

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Double aortic arch with atretic left arch distal to the origin of left subclavian artery (LSCA) is a rare type of vascular ring, and it can be easily confused with the more common type of vascular anomaly, right aortic arch with mirror branching. We present two pediatric cases with this type of vascular ring and images from multi-detector row computed tomography (MDCT), which accurately disclosed the anatomic structure.
CASE REPORT
Case 1
The first patient was a 16-year-old girl who presented difficulty swallowing, which had persisted for 3 years. Barium esophagography (Fig. 1A) revealed posterior indentation of the middle esophagus so MDCT was arranged to delineate the anatomical details of the aortic arch.
The scan was done with a 40-detector-row CT scanner (Brilliance 40; Philips, Best, the Netherlands) according to a protocol published in the literature (1). The scan was interpreted on a dedicated MDCT workstation (Extended Brilliance Workspace; Philips, Best, the Netherlands).
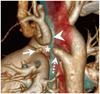
Multi-detector row computed tomography imaging study disclosed apparent right aortic arch with ascending aorta giving origin to a left innominate artery as first branch, which was followed by right common carotid artery and right subclavian artery (RSCA), and a blind-end diverticulum arising from descending aorta (D-aorta) with tip toward the left side (Fig. 1B). A small protruding pouch was also noted over proximal left pulmonary artery. Proximity of the small pouch over pulmonary artery, descending aortic diverticulum, and posterioinferiorly distorted LSCA on CT suggested presence of fibrous tissue connecting these three structures.
Fibrous cord between LSCA and descending aortic diverticulum was confirmed during the surgery, and thus, the double aortic arch with left arch atresia distal to the origin of LSCA (distal left arch atresia) was the final diagnosis rather than the right aortic arch with mirror branching. In addition, left ligamentum arteriosum arising from the small pouch to the fibrous cord was also noted. The surgeons transected both the fibrous cord and ligamentum arteriosum to separate the proximity. After the operation, no specific complications occurred and the patient reported that food swallowing was improved. The follow-up MDCT one year later revealed upward migration of the LSCA without inferior tethering to descending aortic diverticulum, which meant that the ring comprising the "double aortic arch" was no longer present, thereby releasing the trachea and esophagus (Fig. 1C).
Case 2
The second patient was a 3-year-old girl who suffered from failure to thrive and had recurrent respiratory infections. Results of barium esophagography suggested evidence of vascular ring.
Multi-detector row computed tomography was conducted with similar settings to those used with the first patient (1), and the same vascular anomaly was revealed with a more significant anatomic continuity among the LSCA, descending aortic diverticulum, and pouch over pulmonary artery. Furthermore, compressed trachea and esophagus were also revealed after post-processing with volume rendering (Fig. 2). Double aortic arch with distal left arch atresia was diagnosed, and the small pouch over pulmonary artery suggested a ductal diverticulum.
DISCUSSION
The arch anomaly described here - double aortic arch with an atretic left aortic arch distal to the left origin of subclavian artery - is rare (2), and a few cases were revealed by echocardiography combined with angiography or magnetic resonance imaging (MRI) alone (2-4). One case was diagnosed by MDCT in a recent article (5). Our cases provide further pre- and post-operative CT images for comparison and demonstrate the value of MDCT in diagnosis and follow-up. A vascular ring may be diagnosed by barium esophagography, echocardiography, conventional angiography, MRI, and computed tomography. However, MDCT is a superior imaging modality as it provides more detailed information, including vascular structures and spatial relationships to adjacent organs, especially the airways (5). MDCT combined with various post-processing options, such as volume rendering, maximum intensity projection, and multiplanar reformations can delineate details in the compressed trachea, esophagus, and the vascular ring, even in cases in which the ring comprises atretic aortic arch and ligamentum arteriosum (5).
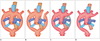
According to the Edward's hypothetic double aortic arch system, aortic arch anomaly is caused by failure of regression, or regression at an abnormal site of the fourth aortic arch (6). Vascular ring may be caused by anomalies of the aortic arch and pulmonary artery. The most common forms are double aortic arch and right aortic arch with aberrant LSCA (Fig. 3A, B), and the less common forms are anomalous innominate artery, anomalous RSCA, and pulmonary sling (4, 7). Sometimes a portion of double aortic arch may be atretic with formation of a fibrous cord, and the vascular structure has the appearance of right aortic arch with mirror branching (Fig. 3C, D), which does not typically comprise a complete vascular ring (2), resulting in delays of surgical correction.
The application of MDCT imaging with volume-rendering enabled the authors to distinguish double aortic arch with atretic left arch from other aortic arch anomalies. Evidence of an inferior convexity of the LSCA and a descending aortic diverticulum suggested the presence of an imperforate vessel or fibrous cord connecting the structures. In our cases, pre-operative imaging by MDCT was proven to be highly accurate and provided valuable information which facilitated surgical planning. In addition, MDCT was used to confirm change in post-operative vascular structure with significant improvements at the 1-year follow-up.

 XML Download
XML Download