

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic liver diseases are a major public health problem as they account for significant morbidity and mortality worldwide (1). Early diagnosis and staging of liver fibrosis is important in order to ensure optimal treatment planning for patients with chronic liver diseases, which can ultimately lead to cirrhosis, decompensated liver disease, and hepatocellular carcinoma (HCC) (2-4). Furthermore, several previous studies have demonstrated that the degree of fibrosis also has prognostic significance in patients with chronic hepatitis B or C (5, 6). Until now, liver biopsy has been widely accepted as the most specific test for assessing the nature and severity of liver diseases, and also as the gold standard method used to assess liver fibrosis (7). However, liver biopsy has several limitations, including possible procedure-related complications, sampling error, and intra- or interobserver variability, leading to potential over- or under-staging of hepatic fibrosis (HF) (8, 9). For these reasons, there has been a huge clinical demand for a noninvasive option, which can be used to diagnose HF and to differentiate the degree of fibrosis (4, 10).
Until now, there have been numerous attempts to evaluate the degree of HF using image-based techniques, such as diffusion-weighted imaging, perfusion CT, contrast-enhanced ultrasound (US) examination, dynamic contrast-enhanced magnetic resonance (MR) imaging, hepatocyte-specific MR contrast-media-enhanced MRI, and various stiffness imaging techniques (elastography) (1, 6, 11-17). Among these methods, stiffness imaging techniques, such as transient elastography (TE), have begun to be used in clinical practice and have received significant attention as potentially successful non-invasive tests for evaluating HF and with meaningful validation for the staging of HF (1, 6, 18, 19). TE appears to be more of an accurate method for the early detection of cirrhosis than other cross-sectional imaging techniques (20). More recently, other stiffness imaging techniques that measure the shear wave velocity in liver tissue, such as magnetic resonance elastography (MRE), and US-based elastography (USE) techniques, such as Acoustic Radiation Force Imaging (ARFI) and Shear wave Elastography (SWE), have been introduced and are now available in the liver (14, 16), as well as in other organs (21-23) at many medical centers. MRE and USE are quantitative measuring tools for HF; however, there have been only a few previous studies comparing the measured liver stiffness (LS) values on TE, ARFI, and MRE in either patients or phantoms (17, 24). Although either examination can be used for the evaluation of HF, there are not a sufficient number of published studies, regarding the correlation between these two examinations in order to be able to correctly determine that the liver stiffness measurements (LSMs) on both examinations are interchangeable. The advantages and disadvantages of MRE and USE, such as their performance on obese patients and those with ascites, have also been discussed in previous studies (25, 26). However, until now, there has been no study that compared the technical success rates and the occurrence of unreliable LSMs obtained by MRE and SWE in the same patients.
Therefore, the goal of this study is to directly compare the stiffness values measured by MRE and USE in the same patients and to show a correlation between the measured LS values obtained using the two techniques. We also attempted to determine the technical success rates and the incidence of unreliable LS measurements of both examinations in liver donors, as well as liver transplantation (LT) recipients with cirrhosis.
MATERIALS AND METHODS
Study Population
This retrospective study was approved by our institutional review board, and informed consent was waived. From August 2011 to June 2012, 114 living liver donor candidates (M : F = 79 : 35, mean age 34.1 ± 11.8 years, age range 16-61) and 94 LT recipient candidates (M : F = 72 : 22, mean age 54.6 ± 8.2 years, age range 28-72) underwent MRE or SWE as part of their preoperative work up. There were 111 study patients who underwent both of MRE and SWE, 42 who underwent only SWE, and 55 who underwent only MRE. In this study population, the technical success rates of both SWE and MRE examinations were determined.
