both transverse and longitudinal scan views.
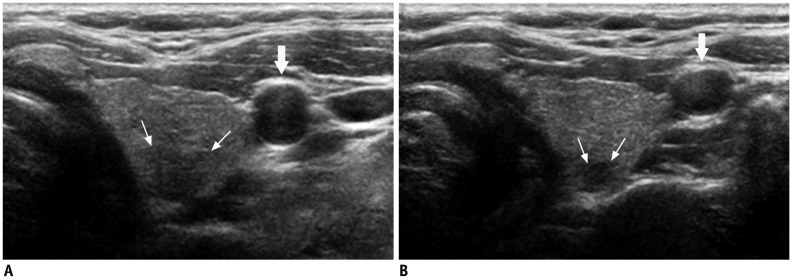
 | Fig. 4Artifact related with muscle interface in 28-year-old man.
A. Before compression, hypoechoic lesion (arrows) is visible in anterior portion of right thyroid lobe. B. Following compression, lesion disappeared as it was pseudo-lesion caused by shadow (field with dots) from sternocleidomastoid muscle interface.
|
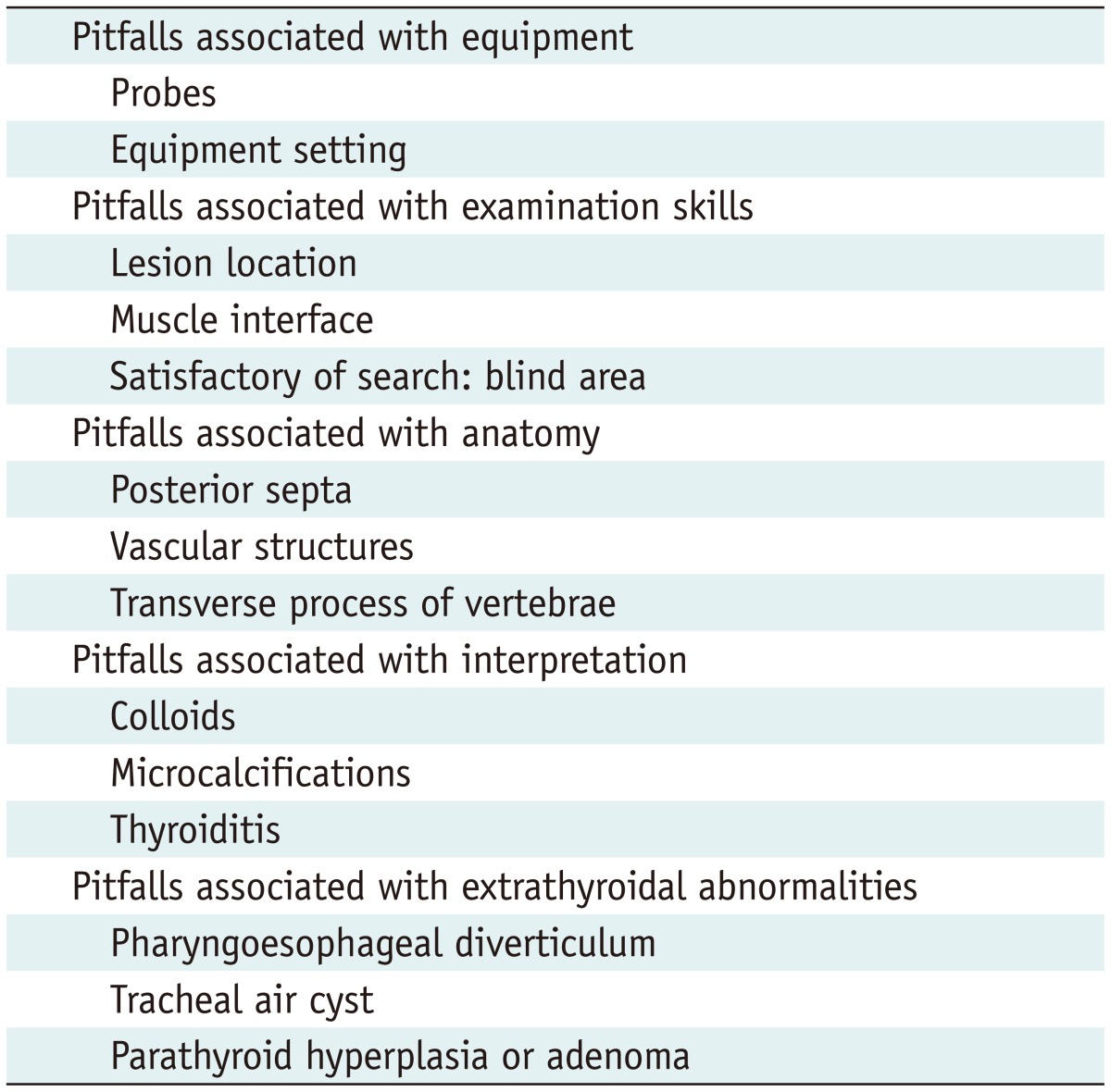
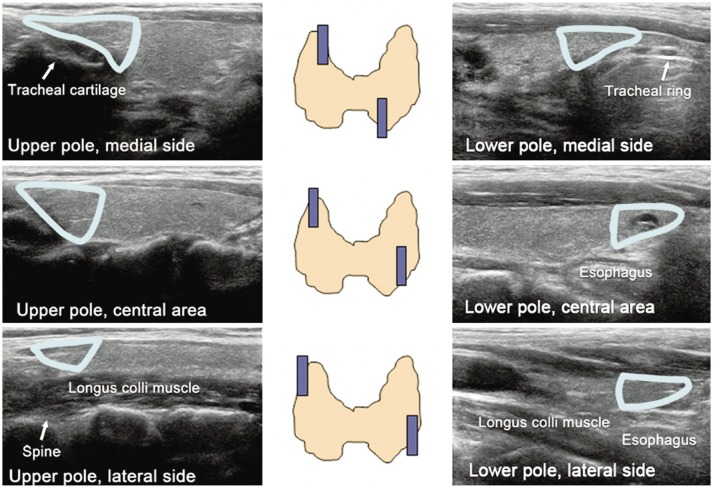
"Satisfaction of search (SOS)" is a subset of under-reading errors (false-negative responses) and it occurs when one or more lesions remain undetected after the detection of others (20). In thyroid US, when multiple nodules are seen on US, some nodules might be missed (Fig. 5). Commonly overlooked sites are the four tips of the thyroid upper and lower poles. To avoid error, the US technician must examine the thyroid gland from tip-to-tip in its entirety, while paying special attention to each tip's triangular shape (Fig. 6). This is particularly important for novices; using a checklist form is recommended to avoid SOS errors.
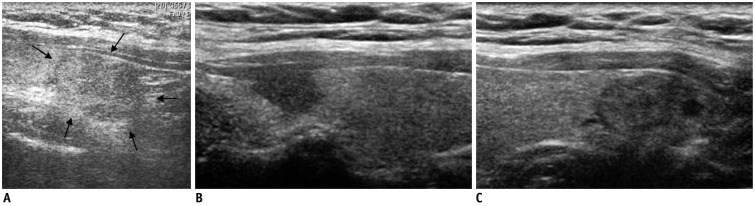 | Fig. 5Satisfaction of search in 51-year-old man with benign nodule.
