

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric varices are a complication of portal hypertension (1-3), although less common than esophageal varices (1). However, once gastric varices bleed, the mortality rate without therapy is high: 45-55% (1, 4, 5). Thus, quick management of bleeding gastric varices is necessary. Balloon-occluded retrograde transvenous obliteration (B-RTO) is known as an effective therapy for gastric varices (6-9).
Ethanolamine oleate, which is used as a sclerotic agent, can cause hemolysis, releasing free hemoglobin and possibly causing renal tubular disturbance and acute real failure. Since excessive amounts of ethanolamine oleate will cause acute renal failure, the total amount used in the B-RTO procedure should be reduced as much as possible. In general, the maximum volume of ethanolamine oleatehtiopamidol (EOI) is approximately 20 mL in most sessions of endoscopic injection sclerotherapy for esophageal varices (5). EOI is also used in B-RTO as a sclerotic agent. According to Kiyosue et al. (10), sufficient filling of the entire gastric varix by sclerotic agents is necessary in B-RTO. In most cases, more than 20 mL of EOI is required to obtain complete variceal thrombosis (7-9).
In our institution, in principle, the B-RTO catheter is retained overnight. In cases where a large amount of sclerotic agent would be necessary, we have made it a rule only to infuse sclerotic agents to the maximum extent with regard to safety the first day. Then, if distribution in the gastric varix is very scanty or none although the sclerotic agent can be seen in the gastro-renal shunt, the following day we again infuse the sclerotic agent to obtain sufficient distribution in the entire gastric varix.
In the present study, we retrospectively analyzed the safety and usefulness of such a two-tiered approach in B-RTO as treatment for large gastric varices after portal hypertension.
Go to : 
MATERIALS AND METHODS
Patients
Between October 2004 and October 2011, 50 patients underwent B-RTO for gastric varices that occurred as a consequence of portal hypertension (23 women, 27 men; age range, 40-81 years; mean age, 66.1 years) performed by one of four interventional radiologists experienced in this procedure within our institution. In all patients, endoscopy revealed active bleeding (spurting or oozing) (n = 6) or signs of recent bleeding and/or growing gastric varices during the observation period (n = 44). Before B-RTO, a contrast-enhanced abdominal CT was performed to evaluate the gastric varices and presence of drainage veins such as a gastro-renal shunt. Criteria for admission into the study included a dilated drainage vein such as a gastro-renal shunt, no obstruction of the portal vein, and Child-Pugh Classification A or B. Patients provided written informed consent to undergo the procedure. Our institution does not require approval from the institutional review board for this type of retrospective study.
Procedures
In patients with a dilated gastro-renal shunt as seen on contrast-enhanced abdominal CT (n = 45), we performed B-RTO according to the method described by Kanagawa et al. (6). Briefly, after an 8-Fr catheter sheath-introducer (Medikit, Tokyo, Japan) was inserted from the right femoral vein under local anesthesia, a 6-Fr balloon catheter with a balloon 20 mm in diameter (Clinical Supply, Gifu, Japan) was advanced to the left renal vein through the sheath-introducer, and the tip was wedged into the end of the gastro-renal shunt. The balloon was inflated to occlude the gastro-renal shunt.
Retrograde venography was performed to identify gastric varices and their inflowing and outflowing vessels and to evaluate the degree of outflowing vessels other than the gastro-renal shunt. When this retrograde venography revealed that large collateral vessels had developed as additional drainage veins for the gastric varices, these collateral vessels were embolized with micro-coils. For this embolization, a micro-catheter was coaxially advanced from the balloon catheter inserted into the gastro-renal shunt or from a 5-Fr catheter newly inserted from the femoral vein and advanced to the segment of the collateral vein that entered into the inferior vena cava.
