

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Magnetic resonance imaging (MRI) has been widely used for the diagnosis and evaluation of malignancies arising in various parts of the body, but its use in evaluating superficial structures has been limited, due to the high resolution required. However, the introduction of microscopy surface coils has enabled its use in the evaluation of more superficial structures with better image quality and high resolution (1). Numerous studies have shown the usefulness of high-resolution MRI with microscopy coils (HR-MRI) in the evaluation of patellar cartilage, soft tissue tumors of the hand and foot, and ocular lesions including ocular melanomas (2-4). To meet the growing interest in the noninvasive imaging and characterization of benign and malignant dermatologic disorders, there have been efforts to further increase the signal-to-noise ratio (SNR) of MR images. With a small-diameter surface-coil, MRI has demonstrated the ability to achieve sufficient SNR for high-resolution imaging of healthy skin, as well as of benign and malignant skin lesions with microscopic resolution at 1.5T (5).
As the incidence of malignant melanoma of the skin is increasing worldwide, studies have been conducted concerning new techniques for the diagnosis and evaluation of melanomas. The application of MRI in the differentiation of melanoma and benign melanocytic lesions has been attempted in previous studies (6, 7). Mäurer et al. (6) studied the usefulness of SNR and contrast-noise ratio analysis in high resolution MRI in differentiating malignant skin tumors from benign skin tumors of the melanincontaining system. MRI had a limited role in differentiation thus clinical and histologic examinations were proposed to be the next important step in the evaluation of melanin containing skin tumors. Another study by Pennasilico et al. (7) showed that dynamic subtraction magnetic resonance (MR) imaging may be helpful in differentiating in vivo melanomas from benign melanocytic lesions. However, to our knowledge, no attempt has been made to utilize HR-MRI as a tool for the preoperative evaluation of malignant melanomas. The accurate determination of the microscopic stage of melanoma by measuring the vertical thickness of the lesion in millimeters is important in determining the radial margin of the surgical excision and predicting the prognosis of the disease. Currently, this is only feasible during the histopathologic examination, after the primary tumor has been excised. In this study, we aimed to evaluate the accuracy of the preoperative MRI using a microscopy coil in assessing the thickness of the primary tumor in malignant melanomas.
MATERIALS AND METHODS
Our institutional review board approved this retrospective study and informed consent was waived.
Patient Selection
Fifteen patients with malignant melanoma who had undergone preoperative MR imaging in our institution, between January 2004 and January 2011 were identified from our radiology report database. Inclusion criteria were as follows: 1) a histopathologic diagnosis of malignant melanoma of the skin, and 2) MR imaging performed with a microscopy coil. We excluded four patients due to the following conditions: 1) MR imaging performed without a microscopy coil (n = 2), 2) prior treatment (n = 1), and 3) insufficient histopathologic data (n = 1). As a result, a total of eleven patients were included in the study (6 men, 5 women; mean age, 69 years; age range, 51-82 years).
Image Acquisition
All MR images were obtained with a 1.5T MR imager (Gyroscan NT Intera, Philips Healthcare Best, The Netherlands), using a microscopy coil consisted of a single turn with an inner-diameter of 47 mm. The coil was fixed to the region of interest by tape. The MR imaging protocol included axial T2-weighted fast spin echo (FSE) (repetition time [TR] msec/echo time [TE] msec, 2447/100; section thickness, 1.5 or 3.0 mm; field of view [FOV], 90 × 90 mm; matrix, 256 × 256; echo train length [ETL], 12) or sagittal T2-weighted FSE (2500/80 [TR msec/TE msec]; section thickness, 1.5 or 3.0 mm; FOV, 60 × 60 mm; matrix, 256 × 256; ETL, 8). T1-weighted FSE sequences with fat suppression (FS) were also acquired in the axial or sagittal plane after the intravenous administration of 0.1 mmol/kg of gadodiamide (Omniscan, GE Healthcare, Princeton, NJ, USA) with the following imaging parameters: 400/22 (TR msec/TE msec), section thickness, 1.5 mm; FOV, either 60 × 60 mm or 90 × 90 mm; matrix, 256 × 256; ETL, 4.
Image Analysis
In consensus, two radiologists (a musculoskeletal staff radiologist with 10 years of experience in musculoskeletal imaging and, a third year resident) selected the imaging plane, which best depicted the thickness of the primary tumor prior to image analysis. Both radiologists agreed on the fact that despite the presence of edema, the subjective tumor conspicuity was greater on T2-weighted images (T2WI) and Gd T1-weighted fat suppressed images (Gd-FS-T1WI) compared to T1-WI, and therefore were selected as the target of analysis. Image analysis was performed in two separate sessions, two weeks apart; the observers independently evaluated the T2WI and Gd-FS-T1WI in two separate sessions. On the selected image plane, the maximum vertical tumor thickness was measured by drawing a line perpendicular to a horizontal line connecting the two tumor-skin interfaces (Fig. 1). Measurements of the thickness of the primary tumor were measured in millimeters and were taken down to the 2nd decimal place and the decimal number was rounded to the closest tenth place for each image sequence in regards to each session.
