

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Studies have shown that most acute coronary syndromes (ACS) result from the rupture of unstable plaques and subsequent thrombus formation (1, 2). The risk of atherosclerotic plaque disruption and thrombosis is thought to be closely related to plaque composition rather than the severity of an actual luminal stenosis (3-5). Therefore, it is of paramount clinical importance to elucidate the composition of coronary atherosclerotic plaques.
The atherosclerotic plaque imaging is the arterial wall imaging (6, 7). Atherosclerosis is a systemic disease of the vessel wall that occurs frequently in the aorta and in the carotid, coronary and peripheral arteries. The formation and development of the atherosclerotic plaque is at the arterial intima. A number of publications (8-10) showed that vivo and ex vivo MR imaging can characterize the composition of great vessels, such as carotid and aortic atherosclerotic plaques. However, imaging the coronary artery wall with magnetic resonance in vivo is challenging due to the cardiac and respiratory motion artifacts, smaller size and tortuous course. Currently, bright blood technique is usually used in imaging human coronary artery in vivo (11). Although the black blood technique was used in human coronary artery studies in vivo (12-14), only coronary wall thickening could be delineated but the compositions of coronary atherosclerotic plaque were not identified. Poor spatial resolution is another limitation for MRI when identifying coronary atherosclerotic plaque composition in vivo. Ex vivo coronary artery wall imaging eliminates the above mentioned disadvantages. But the studies were minimal and the procedure was complicated, the coronary artery was dissected from heart (15, 16). Recent study demonstrated that ex vivo MRI imaging can classify the human coronary atherosclerotic plaques (17). The general purpose of the present study is to investigate the feasibility and optimize imaging protocol for ex vivo porcine and human coronary artery wall using MRI, thus, potentially directing vivo MR vessel wall imaging techniques for characterizing coronary atherosclerotic plaques.
Go to : 
MATERIALS AND METHODS
Porcine Ex Vivo Heart Specimens and Contrast Agent Preparation
Initially, to derive optimal protocol for ex vivo coronary artery wall imaging, 10 fresh porcine hearts (weighted from 500 g to 750 g) were prospectively studied with MRI on the day of explanation. The study was approved by the institutional animal care committee. The animals had no suspect of atherosclerotic vessel wall changes. Before examination, the heart was flushed with water to clear clots within the chambers and coronary arteries, and then, a three-way tube was inserted into the left main coronary artery through the left coronary sinus and fixed in order to inject the contrast. To null the lumen and improve the contrast between the wall and lumen, 20 mL of diluted MRI contrast medium containing iron-oxide particles ferucarbotran (Resovist®, SPIO, Bayer Schering Pharma, Berlin, Germany) was injected into the LAD via the three-way tube, mimicking black blood technique. The optimal proportion of MR contrast agent and saline solution was 1% vs. 99% (17).
Optimizing MR Imaging Procedure
The porcine heart was imaged by using the SIGNA 1.5T HD MR scanner (GE Medical Systems). To investigate optimal coronary vessel wall delineation, three different surface coils were respectively used as described in Table 1 (temporomandibular surface coil, eight-channel head surface coil and knee coil). The proximal segment of left anterior descending artery (LAD) was placed horizontally. The 3-planar imaging was used for the localization and 3D steady state free precession (SSFP) sequence was used to delineate LAD with repeat time (TR) 7.5 ms, echo time (TE) 3.1 ms, field of view (FOV) 12 × 12 cm, slice thickness 3.0 mm, slice space 1.5 mm, matrix 256 × 192, number of excitations (NEX) 1 (Fig. 1). Before scanning, 10 mL saline solution was injected into the left coronary artery via a three-way tube. Then, 2D spin-echo T1-weighted image (T1WI) with fat saturation was performed respectively with temporomandibular surface coil, eight-channel head surface coil and knee coil using the same parameters (TR 440 ms, TE 21 ms, FOV 12 × 9 cm, slice 2 mm, slice space 0.2 mm, matrix 384 × 256, a resolution in-plane of 313 × 352 um, 3 signal averages). Fat suppression was used to reduce the signals from epicardial fatty tissues. The purpose of using different coil imaging 2D spin-echo T1W1 was to select the coil with the highest SNR image.


