

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Progressive enlargement of a multinodular thyroid goiter can compress the trachea and thus cause airway obstruction symptom (1).
In numerous clinical reports (2-5), researchers have demonstrated their clinical experiences with tracheal stent placements for the palliation of tracheal stenosis in patients with thyroid goiter. Tracheal stenting can provide symptomatic relief of patients' respiratory problems, and can thus allow the medical staff to perform other therapeutic or palliative curative measures such as thyroidectomy or laser treatments (2-4). However, complications such as stent migration, sputum retention or granulation tissue formation through the stent meshes or at either ends of the stent limit the effectiveness for long-term placement of airway stents (6, 7).
Radiofrequency (RF) ablation is reported to be a valid and safe approach for the treatment of benign thyroid nodules with pressure symptoms (8, 9). However, ablated thyroid nodules only slowly decrease in size after several months or years (9), and edema and resulting volume increase can occur immediately following RF ablation (10, 11).
We report the case of an elderly male who successfully underwent tracheal stent placements for respiratory distresses, and then, subsequent RF ablation for thyroid volume reduction. This sequential treatment then allowed elective stent removals for this patient with thyroid goiter with tracheal stenosis after the RF ablation.
Go to : 
CASE REPORT
An 80-year-old man was presented with acute onset of dyspnea associated with cough and sputum. He had suffered from a thyroid goiter for 50 years, although it was non-toxic and growing very slowly. Intermittent dyspnea had begun 10 years earlier and had worsened during the previous week. The patient complained of dyspnea while resting when he was seen in our Emergency Department. He had not undergone previous treatments for his thyroid goiter (Fig. 1A). CT scans (Fig. 1B) obtained on his first admission showed remarkable narrowing of the tracheal lumen caused by enlarged bilateral thyroid glands. The narrowest diameter of the stenosis was 5.8 mm.
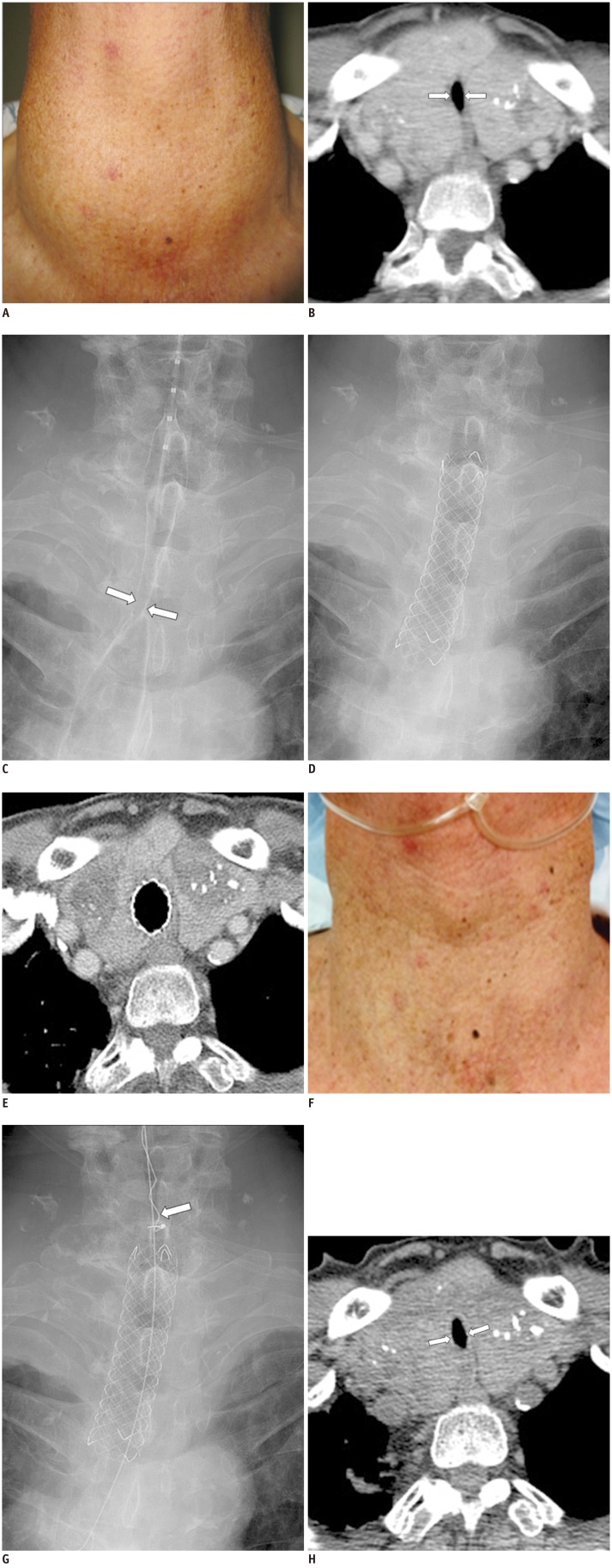 | Fig. 1Tracheal stenting and radiofrequency ablation for thyroid goiter.