Histopathologic Analysis
In all patients, the biopsy and surgical specimens were also retrospectively reviewed by a pathologist (with 15 years of experience in bone and soft tissue pathology) at our institution. The specimens were evaluated histopathologically for features of malignant melanoma, with a special focus on the primary tumor thickness. The primary tumor thickness was measured from the top of the epidermal granular layer to the deepest melanocyte of the invasive component of melanoma (8, 9). When correlating the MR findings with the histopathologic results, the tumor thickness in punch biopsy and subsequent surgical specimens were both considered and the greater value of the two values were selected for statistical analysis.
Statistical Analysis
All statistical analyses were performed with MedCalc software (version 11.1.1.0 for Microsoft Windows 2000/XP/Vista/7; MedCalc Software, Mariakerke, Belgium). A p value of less than 0.05 was considered statistically significant.
Intra- and interobserver variabilities of the measurements of primary tumor thickness were evaluated by using the intraclass correlation coefficient (ICC). An ICC value greater than 0.75, was considered to represent good agreement (10, 11). In order to quantify the relationship between histopathologic thickness and each of the measurements, concordance correlation coefficients (CCCs) were assessed along with their 95% confidence intervals (12, 13). The CCC measures the reproducibility of two measurements by evaluating the degree to which pairs of observations fall on the 45° line. We referred to recommendations suggested for a similar metric, the κ statistic (14), to guide interpretation of the CCC (12). CCCs of 0.81-1.00 indicated almost perfect agreement; 0.61-0.80, substantial agreement; 0.41-0.60, moderate agreement, 0.21-0.40, fair agreement; and 0-0.20, slight to poor agreement (12).
RESULTS
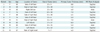
All 11 patients presented with a pigmented skin lesion of growing size. The mean size of the lesions was 20.1 mm (range, 7.0-60.0 mm). The tumors were localized on the plantar aspect of the foot (n = 7) (Fig. 3), toe (n = 1) (Fig. 4), thumb (n = 2), and on the palm of the hand (n = 1). Punch biopsy was performed for the 11 lesions and all were histopathologically confirmed for malignant melanoma, prior to MR imaging. Surgical excision was performed in 10 cases, whereas in one case, surgical treatment was not performed due to the patient's co-morbidities. The median time from biopsy to MR examination was 11 days (range, 0-35 days), and the median time from MR examination to surgery was 8 days (range, 1-18 days). The demographic data and histopathologic findings are summarized in Table 1.
Primary Tumor Thickness on MR: Correlation with Histopathologic Results
The intraobserver variabilities of readers 1 and 2 are shown in Table 2, and the interobserver variability in Table 3. All ICC values exceeded 0.75, indicating good agreement. A tendency of higher agreement was observed on T2WI, compared with Gd-FS-T1WI. Scatter plots of tumor thickness measurements on Gd-FS-T1WI and T2WI versus histopathologic results are shown in Figure 2. Most tumor thickness measurements taken on Gd-FS-T1WI overestimated the histopathologic tumor thickness (81.8% [9/11] overestimated and 18.2% [2/11] underestimated by reader 1 and 100% [11/11] overestimated by reader 2). For T2WI, the overestimated measurements were 81.8% (9/11) for both readers 1 and 2. The data points were closer to the 45-degree line for T2-WI, compared to Gd-FS-T1WI.
The CCC and corresponding 95% interval for each tumor thickness measurements compared with the histopathologic findings are shown in Table 4. The CCC of measurements on T2WIs ranged from 0.64 to 0.78, indicating a substantial agreement, whereas the CCC of measurements on Gd-FS-T1WIs ranged from 0.50 to 0.61, indicating moderate to substantial agreement.
DISCUSSION
A melanoma is a malignant tumor of melanocytes, which are derived from the neural crest. Most melanomas arise in the skin, although they may also arise at other sites where neural crest cells migrate, such as mucosal surfaces or the eye. Melanomas can develop on any site on the skin surface, but there seems to be a predilection of sites according to gender, with a greater number of occurrences appearing on the extremities in women, and on the trunk or head and neck in men. All 11 patients included in our study presented with melanoma located in the extremities, with the majority located on the plantar aspect of the foot.