Next, 2D spin-echo T1WI was repeated with temporomandibular surface coil and matrix 512 × 512 (same other parameters). The purpose of using 512 × 512 in matrix was to investigate if the SNR and CNR of the images were acceptable on the basis of higher spatial resolution. Lastly, T1WI, proton density-weighted image (PDWI) and fast spin echo T2-weighted image (FSE T2WI) with fat saturation, were performed by using temporomandibular surface coil after MR contrast injection. The orientation of T1WI, PDW and T2WI was coincident. The parameters of T1WI were TR 440 ms, TE 21 ms, FOV 12 × 9 cm, slice 2 mm, slice space 0.2 mm, matrix 512 × 512, a resolution in-plane of 234 × 176 um, 3 signal averages. The parameters of PDW included TR 2000 ms, TE 21 ms, FOV 12 × 9 cm, slice 2 mm, slice space 0.2 mm, matrix 512 × 512, 3 signal averages. The parameters of T2WI were TR 4500 ms, TE 105 ms, FOV 12 × 9 cm, slice 2 mm, slice space 0.2 mm, matrix 512 × 512, 3 signal averages.
Human Ex Vivo Heart Specimens
The study was approved by our institutional review board. The informed consents were available from the relatives of the deceased. The hearts from 8 consecutive autopsy subjects with known coronary artery diseases (8 males aged from 84 to 90 years with a mean age of 86.3 ± 1.4 years, 4 died from malignancy, 3 from infections and 1 with myocardial infarction) underwent the coronary MR examinations. The time interval between patient's death and MR imaging was within 24 hours. The specimen preparation was identical to the modality used for porcine hearts. The imaging protocols were described above, with temporomandibular surface coil and matrix 512 × 512. Although the SNR and CNR with 512 × 512 images in matrix were lower than those with 384 × 256 in matrix (the increase in matrix and spatial resolution will consequentially sacrifice SNR) using temporomandibular surface coil, spatial resolution was remarkably increased and image quality was better than the 384 × 256 in matrix with eight-channel head coil and knee coil. Therefore, we imaged human coronary artery wall with temporomandibular surface coil and 512 × 512 in matrix. After scanning, standard pathological sectioning of human hearts were performed immediately. The proximal 40 mm of the LAD was sectioned into 10 tissue blocks of 4 mm in thickness, and the distance from the tissue block to the bifurcation of the left main coronary artery was recorded to match with MR images. After decalcification, the tissue blocks were embedded in paraffin and prepared for histological examination in sections 4-µm thick. Blocks were stained with haematoxylene and eosin (HE).
Analysis of MR Data
Porcine Hearts
To test the optimal protocol for ex vivo coronary artery wall imaging, the proximal segment of LAD in porcine heart was chosen as a target vessel. Signals of the LAD wall, lumen, surrounded by fatty tissues adjacent to LAD, myocardium of anterior part of interventricular septum and noise were respectively measured. Noise was the standard deviation of air signal intensity. SNR of image, CNR1 between the LAD wall and lumen, CNR2 between the LAD wall and surrounding fatty tissue were respectively calculated. The equations were as follow.