Then 5% EOI (mixture of 10% ethanolamine oleate [Oldamin, Takeda Pharmaceutical, Osaka, Japan] and the same volume of 370 mgI/mL iopamidol) were slowly administered until the entire gastric varix was shown by fluoroscopy to be filled. When collaterals too small to advance the micro-catheter developed, in the early steps of embolization 5% EOI was administered intermittently over a period of approximately 30 minutes in expectation of embolization regarding those vessels (11). However, when the volume of 5% EOI exceeded 20-30 mL, further infusion of 5% EOI was abandoned even if sufficient distribution of the sclerotic agent in the gastric varix was not obtained. The patient shown in Figure 1 is one of such cases.
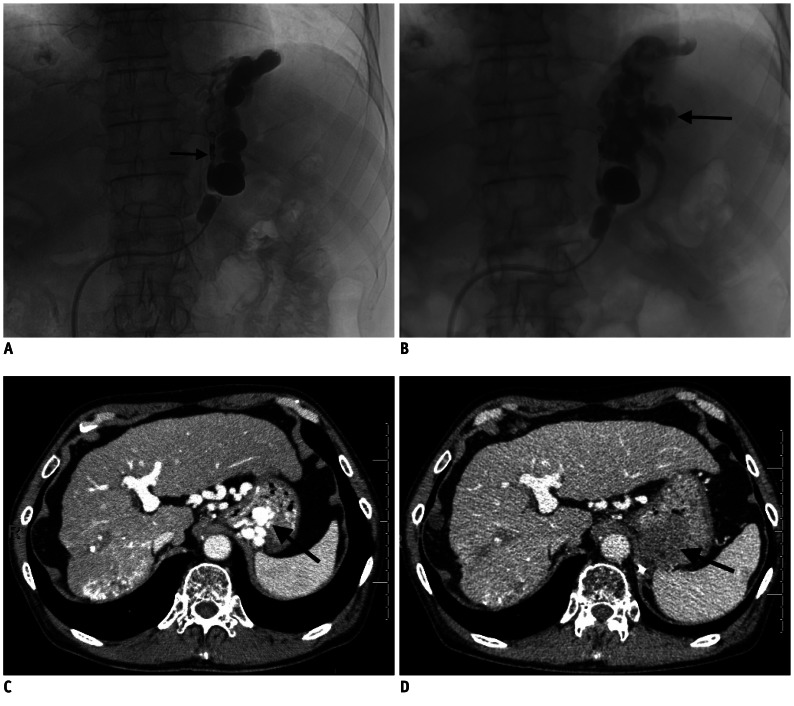 | Fig. 168-year-old man with gastric varix (patient no. 8 in table).
A. Fluoroscopic image obtained after infusion of sclerotic agent from balloon catheter positioned at gastro-renal shunt shows no distribution of sclerotic agent in gastric varix. Note that left inferior phrenic vein that developed as collateral vein had been embolized with micro-coils (arrow). B. Retrograde venography obtained with balloon occlusion of gastro-renal on day 2 shows that contrast material is distributed in entire gastric varix (arrow) through gastro-renal shunt that had been thrombosed in some but not all areas. C. Enhanced CT before balloon-occluded transvenous obliteration shows that intravenously administered contrast agent allows visualization of varix in gastric walls (arrow). D. Enhanced CT obtained 6 days after balloon-occluded transvenous obliteration shows well-thrombosed gastric varix (arrow).
|
For the 33 patients who had large gastric varices we added an injection of 2-53 mL (mean, 19.6 mL) of 50% glucose solution before the injection of the 5% EOI to reduce the dose of the 5% EOI as recommended by Hirota et al. (8) and Yamagami et al. (9). Details of usage for the 50% glucose solution were described elsewhere (9). During these procedures, 4000 units of human haptoglobin was administered intravenously to prevent renal failure owing to hemolysis. Details of the B-RTO procedure have been described elsewhere (5-11).
To avoid incomplete therapeutic efficacy and pulmonary embolism due to an unstable thrombus, we left the catheter in the gastro-renal shunt with the balloon inflated for 15-20 hours (i.e., until the next morning), at which time retrograde venography was performed. When sufficient occupation of the thrombus in the gastric varix was confirmed, the catheter was removed. However, if flow into the gastric varix was still evident, 5% EOI was additionally infused to obtain distribution in the entire gastric varix as shown by fluoroscopy. When it was considered that a large amount of sclerotic agents would be necessary, 50% glucose solution was additionally used. Prior to this additional infusion, we confirmed that renal dysfunction due to the first day's treatment had not occurred. After 30 minutes, the catheter was withdrawn.
