

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The anterior commissure (AC) and posterior commissure (PC) are two dominant anatomic structures serve as indirect localization of intracerebral anatomy. The intercommissural line has also been used as a reliable reference line for stereotactic surgery. Rapid advancement of neuroimaging techniques made possible for the detailed analyses of the anatomic structures of AC and PC. Also with the use of ultra-high field MRI such as 7.0T MRI, the sizes and shapes of the AC and PC are now clearly visible, and it appears possible to quantify the individual differences (1, 2). Due to these technological advances, the previous descriptions of AC and PC are become obsolete and needs a revisit for the updated definition.
It is understood that the availability of an accurate standard intracerebral reference line for overall neuroanatomy will enhance the standardization of image interpretation of any given section of the brain so that the information obtained can be compared easily. Moreover, such information will be more helpful during stereotactic surgery. Several studies have investigated the strcutres of AC and PC previously, however, the present was based on the images obtained from the conventional MRI system, such as 1.5T or 3.0T MRI, which was rare in the literature (3-5).
The objective of the present study was to analyze the anatomic variation of the AC and PC using a 7.0T MRI and standardization of the reference line for the use in conventional neuroanatomic practice as well as indirect intracerebral localization.
Go to : 
MATERIALS AND METHODS
Subjects and Equipment
Thirty-four cases (21 males and 13 females with an average age of 25 and 23 years, respectively) of healthy volunteers were enrolled in this study. The study was approved by the Gachon Gil Hospital IRB and the Korea Food & Drug Administration. Magnetic resonance imaging (MRI) scanning was performed with a Siemens 7.0T MRI (Magnetom; Siemens, Enlargen, Germany) scanner using an 8-channel TX-RX head coil. A conventional 1.5T MRI was used for comparison purposes.
Image Data Acquisition Method