A. Outside ultrasonography showed nodule (arrows) in right thyroid lobe. B, C. However, another suspicious nodule was detected at tip of right upper pole. Lesion in upper pole was surgically confirmed to be papillary carcinoma, but lesion in lower pole was confirmed to be adenomatous hyperplasia.
|
Go to :
Pitfalls Associated with Anatomy
There are several normal structures within the neck that may influence examination and can potentially mimic pathologic lesions. The first structure of issue is: the echogenic septum within the thyroid gland (Fig. 7). This septum makes a posterior shadow resulting in a posterior dark region that may resemble a hypoechoic lesion. In patients with Hashimoto thyroiditis, echogenic septa may be the cause of multiple hypoechoic lesions termed pseudo-nodules (8). When these septa are visualized, it is imperative to turn the transducer and confirm the lesion on both transverse and longitudinal scans.
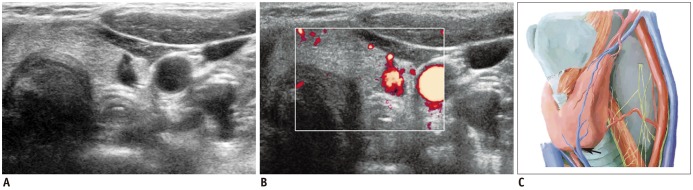
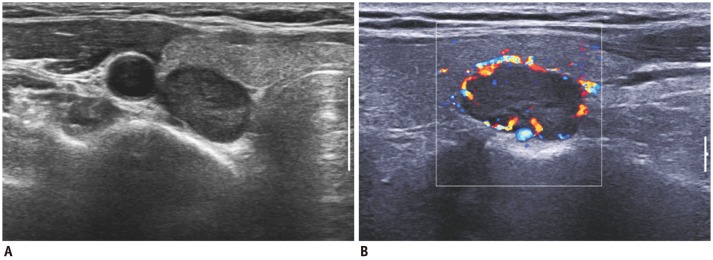
The second normal structure often mistaken for a pathologic lesion is the blood vessel. The thyroid gland is supplied by superior and inferior thyroid arteries and drains into superior, middle, and inferior thyroid veins. The superior thyroid artery primarily supplies the anterior aspect of the thyroid lobe, while the inferior thyroid artery supplies the posterior aspect. In some patients, these vascular structures mimic a suspicious elongated nodule at the posterior aspect of the thyroid gland (Fig. 8). Occasionally, the inferior thyroid artery or vein appears like a nodule on US (Fig. 9). In these cases, color Doppler images with graded compression become useful in ruling out vascular structures.
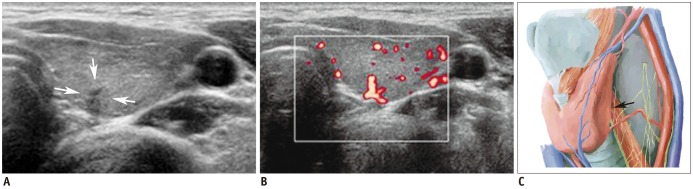 | Fig. 8Vascular structure mimicking thyroid nodule.
A. Irregular, taller-than-wide, hypoechoic lesion (arrows) was seen at posterior aspect of left mid thyroid pole. B. Color Doppler scan revealed vascular structure. C. Vascular structure likely arose from inferior thyroid artery (arrow). Spectral wave form on Doppler scan would help confirmation.
|
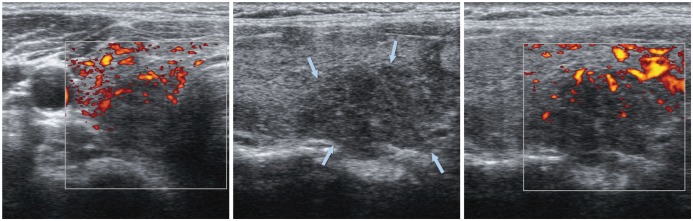
Finally, the transverse vertebral processes of the cervical spine or a cervical rib may also present opportunity for misidentification by mimicking calcified jugular chain lymph nodes. These structures show up as echogenic lesions with an intense posterior shadowing on US (Fig. 10). This diagnostic dilemma may be particularly important in patients who have previously undergone thyroidectomy for thyroid cancer. According to previous reports (21, 22), intranodal calcifications have been noted in 46% to 69% of metastatic lymph nodes from thyroid papillary carcinoma (Fig. 11). Intranodal calcifications may also be seen in tuberculosis, sarcoidosis, treated lymphoma, and following radiation or chemotherapy (21-23). Thus, the US technician should be alert to these similarities, and attempt to differentiate the transverse processes from metastatic lymph nodes when evaluating the lateral neck. In this instance, however, if the examiner were to perform FNAB of the transverse process, normal soft tissue smears would result (24).