In addition, for cross-validation of the two examinations in the normal liver and cirrhotic liver, we included liver donors with no evidence of HF and recipients with histologically determined liver cirrhosis (F4), and in whom the LS values were successfully measured on both exams. Among the 50 liver donors and 61 recipients who underwent both MRE and SWE examinations, six donor candidates and 20 recipient candidates without histological confirmation were excluded. In addition, seven liver recipients were excluded due to technical failure on MRE or SWE. Additional nine patients were excluded for the following reasons: 1) two donor candidates with HF (F1 [n = 1] and F2 [n = 1]); 2) a recipient with an inappropriate histological diagnosis for HF (fulminant hepatitis [n = 1]); and 3) six recipients who did not have liver cirrhosis (F2 [n = 1], F3 [n = 5]). Finally, the data of 42 living liver donors (M : F = 33 : 9, mean age; 34.3 ± 12.7 age range; 16-61) and 27 patients with F4 (M : F = 19 : 8, mean age; 53.6 ± 7.53, age range; 36-65) were included for cross-validation of MRE and SWE (Fig. 1). The mean interval between MRE and SWE was 1.5 ± 5.3 days and the median interval between two examinations was 0 days since 71% of study population underwent two examinations on the same day (range: 0-32 days).
Shear Wave Elastography
Shear Wave Elastography was performed using a SWE (Aixplorer™, SuperSonic Imagine, Aix-en-Provence, France) and a convex probe by one of the five abdominal radiologists with 5-8 years of clinical experience. The operators were blinded to the results obtained by using the other technique during the measurements. After placing a region of interest (ROI) in the right anterior segment of the liver, and avoiding major vessels, LS values were measured five times using an intercostal approach. The measurement depth was from 25 mm to 45 mm. Patients were instructed to hold their breath for approximately five to seven seconds while the LS values were being measured.
The convex probe generates pushing beams that displace focal spots in the liver tissue at five different depths. The degree of displacement increases along with the amount of time and is also reinforced by the pushing beams focusing on the different liver tissue depths. Tissue displacement is captured by the ultrafast echographic device in the same probe and at a very high frame rate (> 2000 frames/sec), and these sequences are performed repeatedly in three different directions, i.e. central, left, and right edges of the image. After obtaining the data, one-dimensional speckle tracking using successive echographic images, is performed and the shear wave speed is assessed by means of a time-of-flight estimation between two points during the shear wave propagation between the two different depths (27, 28). Finally, the LS value is calculated as kilopascals (kPa) using shear wave velocity in the liver tissue, according to the following equation: E = 3pvs2. The variable p represents a tissue density, and vs is the shear wave velocity. The median value of five measured LS values is obtained and recorded as the LS value on SWE. The standard deviation (SD) of the five measured LS values is also obtained in each patient.
According to previous studies on TE, SWE is considered to have failed when ROI measurements do not provide a properly color-coded elastogram with an artifact > 30% of the ROI and an appropriate stiffness value after five measurements (20, 29). The stiffness measurement of SWE was also considered unreliable when a patient's measured stiffness values were too varied on SWE. This variability was expressed using a coefficient of variation (CV) where CV was calculated as CV = (standard deviation [SD] / mean LS value on MRE or SWE) × 100%. When the CV of the measured stiffness values on SWE was larger than 30%, the LS values were regarded as unreliable results.
MR Elastography
Magnetic resonance examinations, including MRE, were performed on a 1.5-T whole-body MR scanner (SignaHDx; GE Healthcare, Milwaukee, WI, USA) with an eight-channel torso phased-array coil. All images were obtained either in the axial or the coronal plane. The baseline liver imaging protocol included the following sequences: a respiratory-triggered T2-weighted rapid acquisition relaxation-enhanced sequence; a T2-weighted single-shot fast spin-echo sequence; a breath-hold T1-weighted dual echo (in-phase and opposed-phase) spoiled gradient recalled echo (GRE) sequence; and a T2*-weighted GRE sequence. MRE was performed before injecting gadoxetate disodium.
In order to obtain MRE, a 19-cm-diameter, 1.5-cm-thick, cylindrical passive longitudinal driver (MR-Touch; GE Healthcare, Milwaukee, WI, USA) was placed against the right anterior chest wall with the center of the driver at the level of the xiphisternum. To produce propagating shear waves in the liver, continuous longitudinal vibration at 60 Hz was used and was transmitted from the active driver to the passive driver, which was held in place using an abdominal binder and through a flexible vinyl tube (30). To capture the propagation of the shear waves over a full period of motion, a phase contrast, gradient-echo MRE sequence was used to collect axial wave images sensitized along the through-plane direction of motion (31). The measurement parameters of the MRE gradient echo sequence were as follows: repetition time/echo time, 100/26.8 ms; flip angle, 30°; field of view, 32-37 cm; matrix size, 256 × 64; slice thickness, 10 mm; and a 5-mm interslice gap. Two to the four MRE slices were obtained for each patient.