Prior to obtaining the general picture and MRI images two markers were attached to the face of the subject. One marker was on the lateral canthus and the other marker was on the center of the external auditory meatus as the reference points for the canthomeatal line (CML). Each volunteer was asked to sit comfortably and look to the level of his/her eye. A picture was taken on a flat ground to obtain a horizontal reference line (Fig. 1A).
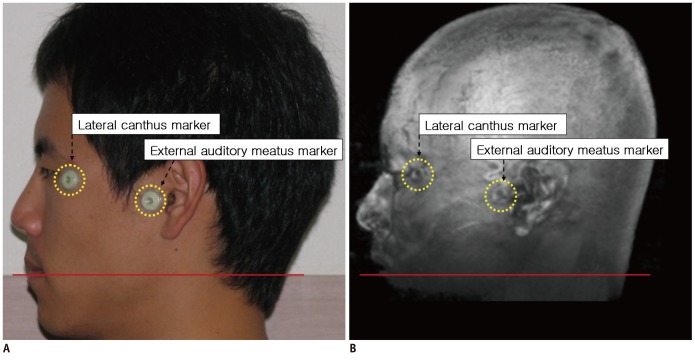
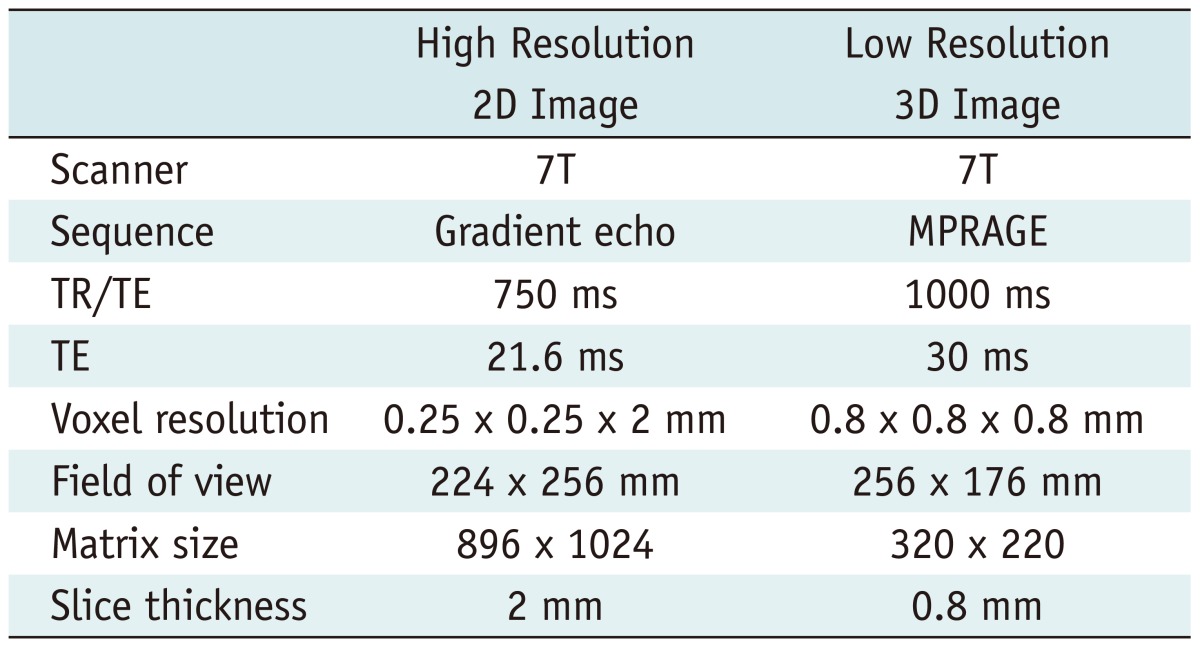
The main MR imaging was the sagittal T2* weighted 2D high resolution image which were used for the analysis of the shape and position of the AC and PC. Volunteers were asked to fix the head position during scanning which took about 1 hour to obtain a high resolution midsagittal image. The central brain area showed that the AC and PC were scanned first. Additionally, a 3D T1 weighted imaging was carried out to observe the head structure. This image was taken at the same head position with that of the previous imaging to compare the position of the brain and head together. Figure 1B shows an example of the T1 MR image after rendering with markers. For the surface image, low resolution magnetization prepared rapid gradient echo imaging sequence was chose to cover the whole brain. The MR imaging parameters that were used in the study are summarized in Table 1.
Go to :
RESULTS
The Anterior and Posterior Commissures Using 1.5T and 7.0T MRI
Under normal circumstances using 1.5T MRI, both the AC and PC are seen as blurred, round structures with poor delineation in the midsagittal section. The outlines are usually severely blurred and cannot be delineated accurately. One can barely determine the centers of the AC and PC (Fig. 2A). In contrast, the mid-sagittal slice of the 7.0T MRI showed AC as a small island. Similarly, the PC image on 7.0T T2* also showed structures which appear as denoted as C in Figure 2B. The PC is generally C-shaped and its boundary could also be easily identified, except the upper and lower ends that are not as distinct as the AC. Therefore, we set the PC as a "C-shaped" object between the pineal recess and the mesocoelic recess, as shown in Figure 3B. The curvature and direction of the C varies slightly, however, the upper and lower ends can always be easily identified. Additionally, it was interesting to note the mesocoelic recess was more clearly developed in some individuals.