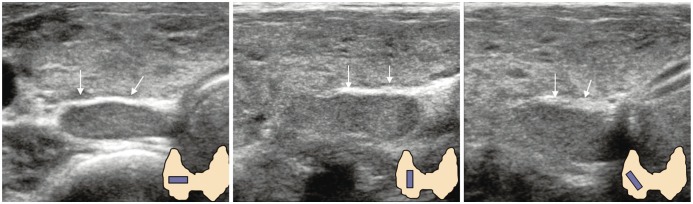
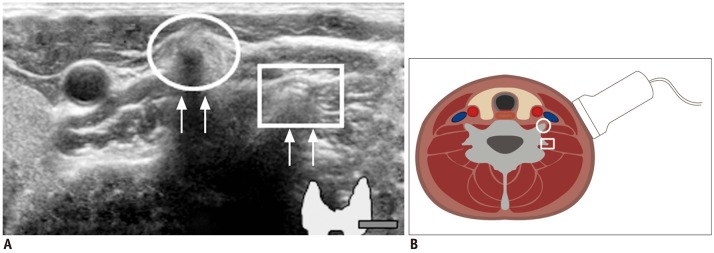 | Fig. 10Prominent vertebral transverse process mimicking calcified lymph nodes.
A. Circle indicates anterior tubercle of transverse process and square identifies posterior tubercle. Echogenic line (arrows) suggested vertebral cortex. B. Sectional diagram provides more detailed explanation.
|
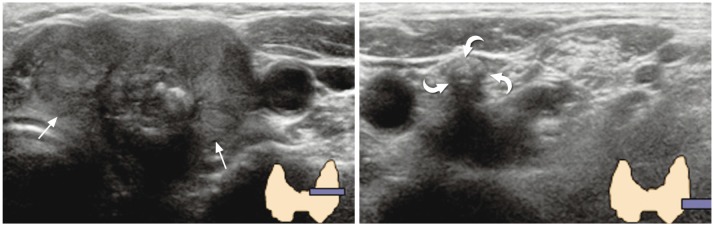 | Fig. 11
Dense calcified lymph node mimicking vertebral transverse process. 69-year-old woman was referred to our hospital for diagnosed thyroid cancer (arrows). During preoperative thyroid ultrasonography, dense calcification (curved arrows) was visible at left level IV region. It was initially confused with vertebral transverse process, but was finally determined to be metastatic lymph node.
|
Go to :
Pitfalls Associated with Interpretation
Myriad criteria have already been established for differentiating benign thyroid lesions from malignant lesions (6, 25-29). One of the well-known findings associated with thyroid cancer is microcalcification associated with psammoma bodies. This proves to be an important diagnostic factor because of its high specificity (1, 29, 30). Although microcalcification is often confused with colloid crystal as both are seen as echogenic dots on US, a follow-up with US alone is sufficient in an anechoic cyst with the characteristic "comet-tail artifact" (Fig. 12) (31).
 | Fig. 12
Typical comet-tail artifact in benign colloid cyst. 58-year-old woman who had undergone mastectomy for breast cancer was presented for screening thyroid ultrasonography. Small cyst containing echogenic spot with comet-tail (arrows) was identified. This is typical case of "comet-tail artifact" caused by colloid crystals.