Human Ex Vivo Hearts
To test the delineation of atherosclerotic plaque, the ex vivo human hearts were evaluated. Two experienced radiologist, blinded to the histopathology results, evaluated the original two-dimensional, cross-sectional MR images independently and collectively resolved any differences in reading. Each reader classified the plaque independently twice, 2 months apart, to determine the intra-observer variability. The thickness of the vessel wall and signal of plaque were recorded. The plaques were classified according to the AHA criteria and modified the histological classification by Cai et al. (18-20). MRI cannot distinguish type IV lesion from type V lesion, so they are called type IV-V (lipid, necrosis, fibrosis) lesion. Type IV-V lesions showed high or equal signal intensity on T1WI and PDW, low or equal signal intensity on T2WI. Type VI (sub-acute hemorrhage) lesions showed high signal intensity on T1WI and T2WI. Type VII (calcification) lesions showed signal loss on all three sequences. Type VIII (fibrosis without lipid core) lesions had equal signal intensity on T1WI and high or equal signal intensity on T2WI. For each image location, there were three images (T1WI, PDW, T2WI) available for reviews to determine the lesion type. To decrease dependence on lesion type, MR images of proximal 40 mm of LAD were selected at a 4-mm interval (originally 14-20 images, selected 1 from 2 images). This protocol generated 7 to 10 image locations per LAD that could be compared with histological sections. The histopathologic sections were analyzed by an experienced pathologist who was blinded to the MRI results, and plaques were classified according to the AHA criteria (19, 20). I.e., type IV-V (lipid, necrosis, fibrosis); type VI (hemorrhage); type VII (calcification) and type VIII (fibrosis without lipid core). MRI images and histopathologic sections were matched prospectively in the region of the proximal 40 mm of the LAD. The process of matching images to histopathologic sections used landmarks such as the relative distance from the left main trunk bifurcation, and some morphological features such as vessel shapes and lumen sizes, the location of the LAD branches, as well as calcifications.
Statistical Analysis
For the porcine hearts, comparisons of the SNR, CNR1, CNR2 of T1WI using temporomandibular surface coil, eight-channel head surface coil and knee coil were performed using analysis of variance, with p-value < 0.05 considered statistically significant. Comparisons of the SNR and CNR of T1WI using temporomandibular surface coil with different matrix were performed using analysis of variance.
For the human hearts, the sensitivity, specificity and accuracy of MRI for classifying the plaques were calculated. To test for intra-observer and inter-observer agreements of MRI-based plaque classification, the kappa statistics (k) were used.
Go to :
RESULTS
Porcine Coronary Artery
The SNR, CNR1 and CNR2 of T1WI using temporomandibular surface coil, eight-channel head surface coil and knee coil were summarized in Table 1. The SNR, CNR1 and CNR2 of T1WI using temporomandibular surface coil were higher than those using eight-channel head surface coil and knee coil (p < 0.05) (Fig. 2). The SNR and CNR2 of T1WI using knee coil were higher than those using eight-channel head surface coil (p < 0.05). However, the CNR1 of T1WI using knee coil was higher than that using eight-channel head surface coil and did not reach statistical significance (p > 0.05). The SNR and CNR1 and CNR2 of T1WI with 512 × 512 in matrix using temporomandibular surface coil were lower than those with 384 × 256 in matrix (p < 0.05) (Fig. 3), but markedly higher than those using eight-channel head coil and knee coil with 384 × 256 in matrix (p < 0.05). Accordingly, the image quality of T1WI, PDW and T2WI with 512 × 512 in matrix using temporomandibular surface coil was still satisfactory due to the coronary artery wall visualized clearly, accompanying higher spatial resolution compared with 384 × 256 in matrix (Fig. 4).
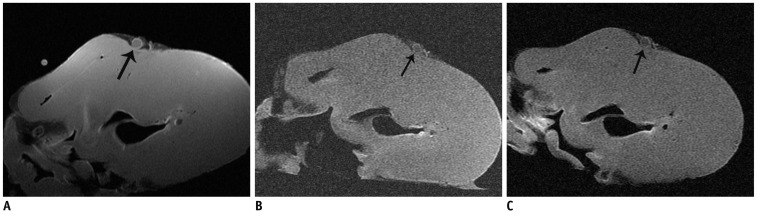 | Fig. 2Signal noise ratio, and CNR between left anterior descending artery wall and lumen, of T1 weighted image, using temporomandibular surface coil (A) were higher than those of head coil (B) and knee coil (C) with same parameters, 384 × 256 in matrix.