In the 5 patients who did not have a gastro-renal shunt, B-RTO was performed from another dilated drainage vein: from the left inferior phrenic vein in 4 and from the pericardiacophrenic vein in 1. With the use of the left inferior phrenic vein, a 5-Fr balloon catheter with a balloon 11 mm in diameter (Moiyan, Miyano, Kobe, Japan) was inserted from the right femoral vein and was advanced through the inferior vena cava to the left inferior phrenic vein. Embolization of the collateral vessels and infusion of sclerotic agents to the gastric varix were done through a microcatheter coaxially advanced from the balloon catheter. When B-RTO was performed from the pericardiacophrenic vein, a 3.3-Fr balloon catheter with a balloon 8 mm in diameter (Fuji Systems, Tokyo, Japan) was advanced coaxially through a 6-Fr guiding catheter that had been inserted from the left subclavian vein punctured under guidance of ultrasonography and advanced to the pericardiacophrenic vein. Then, this 3.3-Fr balloon catheter was used for embolization of the collateral vessels and infusion of sclerotic agents into the gastric varices.
Contrast-enhanced abdominal CT images were obtained approximately one week after B-RTO to evaluate the therapeutic effects in all patients. Gastrointestinal endoscopy was routinely performed one month after B-RTO and every 3 to 6 months thereafter. Endoscopic findings for varices were evaluated by endoscopists.
Parameters Investigated
First, distribution of the sclerotic agent in the gastric varices on the first day was evaluated in all cases. Then the following parameters were retrospectively investigated for cases with poor distribution on the first treatment day: 1) management of such cases on the second day, 2) changes in blood data for hepatic, renal, and coagulation systems, 3) recurrence of gastric varices, and 4) complications related to the B-RTO procedure.
Images such as balloon-occluded retrograde venography obtained during the B-RTO procedure and contrast-enhanced CT images acquired before and approximately one week after B-RTO were analyzed by two of the authors. A consensus on the interpretation was reached through discussion.
Go to :
RESULTS
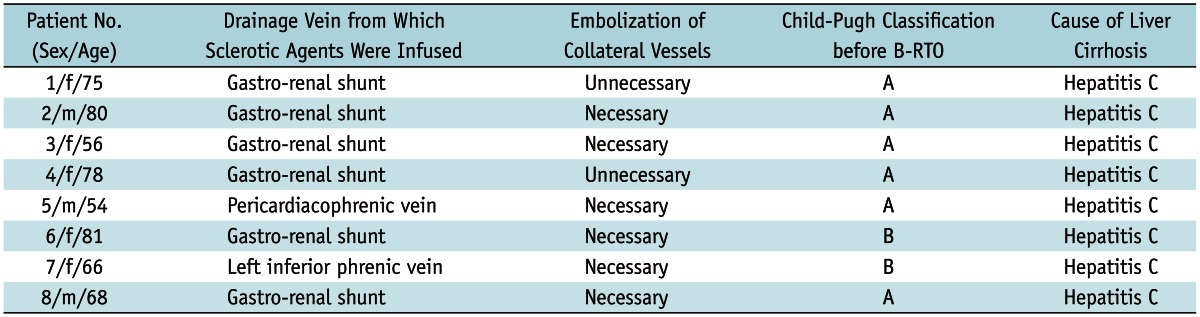
In all 50 patients, the balloon catheter from which sclerotic agents would be infused was successfully advanced to the intended drainage vein of the gastric varix. On day 1 of therapy, sufficient distribution of the sclerotic agent in the entire or almost the entire gastric varix was shown in 42 patients (84%). However, in 8 patients (16%), there was very little (n = 6) or no (n = 2) distribution in the gastric varix although the sclerotic agent was seen in its drainage vein. Tables 1 and 2 provide information on the characteristics of the 8 patients and the B-RTO procedures in these patients, respectively.