|
Certain types of thyroiditis may be misdiagnosed as thyroid malignancy: in particular, subacute and chronic lymphocytic thyroiditis. Park et al. (32) reported the presence of ill-defined hypoechoic lesions without a discrete round to oval shape as a US finding associated with subacute thyroiditis and that clinically, subacute thyroiditis was also associated with painful neck swelling and/or fever (Fig. 13). The thyroiditis tend to show geographical changes on different US views unlike true focal masses and some patients may have a recent upper respiratory infection history (32). Langer et al. (33) reported that focal thyroiditis is associated with solid hyperechoic nodules with ill-defined margins. Some of these nodules are seen as ill-defined, irregular, geographically patterned hypo- to marked hypo-echoic lesions with relatively decreased vascularity compared to surrounding tissues (Fig. 14). These lesions may mimic malignancy; thus, further work-up is warranted. However, results of FNAB are typically consistent with benign lesions such as benign follicular cells being found with or without the presence of macrophages.
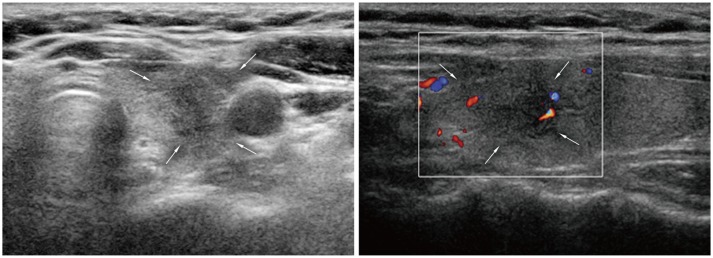 | Fig. 13
Subacute thyroiditis. 48-year-old woman was referred for suspicious left thyroid lesion. Ultrasonography revealed irregular hypoechoic mass (arrows) in her left upper pole. Vascularity was noted at some peripheral areas on color Doppler imaging. Patient had experienced neck pain within past several weeks. Fine needle aspiration biopsy was performed and confirmed subacute thyroiditis.
|
 | Fig. 14
Focal lymphocytic thyroiditis. 40-year-old woman underwent thyroid US for evaluation of hypothyroidism. Suspicious hypoechoic lesion (arrows) was seen in mid pole of right thyroid lobe. However, lesion was confirmed to be lymphocytic thyroiditis by US-guided fine needle aspiration biopsy. US = ultrasonography
|
Go to :
Pitfalls Associated with Extrathyroidal Abnormalities
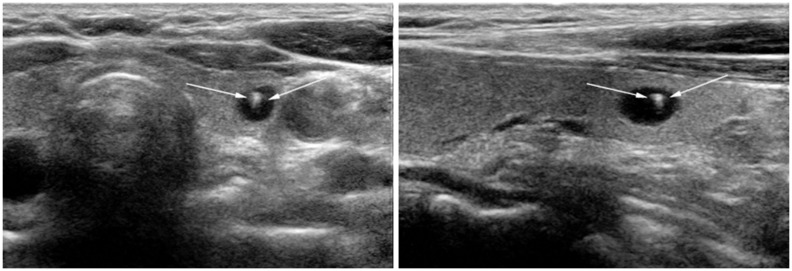
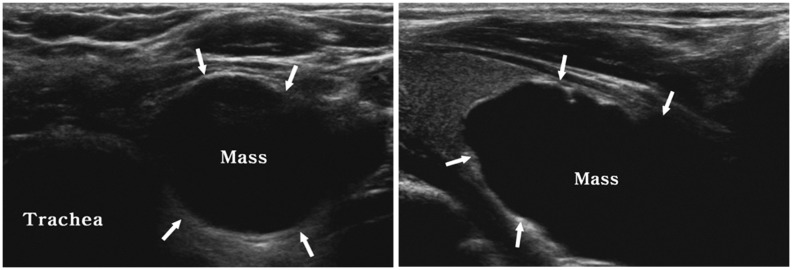
A well-known example of an extrathyroidal lesion masquerading as thyroid pathology is a small pharyngoesophageal diverticulum. It has the appearance of a hypoechoic mass with internal echogenic dots on US; thus, it is often misdiagnosed as a suspicious nodule (Fig. 15). However, the shape of diverticulum may change by peristalsis during scanning (12). Rarely, a paratracheal air cyst may also mimic a suspicious thyroid lesion. Indeed, it is similar in appearance to a pharyngoesophageal diverticulum but is usually located near the right inferoposterior aspect of the thyroid gland with a narrow stalk (Fig. 16) (12, 34). A third structure also commonly seen is the parathyroid lesion. Although the normal parathyroid gland is not typically seen on US, parathyroid lesions such as hyperplasia, adenomas or cysts may be seen near the posterior or inferior aspect of the thyroid gland (Fig. 17). Typically, the parathyroid adenoma appears as a well-circumscribed, round or oval, hypoechoic nodule. Not frequently, the parathyroid adenoma may develop cystic degeneration and contain calcifications (Fig. 18), and if this type of pathology is also present, it may lead to misdiagnosis (14, 15).