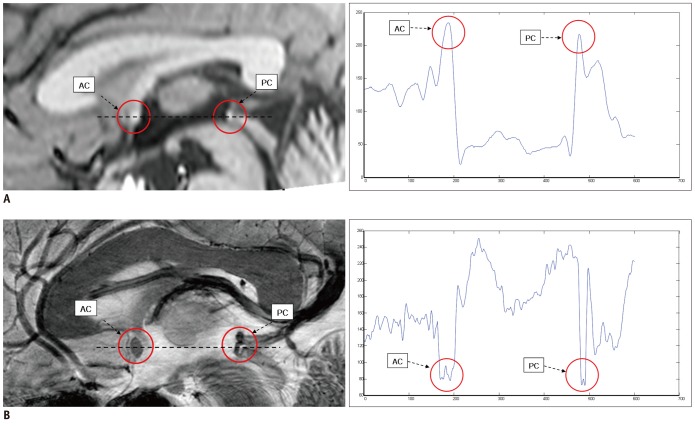 | Fig. 2Comparison of AC and PC in 1.5T and 7.0T images (sagittal view).
A. 1.5T image with central commissural line (black dotted line) and intensity plot (blue solid line). B. Same as (A) with 7.0T image. AC and PC are circled in sagittal views of both 1.5T and 7.0T MRI images. Note clear AC and PC contrast and edge in 7.0T image. AC = anterior commissure, PC = posterior commissure
|
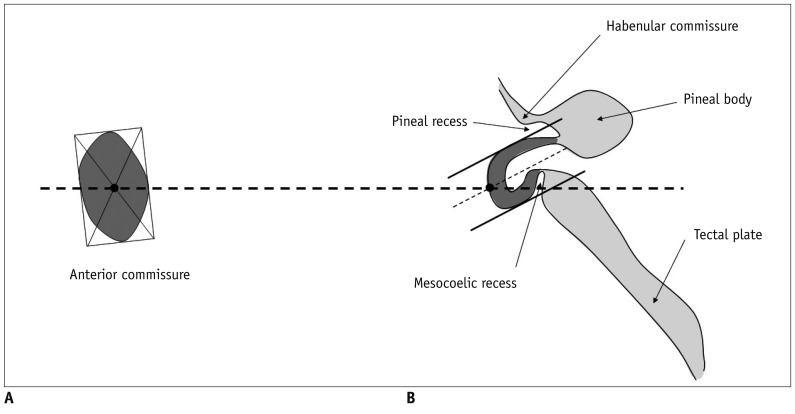
Determination of the Center of the AC and PC
Determination of the center of the AC and PC is required to draw a line connecting the AC and PC and to measure the distance between the AC and PC. The center of the AC was determined by the point of intersection of two diagonal lines of the squares around the AC, as seen in Figure 3A. For the PC, the midpoint of the entire outlined length of the PC from the pineal recess to the mesocoelic recess is set at the center of the PC. The distance between the AC center to the PC center was defined as the intercomissural distance, as shown in Figure 4. The connecting line between the AC center and the PC center was defined as the central intercommissural line (CIL), instead of the intercommissural line as it was usually defined before. The average central intercommissural distances measured were 2.54 cm in males and 2.42 cm in females in the current study.
Measurements of the AC and PC
Since AC is an oblong shape directed superoinferiorly, the superior-inferior axis is the long axis of the AC and the anterior-posterior axis of the AC is a short axis. The long axis of the AC is slightly shorter in males than females (0.44 ± 0.07 cm vs. 0.48 ± 0.06 cm). However, the short axis of the AC showed no difference among the subjects. The ratio of the long axis to the short axis is 1.73 ± 0.19 in males and 1.92 ± 0.32 in females. The angle between the AC-PC axis and the long axis of the AC is not orthogonal, but is slightly tilted anteriorly by 103.4 ± 4.6 degrees in female and 99.5 ± 6.2 degrees in male (Fig. 4).
Comparison of the Intra- and Extra-Cerebral Reference Lines
Since many intra- and extra-cerebral reference lines are used in radiology practice, we compared these reference lines by measuring the differences in the angle from the horizontal line. First, we measured the angles between the horizontal line and the CIL. The CIL was 8.7 ± 5.1 degrees in males and 11.0 ± 4.8 degrees in females in reference to the horizontal line. Secondly, the tangential intercommissural line (TIL), the most commonly used reference line connecting the upper edge of the AC and the lower edge of the PC, is drawn as shown in Figure 5B. The TIL had a 17.4 ± 5.2 degree difference in males and a 19.8 ± 4.9 degree difference in females in reference to the horizontal line. Another reference line is the corpus callosum line (CCL), which connects the lower borders of the genu and the splenium of the corpus callosum, as shown in Figure 5C. It is similar to the horizontal line. However, we found that the CCL varies considerably by different subjects with a large standard deviation (Fig. 6B).