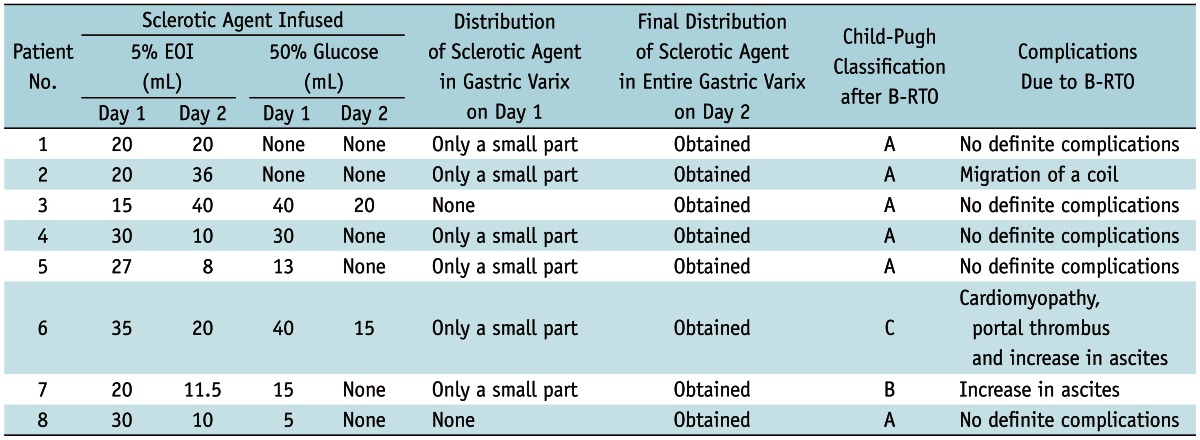
In those 8 patients, balloon-occluded retrograde venography obtained on day 2 showed that the entire gastric varix could be visualized although some areas of the gastro-renal shunt were thrombosed. In those cases, additional infusion of the sclerotic agent was performed, and the sclerotic agents were distributed in the entire gastric varix in all 8 patients. The mean volume of EOI infused on day 1 was 24.6 mL (range 15 to 35 mL) while the mean volume on day 2 was 19.4 mL (range 8 to 40 mL). Contrast-enhanced abdominal CT after B-RTO revealed that gastric varices were well obliterated in all 8 patients. During the follow-up period (mean, 51.2 months; range, 19-90 months), endoscopy revealed no recurrence of gastric varices and the new development of esophageal varices in 1.
As for complications related to the B-RTO procedure in these 8 patients, stress cardiomyopathy occurred in 1, development of thrombus in the portal vein in 1, and a temporary increase in ascites in 2 patients. In one patient, a micro-coil migrated from the left inferior phrenic vein to the right atrium during the procedure, but no arrhythmia or other serious complications occurred. No decrease in renal function was observed. Pulmonary edema did not occur in any patient nor was there worsening of the coagulation system. Symptoms suggesting pulmonary embolism were not observed in any of these patients. The Child-Pugh classification worsened in only one patient.
Go to :
DISCUSSION
Treatments for portal hypertension can be roughly classified into two types: shunt occlusion and shunt creation (3). A transjugular intrahepatic portosystemic venous shunt procedure is included among the latter therapies (12-14). On the contrary, B-RTO is a shunt occlusion therapy and is performed to prevent the rupture of gastric varices due to portal hypertension (6-11, 15-17).
In 1984, Olson et al. (18) first reported a case of a gastric varix treated with B-RTO using ethanol as the sclerotic agent; however, the treatment did not result in the disappearance of the gastric varix. But since the preliminary report by Kanagawa et al. (6) on the use of EOI as the sclerotic agent, reports of the effectiveness of B-RTO for gastric varices have increased (7-10). Its effectiveness has been reported to be good; Kitamoto et al. (19) demonstrated complete success in 88% of 23 patients, with a 9% rate of re-bleeding from gastric varices. Ninoi et al. (20) reported a 5-year recurrence rate of 2.7% and a 5-year bleeding rate of 1.5%. Considering these low rates, they suggested that B-RTO could become a standard treatment for gastric varices with a gastro-renal shunt.