|
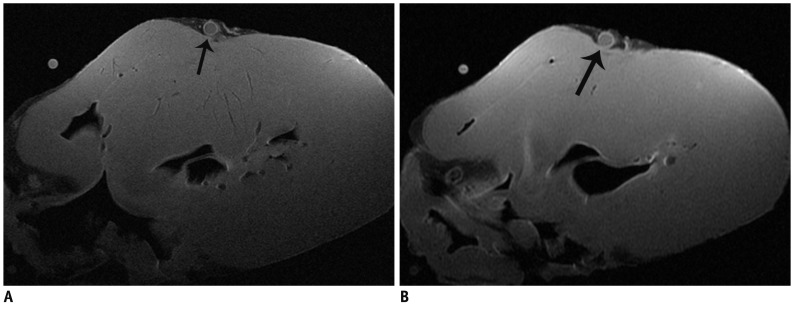 | Fig. 3Signal noise ratio, and CNR between left anterior descending artery wall and lumen, of T1 weighted image, with 512 × 512 in matrix (A) using temporomandibular surface coil were lower than those with 384 × 256 in matrix (B), however coronary artery wall was demonstrated more clearly.
|
 | Fig. 4
Image quality of T1 weighted image (A), proton density-weighted image (B) and T2-weighted image (C) with 512 × 512 in matrix was still satisfactory using temporomandibular surface coil, accompanying higher spatial resolution compared with 384 × 256 in matrix. Coronary artery wall was visualized clearly (black arrow) and noise was acceptable.
|
Human Coronary Artery
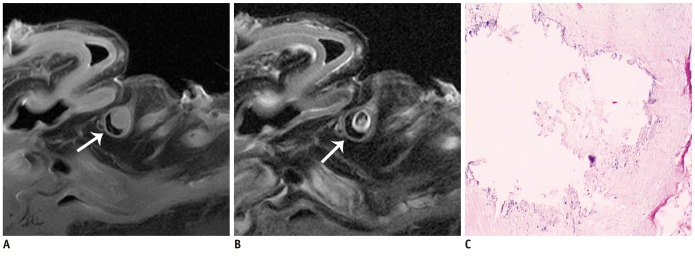
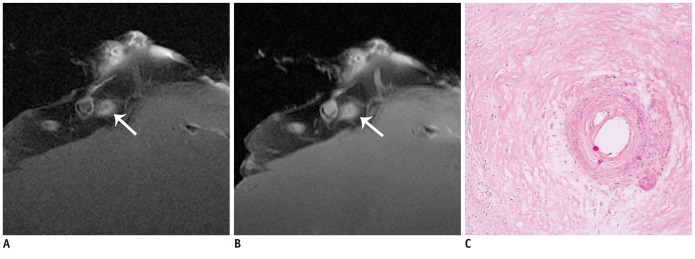
A total of 58 MRI images from the 8 hearts were matched with corresponding histopathologic sections. Among the histopathologic sections, there were 18 lipid-rich plaque sections (type IV-V) (31%) (Fig. 5), 4 hemorrhage plaque sections (type VI) (7%) (Fig. 6), 33 calcified plaque sections (type VII) (57%) (Fig. 7), and 3 fibrous plaque sections (type VIII) (5%) (Fig. 8).
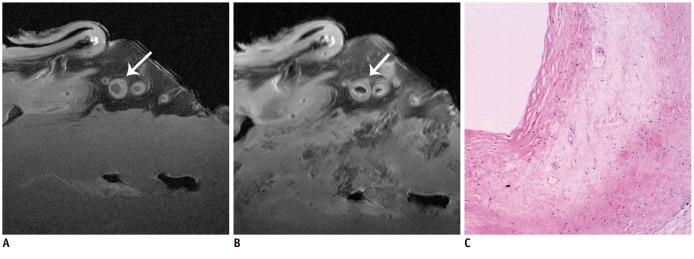 | Fig. 5Type IV-V lesion.
MRI images (A, B) showed irregular thickening of left anterior descending artery wall, slightly high or equal signal on T1 weighted image (A), and slightly low signal on proton density-weighted (B) (white arrow in A and B). Pathological section showed extracellular lipid accumulating into lipid pool (C). Original magnification was × 4.
|
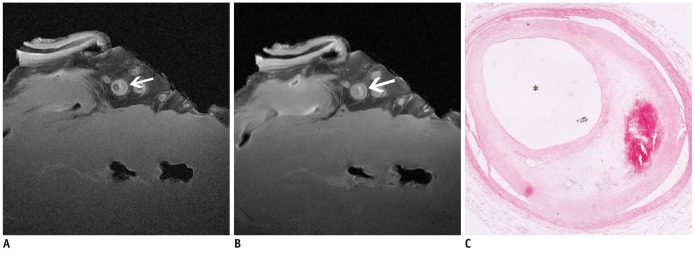 | Fig. 6Type VI lesion with intraplaque hemorrhage.