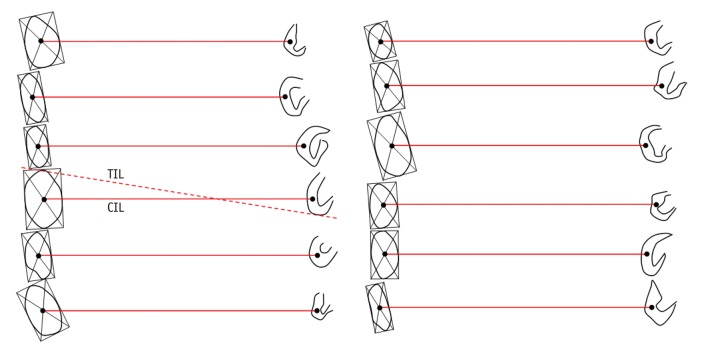
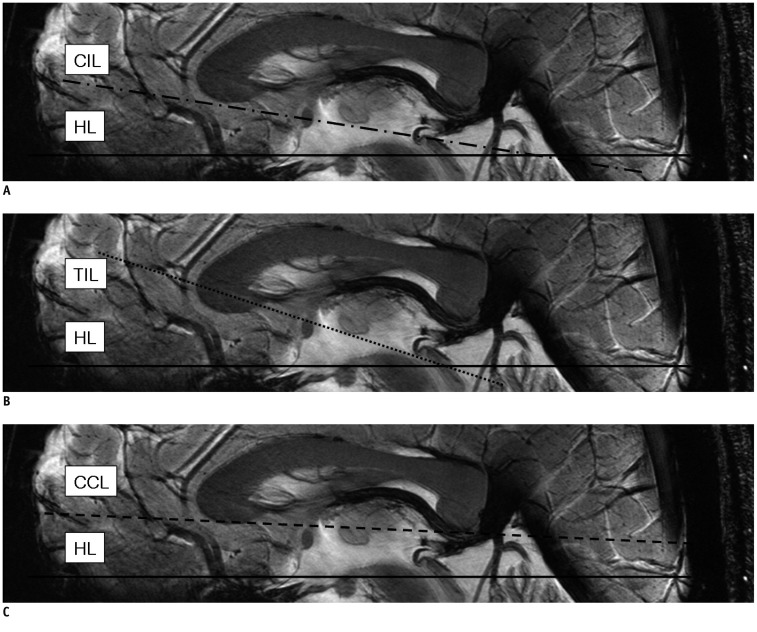 | Fig. 5Various intercommissural and extended cerebral reference lines in reference to horizontal line (HL : solid line).