Patients were instructed to hold their breath as each slice was being obtained. MRE acquisitions were performed in 2-4 slice locations in the liver. The MRE acquisition of each slice required two breath-holds and each breath-holding time was 16 seconds. Therefore, as to gain a consistent position of the liver for each phase offset, patients held their breath at the end of expiration. After the data acquisition was completed, the wave images were automatically processed by the host computer of the MRI system in order to generate elastograms depicting the shear stiffness in kPa, using a local frequency estimation inversion algorithm and a Gaussian band pass filter, as described in a previous study (32).
Before measuring the mean shear stiffness, one attending abdominal radiologist with 18 years of clinical experience including MRE images and elastograms, evaluated the MRE images, including the anatomic image set, wave image set, and the elastogram set. This reviewer assessed the quality of the elastograms by referencing anatomic images and wave images in each patient and then classifying them as adequate or inadequate MRE examinations. Inadequate MRE examinations, i.e. technical failure, were defined as: 1) when wave images showed poor wave propagation; 2) anatomic images showed severe respiratory motion along the slice selection axis (z-axis); or 3) there was significant signal loss of the liver parenchyma compared with that of the kidneys and the muscle, which suggested increased iron overload (11).
The mean LS values of the hepatic parenchyma were then calculated by placing multiple ROIs on the MRE. The ROIs was placed by one attending abdominal radiologist with six years of clinical experience, who was blinded to each patient's clinical history, as well as to the other imaging findings. ROIs were drawn three times in the magnitude image obtained during the MRE sequence. These ROIs could then be copied to the corresponding position in the stiffness map, which then gave the stiffness values in kPa. For the ROI measurement, ROIs were placed on the wave images, where the wave propagations were regular and were relatively free of reflections or interference patterns, and were also clearly demonstrated on the confidence map (33). The ROIs were also usually placed in the right lobe of the liver; thus, avoiding large hepatic vessels and their large branches, liver edges, and motion artifacts, and on four-section slices. The LS value (kPa) was calculated as the median value of four ROIs on four slices. In order to obtain the CV, approximately 1-cm2 (0.96-1.47 cm2) ROIs were drawn in the liver right anterior segment average of five times at the portal vein hilum level. The SD value of five ROIs was used for the CV calculation in each patient, as the SD of the LS values on four, consecutive MRE slices was thought to represent the heterogeneity of HF over the regions of the liver, rather than a measurement error. As with SWE, the stiffness measurement of MRE was considered unreliable when the CV of the measured stiffness values was larger than 30% as these LS values were regarded as unreliable results.
Histopathologic Analysis
Small surgical biopsy specimens were obtained from donors, and explanted liver specimens were obtained from LT recipients. The specimens were fixed in a formalin-alcohol-acetic solution and were embedded in paraffin; 4-mm-thick sections were then cut and stained with hematoxylin-eosin. All specimens were analyzed by one expert hepatopathologist with seven years of clinical experience interpreting liver pathology examinations, and who did not know the results of either examination or the clinical data. The grade of necroinflammatory activity (A) and the fibrosis stage (F) were semi-quantitatively evaluated. The liver necroinflammatory activity and the fibrosis stage were assessed, according to the Standardized Guidelines proposed by the Korean Study Group for the Pathology of Digestive Diseases (34-36). The grade of necroinflammatory activity consisted of lobular activity (L) and porto-periportal activity (P), both of which were graded from 0 to 4 where 0 = none, 1 = minimal, 2 = mild, 3 = moderate, and 4 = severe. Fibrosis was also graded as F0-F4 as follows: F0 = no fibrosis; F1 = portal fibrosis; F2 = periportal fibrosis; F3 = septal fibrosis; and F4 = cirrhosis (36).