Plaque showed high signal on T1 weighted image (A) and proton density-weighted (B) (white arrow in A and B). Pathological section showed intraplaque hemorrhage (C). Original magnification was × 4.
|
The accuracy of MRI for classification of plaques was 93% (54/58), and the distribution of plaques was shown in Table 2. The sensitivity and specificity of MRI for identifying different types of plaques were: type IV-V, 94% and 95%; type VI, 100% and 98%; type VII, 91% and 100%; and type VIII, 100% and 98%, respectively. Intra-observer agreement among two readers for two readings with 2 months apart was excellent (k = 0.85 and k = 0.83). Agreement between two readers was also very good for plaque classification (k = 0.8).

Go to :
DISCUSSION
The major findings of the study were 2-folded: firstly, we found that visualizing the coronary artery wall in vitro using temporomandibular surface coil was of the highest SNR and CNR; secondly, we demonstrated that high-resolution MRI closely agrees with histopathology in the detection of human coronary atherosclerotic plaques compositions and classification of plaques.
The 2.5-inch temporomandibular surface coil is dramatically superior to eight-channel head surface coil and knee coil in ex vivo coronary artery wall imaging. However, knee coil was commonly used in ex vivo coronary artery imaging with magnetic resonance techniques in previous literatures (6, 21). The SNR and CNR of small objects such as coronary arterial wall are improved as the diameter of surface coil decreases. The 2.5-inch temporomandibular surface coil is dramatically smaller than eight-channel head surface coil and knee coil, and matches very well with the coronary artery. Therefore, we used the temporomandibular surface coil and the SNR and CNR of coronary artery wall imaging were markedly higher than those using eight-channel head surface coil and knee coil. To our knowledge, this is the first report to image coronary artery wall ex vivo using temporomandibular surface coil.
Ex vivo high-resolution MRI was able to distinguish human coronary atherosclerotic plaque composition and accurately classify advanced plaques. Based on composition, the AHA classifies coronary atherosclerotic plaques into 8 different types (19, 20). Type I-III plaques belong to early lesions, which can be dissipated; and type IV-VIII plaques belong to advanced lesions. Type IV-V (lipid, necrosis, fibrosis) lesions showed high or equal signal intensity on T1WI and PDW, low or equal signal intensity on T2WI. Type VI (sub-acute hemorrhage) lesions showed high signal intensity on T1WI and T2WI. Type VII (calcification) lesions showed signal loss on all three sequences. Type VIII (fibrosis without lipid core) lesions had equal signal intensity on T1WI and high or equal signal intensity on T2WI. In this study, the sensitivity and specificity of MRI for classifying advanced plaques were high (type IV-V, 94% and 95%; type VI, 100% and 98%; type VII, 91% and 100%; and type VIII, 100% and 98%, respectively).
There are a few limitations in this study. Firstly, ex vivo high-resolution MR imaging techniques can be further optimized. One method is using the high-field MRI scanner, in which SNR and spatial resolution can be further improved (22, 23). Secondly, the number of fibrous plaques was limited because type VIII lesions are rare and may have a potential influence on the assessment of type VIII lesions. Thirdly, the whole coronary arteries including RCA and LCX can't be covered because the temporomandibular surface coil is smaller than the knee joint and head coils.
Conclusions
Temporomandibular surface coil was dramatically superior to eight-channel head coil and knee coil for ex vivo coronary artery wall imaging, providing for higher spatial resolution and improved SNR with 512 × 512 in matrix. Ex vivo high-resolution MRI was able to distinguish human coronary atherosclerotic plaque compositions and accurately classify advanced plaques, which may be helpful for directing the development and optimizing the vivo MR vessel wall imaging techniques for characterizing coronary atherosclerotic plaques.
Go to :
 XML Download
XML Download