A. Central intercommissural line (CIL : dash-dot line). B. Tangential intercommissural line (TIL : dotted line). C. Corpus callosum line (CCL : dashed line). CCL = corpus callosum line, CIL = central intercommissural line, HL = horizontal line, TIL = tangential intercommissural line
|
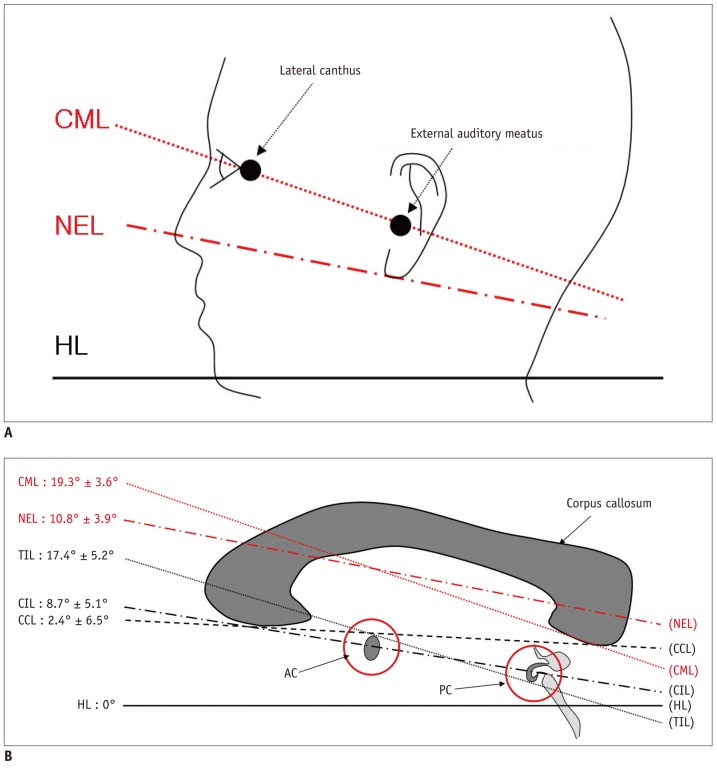 | Fig. 6Extracerebral & intracerebral reference lines in reference to horizontal line.
A. Extracerebral reference lines : nose-ear line (NEL : red dash-dot line), canthomeatal line (CML : red dotted line) all in reference to horizontal line. B. Summary of result in case of male. AC = anterior commissure, PC = posterior commissure, CCL = corpus callosum line (black dashed line), CIL = central intercommissural line (black dash-dot line), CML = canthomeatal line (red dotted line), HL = horizontal line (black solid line), NEL = nose-ear line (red dash-dot line), TIL = tangential intercommissural line (black dotted line)
|
Among the extracerebral reference lines, the CML has long been the standard reference line. The CML has a 19.3 degree difference in reference to the horizontal line. We compared this extracerebral reference line to our intracerebral CIL and measured the difference in the angle between the CIL and CML, which was 10.1 ± 4.0 degrees in males and 10.1 ± 3.0 degrees in females. Thus, the CML has a fairly consistent difference in angle from the CIL by approximately 10 degrees (Fig. 6B).
We also attempted to identify the extracerebral reference line that is parallel to the intracerebral reference line (the CIL) in the same brain, a line connecting the nasal tip and the lower border of the ear lobe, designated as the nose-ear line (NEL), was shown to be closest to the intracerebral reference line, the CIL (Fig. 6A). The NEL had a 10.8 degree difference in reference to the horizontal line. This NEL had a difference in angle from the CIL by 2.2 ± 3.3 in males and 0.4 ± 2.0 in females.
The line connecting the borders of the AC and PC are designated as the TIL. This TIL has long been used among neurosurgeons and neuroscientists using the atlases of Talairach and Tournoux et al. (6) and Schaltenbrand et al. (7). The angle between the CIL and TIL was approximately 8.5 degrees in the current study.
The Distance of the Whole Brain
We set extended central lintercommussural line as E-CIL and extended orthogonal central intercommissural line as E-OCIL (Fig. 7). The distance of the E-CIL was measured extending the CIL to the entire length of the brain on the midsagittal section. The E-OCIL was based on orthogonal CIL axis and measured from the most superior point of the brain to the junction between the medulla oblongata and the spinal cord.