Statistics
To evaluate the agreement of LS measurements of the two examinations, Bland-Altman analysis was used in a log scale (37-39). Pearson's correlation coefficient was obtained to evaluate the correlation between the two examinations in the donor candidates, in the LT recipients, and in the 69 patients, including donors and recipients. Linear regression was also performed to assess the correlation between the two techniques. The CV on MRE and SWE was obtained in the total patient population, in the donor group and in the LT recipient groups. The CV of MRE and SWE were calculated as CV = (SD / mean LS value on MRE or SWE) × 100%. Receiver operating characteristic (ROC) analysis was conducted to evaluate the diagnostic performance of MRE or SWE for excluding the presence of HF. A p value of less than 0.05 was considered significant.
RESULTS
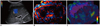
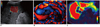
The median LS values measured on SWE were significantly higher than those on MRE in liver donors (p < 0.0001), as well as in F4 patients (p = 0.0005). In donor candidates, the median LSM was 1.78 ± 0.22 kPa on MRE and 4.56 ± 1.44 kPa on SWE (Fig. 2) and in recipients with cirrhosis (F4), the LSM was 6.03 ± 3.02 kPa on MRE and 36.7 ± 39.7 kPa on SWE (Fig. 3, Table 1).
The Technical Success Rate of MRE and SWE
The technical success rates of MRE and SWE were 96.4% (160/166) and 92.2% (141/153), respectively, and there was no significant difference between the two examinations (p = 0.17). Among the 80 LT recipient candidates who underwent SWE, there was technical failure in 12 patients, suggestive of 85% success rate. Conversely, among the 75 LT recipients who underwent MRE, technical failure was seen in six patients, suggestive of 92% technical success rate. Alternatively, there was no instance of technical failure in the liver donor candidates who underwent MRE (n = 91) and/or SWE (n = 73). In addition, 20 of the 80 recipients showed CV >30%, which suggested 13.1% of unreliable LSM on SWE. Conversely, on MRE, there were no patients with unreliable LS measurements. Therefore, when we counted the cases of reliable LS measurements on both MRE and SWE, there was a significant difference in the reliable LS measurements rates between MRE and SWE, i.e. 96.4% for MRE and 79.1% for SWE, respectively (p < 0.0001) (Table 2).
Correlation between MRE and SWE
In the 69 patients who underwent successful MRE and SWE, the LSMs on SWE and MRE showed a moderate correlation (r = 0.66, p < 0.0001). The correlation coefficients between MRE and SWE were 0.37 in liver donors and 0.44 in patients with cirrhosis (F4). According to the linear regression analysis, the coefficient of determination (r2) was 0.41 (p < 0.001) (Fig. 4A). Given that shear modulus was calculated on MRE, whereas Young's modulus was calculated on SWE and in physics, the young's modulus and shear modulus are related by a simple scale factor of 3; for Bland-Altman study, we converted the measured LSM (shear modulus) with MRE into modified LSM (Young's modulus) by multiplying it by 3 (Table 1). The Bland-Altman analysis also demonstrated that the mean difference value of LSM on SWE and modified LSM on MRE was 6.4 ± 24.4 kPa, and the upper and lower limits of agreement (mean ± 2 SD) were 54.2 kPa and -41.4 kPa, respectively. The 95% confidence interval (CI) for the upper limit of agreement was 44.1 to 64.2 kPa and 0.5 to 12.3 kPa for the lower limit. The difference of the log scaled LSMs on MRE and SWE versus the average of the log scaled stiffness values on the two studies did not show a systematic error (Fig. 4B).
More specifically, among the 42 liver donors, the mean difference of LSMs between the two examinations was -0.7 ± 1.4 kPa. The upper and the lower limits of agreement were 2.0 kPa (95% CI: 1.2 to 2.7 kPa) and -3.5 kPa (95% CI: -1.17 to -0.3 kPa), respectively. Alternatively, among the 27 LT recipients who were histologically diagnosed as F4, the mean difference of the LSMs between SWE and MRE was 17.6 ± 36.6 kPa, which was significantly higher than that seen in liver donors. The upper and lower limits of the mean difference in LT recipients were 89.3 kPa (95% CI: 64.3 to 114.3 kPa) and -54.1 kPa (95% CI: -79.2 to -29.1 kPa).