The prognosis of melanoma is affected by clinical and histological factors and by the anatomic location of the lesion. Thickness of the primary tumor, mitotic index, number of regional lymph nodes involved, and ulceration or bleeding at the primary site are histologic factors known to affect the prognosis (15). For diseases clinically confined to the primary site, the greater the thickness of the primary tumor, the higher the chance of lymph node or systemic metastases and the worse the prognosis. Thus, determining the microscopic stage of melanoma by measuring the vertical thickness of the lesion in millimeters is important.
However, accurate microscopic staging of the primary tumor requires careful histologic evaluation of the whole specimen, and therefore is currently only possible after complete excision of the primary melanoma. Surgical excision is performed with margins proportional to the microscopic stage of the primary lesion; for lesions 2 mm or less in thickness, this signifies a 1 cm radial margin, whereas for melanomas greater than 2 mm to 4 mm in thickness, this means a radial excision margin of 2 cm to 3 cm and so on (16, 17). In cases where the final surgical specimen reveals a more vertically extensive lesion than preoperatively evaluated, additional surgical procedures may be needed. One patient included in our study had undergone excisional biopsy at an outside hospital. A histopathologic review of the specimen at our hospital revealed an insufficient radial margin with regard to the thickness of the tumor, and therefore, the patient underwent additional excision. Pre-surgical determination of the precise vertical and horizontal extent of the tumor can help in surgical planning, and this may be achieved with MR imaging.
With the introduction of microscopy coils in MR imaging, the SNR can be increased by minimizing the noise in small-sized voxels. Many studies have shown that MRI with microscopy coils can serve as a diagnostic tool for various skin lesions. Krug et al. (18) demonstrated that high resolution MR images obtained by a 1.0T system using a microscopy coil with an inner diameter of 75 mm enabled visualization of the dermis, subcutaneous tissue, and muscle fascia allowing for a pattern analysis that may minimize the differential diagnosis of various skin diseases and may help to reduce the number of skin biopsies in certain indications. In a study by Gufler et al. (19), high-resolution MRI with a microscopy surface coil and a high-field 1.5-T MR system proved to be a suitable method to determine the extension and depth of infiltration in regards to basal cell carcinomas of the facial region.
Our study results demonstrated that the primary tumor thickness measurements on both T2WI and Gd-FS-T1WI showed excellent intra- and interobserver agreements, suggesting that measurement of tumor thickness on MRI may be a reliable method. Additionally, the correlation between the measurements taken on MRI and histopathologic tumor thickness was also evaluated in our study. The measurements taken on T2WI showed a substantial correlation with the histopathologic tumor thickness, compared with a moderate correlation on Gd-FS-T1WI. The measurements on Gd-FS-T1WI had a greater tendency to overestimate the tumor thickness. We speculate that nonspecific skin enhancement at the biopsy site may have interfered with the measurement of primary tumor thickness on Gd-FS-T1WI. Post-biopsy MRIs performed on patients with breast cancer have been reported to show focal skin enhancement and edema at the skin entry site for a short time after percutaneous biopsy (20).
The results of our study suggest the potential advantage of MRI with microscopy coils as a preoperative evaluation tool in malignant melanomas of the skin. The whole lesion can be evaluated prior to any surgical procedure, and microscopic staging of the tumor may be possible, especially on T2WI. However, the accuracy of evaluation regarding primary tumor thickness on MRI is not yet sufficient, and further improvement of imaging is essential for MRI to play a pivotal role in the preoperative evaluation of malignant melanomas of the skin. The use of a smaller microscopy surface coil and imaging at a higher magnetic field strength are factors that may increase the SNR in small sized voxels. Additionally, the use of anisotropic voxels with the smallest dimension being perpendicular to the skin surface may aid in the delineation of different skin layers.
There are several limitations to our study. First, the number of patients included in the study was relatively small, and the types of melanoma were limited. Second, because of the retrospective nature of the study, the imaging parameters varied. Some of the images were acquired with a section thickness of 3 mm, which implies the potential for a failure to depict the deepest site of tumor invasion. The in-plane resolution was also inconsistent, which may have affected the results of our study. Further studies with more consistent imaging parameters are needed. Third, all patients underwent punch biopsy before having the MRI performed, and in turn the image evaluation of the melanoma was confounded by the post-biopsy changes of the surrounding soft tissue.
We have shown that, high-resolution MR images obtained using a microscopy coil correlated well with histopathologic findings in patients with malignant melanoma of the skin. MR imaging with microscopy coils enables the assessment of the thickness of the primary tumor, especially on T2WI compared to Gd-FS-T1WI, which may allow for a more accurate preoperative evaluation of the disease, thereby potentially improving preoperative planning.







 XML Download
XML Download