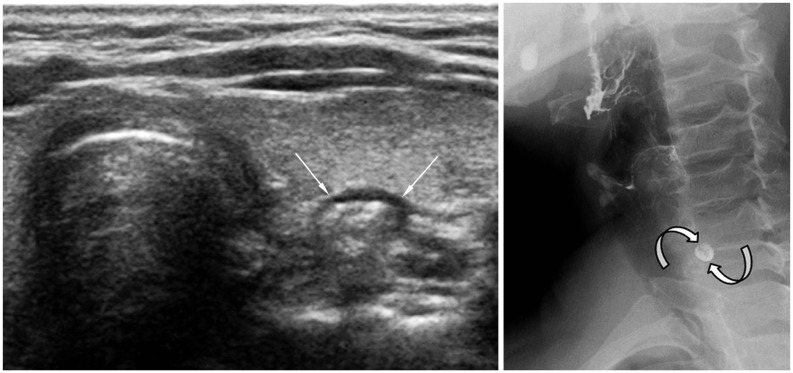 | Fig. 15
Pharyngoesophageal diverticulum. 63-year-old woman was referred for evaluation of left thyroid nodule. High-resolution ultrasonography revealed pharyngoesophageal diverticulum (arrows). Small barium collection (curved arrows) suggesting diverticulum was visible on esophagography.
|
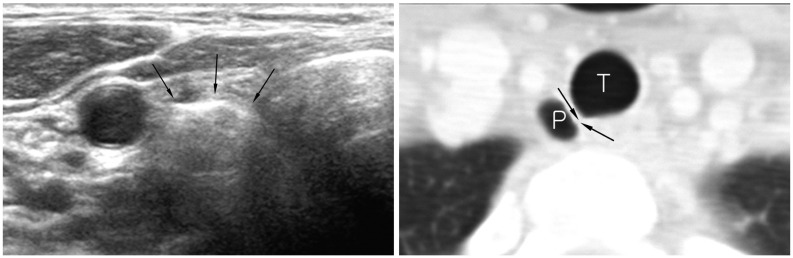 | Fig. 16
Right paratracheal air cyst in 47-year-old woman. Screening ultrasonography revealed echogenic mass (arrows) suggestive of air-containing mass in right paratracheal region. Neck CT scan was performed and confirmed presence of right paratracheal air cyst with slit-like communicating channel (arrows). P = paratracheal air cyst, T = trachea
|
Go to :
CONCLUSION
In conclusion, the diagnostic performance of thyroid US can be limited by various imaging pitfalls associated with US techniques, performance, and misinterpretation of normal structures, or non-thyroidal lesions. A familiarity of these pitfalls may help clinicians and patients avoid further unnecessary evaluation and misdiagnosis.
Go to :
 XML Download
XML Download