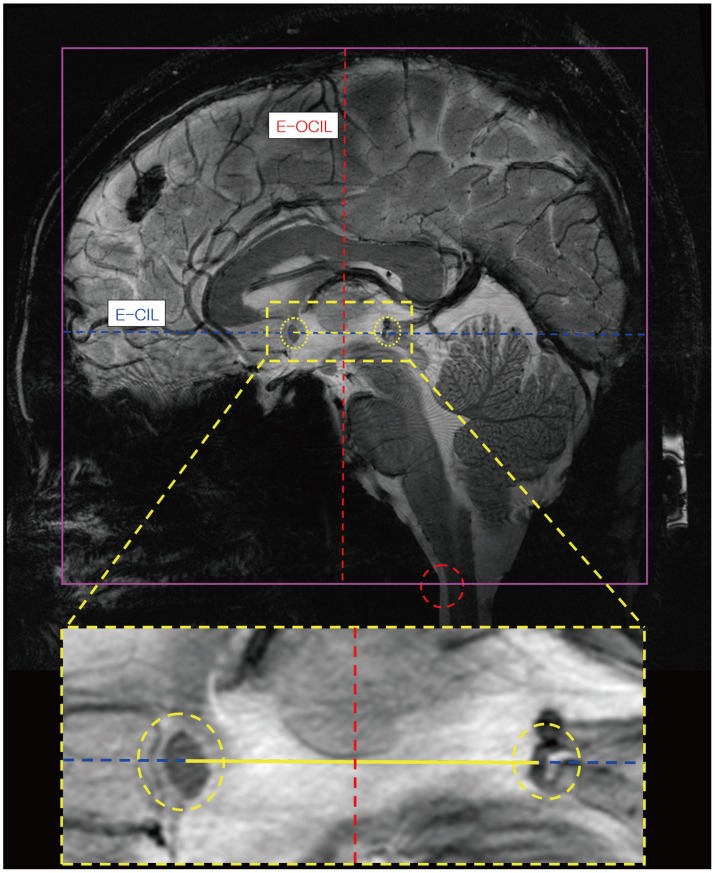 | Fig. 7Definition of virtual extension lines: Blue dotted line indicates extended central lintercommussural line.
Yellow line at middle indicates anterior commissure-posterior commissure connecting line and red dotted line is extended orthogonal central intercommissural line. Two yellow circles show AC and PC points. Red circle is reference point of inferior brain part. AC = anterior commissure, PC = posterior commissure
|
The average AC-PC distance of the brain in this series was 2.49 cm. The average ratio between anterior-posterior extension of the CIL and AC-PC distance was measured to be 6.19 and the average ratio between height of the brain from the parietal to the medullo-spinal cord junction and AC-PC distance was 5.76. If a square is drawn around the extent of the brain, a rectangle is generated. The results of our case study are summarized in Table 2.
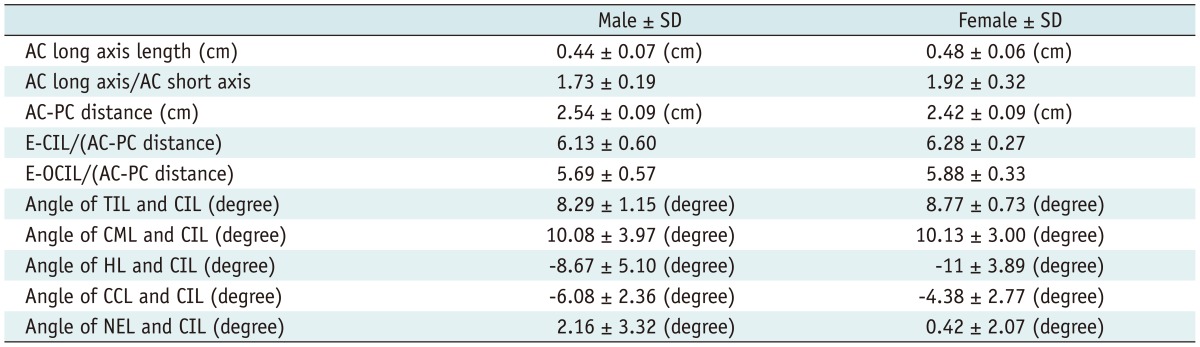
Table 2
Summary of All Analyzed Result
Note.- AC = anterior commissure, PC = posterior commissure, CCL = corpus callosum line, CIL = central intercommissural line, CML = canthomeatal line, E-CIL = extended central intercommissural line, E-OCIL = extended orthogonal central intercommissural line, HL = horizontal line, NEL = nose-ear line, TIL = tangential intercommissural line
![]()
Go to :
DISCUSSION
Both the AC and PC are well known and consistent anatomical structure of the brain, and easy to visualize with existing MRI systems, such as 1.5T or 3.0T. Since the AC and PC are located in the front and back of the deep brain, respectively, and are a significant distance apart, they have been utilized as various reference structures for the indirect localization of the brain, particularly for stereotactic surgery. However, instead of the AC and PC, neurosurgeons use their borders abutting the third ventricle seen through pneumoencephalogram for the guiding structures to locate the deep brain nuclei, such as the basal ganglia and thalamus (8). The line connecting these two borders is referred to as the intercommissural line, although it is not intercommissural in strict sense due to the fact that this line does not connect the actual AC and PC.