Ethanolamine oleate-iopamidol is used as a sclerotic agent at the time of B-RTO as well as for endoscopic injection sclerotherapy (6-9). Ethanolamine oleate agglutinates platelets and destroys the endothelial cells of the vessels, then works as a sclerotic agent. However, this agent can occasionally be diverted to the destruction of red blood cell membranes (8). Thus, although few, there have been reports of complications caused by this sclerotic agent such as pulmonary edema (21), disseminated intravascular coagulation (22), hemothorax (23), cardiogenic shock (8), and renal tubular disturbance and renal insufficiency (7), all of which are attributable to hemolysis of red blood cells caused by ethanolamine oleate.
The maximum volume of EOI used is approximately 20 mL in most sessions of endoscopic injection sclerotherapy for esophageal varices. In reports of B-RTO, the recommended volume of EOI has been within approximately 20-30 mL (8, 9). In general, however, B-RTO requires more than 30 mL of ethanolamine oleate (6-9), a difference that is due to the greater size of gastric varices in comparison with esophageal varices. Hence, the risk of the complications mentioned above may increase in B-RTO, paralleling the increased volume of the sclerotic agent. The advancement of micro-catheters close to gastric varices has been reported to be advantageous in reducing the amount of sclerotic agent required (24).
In the original report of B-RTO by Kanagawa et al. (6), the B-RTO catheter was withdrawn 30 minutes after the procedure. However, in more recent reports, the B-RTO catheter was retained overnight to avoid incomplete therapeutic efficacy and pulmonary embolism due to an unstable thrombus (15, 20, 24-27). The appropriate amount of sclerotic agent that should be infused on day 1 and day 2 has not been determined. Additionally, to our knowledge, there has been no report of the management of large gastric varices in which distribution of sclerotic agents in the gastric varices achieved on the first day was none or very scanty.
Among our study patients, when it was considered that large amounts of sclerotic agent would be necessary, these agents were infused only to the acceptable extent on the first day and, if necessary, an additional infusion would be administered the following day to achieve sufficient distribution in the entire gastric varix. This was necessary in 8 patients, and after treatment on day 2 the entire gastric varix in each patient was well visualized on balloon-occluded retrograde venography and completely obliterated. Mean volume of EOI infused was 24.6 mL on day 1 and was 19.4 mL on day 2, both of which were acceptable volumes. Gastric varices have not recurred in any of these patients. Complications caused by EOI itself, such as pulmonary edema and renal insufficiency did not occur despite the large volume of EOI infused over the two days.
The present study had some limitations. It was not a randomized prospective case control study, and even though the study population was comprised of 50 patients, the main focus of this report involved only 8 patients. Doses of 5% EOI were divided over two days, with the total dose varying from 31.5 mL to 56 mL and the volume of 5% EOI administered on the first day varying from 15 mL to 35 mL. There is no protocol for the upper limit of 5% EOI volume on the first day, which could be considered as a limitation of interpretation in regard to the results. There is also no protocol for the appropriate volume of 50% glucose solution to be used on the first and second day. There is a possibility that the addition of 50% glucose infusions might have had the effect of reducing the total volume of 5% EOI required in these patients. Thus, our results might have involved the mixed effect of both 50% glucose infusions and 5% EOI. However, in the current study we did not investigate the effect of 50% glucose infusions. Since this is a clinical and observational study, volumes of 5% EOI and glucose solution were decided based largely on the experience of the operator. Thus, a further study with a larger number of subjects would be required to determine the most appropriate volumes.
From the results of this study, it could be concluded that when a gastric varix is too large to be obliterated by B-RTO with an acceptable volume of EOI, it might be effective and feasible to only induce thrombosis of the drainage vein of the gastric varix on day 1 with an acceptable volume of EOI. Then, on the following day sclerotic agents can be infused sufficiently to be distributed in the entire gastric varix through the balloon catheter positioned overnight.
Go to :
 XML Download
XML Download