A. At time of patient's admission, photograph (A) shows diffuse swelling on neck. Axial CT scan (B) shows stenotic tracheal lumen (arrows) caused by enlarged thyroid lobes with internal nodules and calcifications. C, D. Placement of retrievable, self-expandable and silicone-covered with barbed metallic stent to relieve dyspnea. Radiograph (C) obtained after contrast injection through 5 Fr catheter shows stenotic tracheal lumen (arrows). Radiograph (D) obtained immediately after stent placement shows well-expanded stent. Two radiofrequency ablation sessions were performed one and six weeks, respectively, following stent placement (not shown). E-G. CT scan (E) and photograph (F) obtained four weeks following second radiofrequency ablation session, shows reduction of thyroid volume. Stent was removed by using retrievable hook (arrow) (G). H. Follow-up CT scan obtained five weeks following stent removal shows stable maintenance of reduced thyroid volume and slightly widened tracheal lumen (arrows) as compared with initial CT scans obtained before stent placement.
|
To relieve his severe dyspnea, a self-expandable stent was placed in the stenotic trachea (Fig. 1C, D). The normal diameter of the adjacent trachea was 18 mm and the stricture length was 6 cm; therefore, we chose a stent with diameter of 18 mm and length of 8 cm. According to our specifications, the stent was designed to be retrievable, self-expandable, and silicone-covered with barbed metallic (S&G Biotech, Seongnam, Korea). The metal used for the stent was nitinol. The stent had a retrievable design for elective removals when it was no longer necessary or if there were stent-related complications.
Two RF ablation sessions were then performed one and six weeks following stent placement and for which we used an 18-gauge, 1-cm, active-tip, internally cooled electrode (VIVA, STARmed, Goyang, Korea). On the basis of our previous clinical experiences (11, 12), an ultrasound-guided, trans isthmic approach was used to insert an electrode along the short axis of the nodule, and all nodules were then managed by using the moving shot technique. With the moving shot technique, multiple, small, conceptual ablation units are ablated unit-by-unit by moving the electrode (10-12). We began ablations with 30 W of RF power. If a transient hyperechoic zone did not form at the electrode tip within 5-10 seconds, the RF power was increased in 10-W increments up to 80 W. The procedure was accepted by our patient, and ablation was terminated when the planned imaginary units were changed to transient hyperechoic zones.
We decided to remove the stent four weeks after the second RF ablation session because the thyroid volume had progressively reduced externally according to follow-up on CT scans (Fig. 1E-G); there was also a concern regarding possible complications, such as stent migration or granulation tissue formation around the stent, resulting from a long-dwelling stent. The last follow-up CT scans (Fig. 1H) obtained five weeks following stent removal showed stable maintenance of the reduced thyroid volume and an apparent narrow tracheal lumen which was, however, relatively wider than that seen on the initial CT scans. The narrowest diameter measured 6.4 mm on the last follow-up CT scans. This report is recorded four months after the stent removel and the patient was able to breathe normally.
Go to :
DISCUSSION
Placement of airway stents is safe and effective in patients with airway obstructions caused by benigns or malignant thyroid diseases (2, 3). Although airway stenting can improve a patient's quality of life due to the immediate reliefs of dyspnea, it is difficult to expect long-term stent durability as stent-related complications because stent migrations or granulation tissue formations are common (6, 7). As the initial treatment, RF ablation for thyroid goiter with compressive symptoms is not appropriate because acute symptom reliefs cannot be achieved. In fact, it has been reported that compressive symptoms can worsen directly after the RF ablation as initial swelling of the thyroid nodule due to percutaneous laser ablation, and was probably caused by thyroid tissue edema (13).
Combination therapy consisting of temporary airway stenting and the RF ablation for thyroid goiter has not yet been reported. It has two definite advantages, one being the immediate reliefs of dyspnea with airway stenting and the other being the reduction of the thyroid volume with RF ablation which allows long-term symptom reliefs even following stent removal. Because the temporary stenting could be combined with radiation/chemotherapy for esophageal or airway malignancy (14, 15), temporary airway stenting with concurrent RF ablation may be an effective palliative treatment for thyroid goiters as resolutions of the dyspnea may be expected to delay and prevent stent-related complications. RF ablation could thus become important for achieving long-term reliefs of compressive symptoms as the thyroid volume could then be substantially reduced (8, 9, 11, 16).
This kind of combination therapy is expected to be very useful in patients presenting symptoms of definite dyspnea, however, it is difficult to predict the benefits of tracheal stenting in combination with RF ablation when patients with thyroid goiters have no respiratory symptoms. We, therefore, assume that tracheal stent placements could be delayed until the patient's symptoms actually surface.
In our patient, the last follow-up CT scans obtained nine weeks after the second RF ablation session, i.e., five weeks following elective stent removals, showed a slightly widened tracheal lumen as compared with that seen on the initial CT scans obtained before the treatment. Although narrowing of the trachea was still observed, it seemed to be stable because the patient experienced no dyspnea in his daily routine life, and further tracheal narrowing was not expected as the overall thyroid volume was decreased.
This type of combination therapy can also be used for patients with inoperable thyroid malignancy of airway obstructions. Because the RF ablation can result in tumor volume reductions secondary to the destruction of thyroid cancer cells (17), long-term palliation is expected with the use of a combination of airway stenting and RF ablation for inoperable thyroid malignancy.
Go to :
 XML Download
XML Download