As the resolution of brain images has improved dramatically, various interacerebral structures, including the AC and PC, have became more clearly visible, particularly with ultra high field MRI, such as 7.0T MRI. As shown here, the AC can be so clearly visualized that the boundary and borders can be delineated; therefore, it is easy to determine the center. The PC could also be delineated clearly to see the entire extent. Therefore, the true intercommissural line can now be drawn by connecting the centers of the AC as well as the PC. We designated this line as the CIL which differs from the convention used in stereotaxy and functional MRI. Instead of the CIL, in sterotaxy the TIL that passes through the superior edge of the AC and the inferior edge of the PC was adopted. We have extended the concept of the CIL that is connecting the center of AC to the center of PC. The TIL is difficult to define and unreliable when the image resolution is poor. We found that our CIL is easy to define and independent of the size of the AC and PC.
The center of the AC and PC are determined by crossing the squares made around the AC and the middle point of the C in PC, as shown in Figure 3A and 3B, enabling us to more reproducible measurement of intercommissural distance The which was found to be 2.54 cm in males and 2.42 cm in females in the present study. The male/female difference was statistically significant. Other studies involving the Korean population using pneumoencephalograms reported intercommissural distances of 2.48 cm in males and 2.38 cm in females (5). When compared with Caucasians, the intercommissural distancce was about 2.35 cm in the Talairach atlas and 2.5 cm in other studies (9). Since the intercommissural distance is fairly constant among different races, the midpoint of the AC and PC could serve as the center (zero) point of the Cartesian coordinate, and thereby the axial, coronal, and sagittal images could be displayed based on this reference point (10).
It is conventional to use external landmarks to orient radiologic images of the brain, such as the orbitomeatal and canthomeatal lines. The horizontal plane is parallel to the horizon and is perpendicular to the vertical plane, which is the direction of the gravitational force at the point. In this study we used a horizontal level indicator to set the horizontal plane; it is parallel to the floor level. In radiologic practice, the canthomeatal line has been used more frequently. We attempted to compare these extracerebral reference lines to our central intercommissural line to find the correlation. We found that the CIL had an approximately 10 degree counter clock wise to the CML. The TIL was roughly parallel to the CML, and the CIL was roughly parallel to the NEL. The NEL can be utilized as a rough estimate of the CIL. The CIL had an approximately 10 degree angle difference to the horizontal line.
Conclusion
Here we propose that the CIL as the new reference line for axial brain images. In conclusion, using 7.0T MRI, the AC and PC are defined in a more robust manner and allowed us to draw the intercommissural line passing the exact center of both AC and PC. This CIL is more easily drawn than the previously used TIL. We found that the CIL is a reproducible reference line that can be the standard reference line for the axial images of the human brain, especially when such a high resolution image is available.
Go to :
 XML Download
XML Download