SD and CV of the Measured LS Values
In the 69 patients, the SDs of the LSMs on MRE and SWE were 0.38 ± 0.60 kPa (0.02-2.98) and 5.08 ± 11.5 kPa (0.1-60.96), respectively. The SD of the LSMs was significantly higher in the liver recipient group than in the liver donor group on both MRE (p < 0.001) and SWE (p = 0.0016): the SD values of the LSMs were 0.10 ± 0.05 kPa on MRE and 0.74 ± 0.62 kPa on SWE in liver donors, whereas the SD values of the LSMs were 0.81 ± 0.80 kPa on MRE and 8.73 ± 11.05 kPa on SWE in LT recipients, respectively (Table 1).
In addition, the CVs were significantly higher on SWE (22.1 ± 20.4%) than on MRE (8.3 ± 5.6%) (p < 0.0001). In the donor and recipient subgroups, the CV of SWE was significantly higher than that of MRE (p < 0.0001); CVs of SWE and MRE in the donors were 16.2 ± 13.98% and 5.97 ± 11.5%, respectively, and the corresponding values in the recipients were 31.3 ± 25.2% and 11.9 ± 6.5%. The recipients (31.26 ± 25.15% of SWE, 11.9 ± 6.5% of MRE) also showed significantly higher CVs than the donors on both examinations (16.23 ± 13.98% of SWE, 5.97 ± 3.39% of MRE) (p = 0.008 and p = 0.0001) (Table 1).
Diagnostic Performance of MRE and SWE for Excluding the Presence of Fibrosis (F0)
According to the ROC analysis, the area under the ROC curves were 1.0 (95% CI: 0.948-1.000) on MRE and 0.989 (95% CI: 0.927-1.000) on SWE, and there was no significant difference (p = 0.19). The cut-off value was < 2.36 kPa on MRE, thus providing 100% sensitivity and 100% specificity for diagnosing F0. The cut-off value was 5.6 kPa on SWE, thus providing 100% sensitivity and 90.5% specificity for diagnosing F0.
DISCUSSION
In our study, we found that there was a moderate correlation in LSMs on both SWE and MRE. Our study results are in good agreement with those of the previous studies, which compared the stiffness values of MRE and TE in a phantom or in in vivo human liver (40, 41). However, in our study, the correlation between SWE and MRE (r2 = 0.42) was inferior to that seen in previous studies (r2 = 0.93), which compared MRE and TE (40, 41). The reason for the discrepancy between our study results and of those previous studies (40, 41) could be attributed to the several differences between TE and SWE for creating shear waves. First, the ways to produce shear waves in TE and SWE were different. On SWE, used in our study, shear modulus could be directly calculated by measuring the shear wave velocity created by the acoustic radiation force impulse, whereas on TE, shear waves were induced by mechanical vibrations of mild amplitude and low frequency, which are transmitted by an US transducer probe that is mounted on the axis of a vibrator (41-44). Second, we assume that the directions of the push pulses of the two examinations differ and that those different directions of the push pulses, i.e., longitudinal vs. transverse, may affect the LS values (2, 14, 44, 45). On MRE, the longitudinal vibration at 60 Hz produced by the passive drivers along the lower chest wall creates the shear waves, which proliferate along the vertical axis. Alternatively, on SWE the longitudinal focused US pulse (push pulse or acoustic radiation force impulse) progresses along the vertical axis of the sonic propagation and generates shear waves on the transverse axis. Although the three directions of motion are captured and integrated on each examination, the shear wave speed differs in the different directions, especially in the tortuous structure of liver cirrhosis. This may explain why the difference between the two examinations was greater in the cirrhotic livers. The difference of the frequency of vibration of MRE (60 Hz) and SWE (50 Hz) may also contribute to the discrepancy between the two examinations as the use of higher frequency increases the shear modulus (46). In addition, the LSMs of SWE were significantly higher than those of MRE in both the normal livers and in cirrhotic livers. Therefore, our study results suggested that although there is a clear tendency toward a positive correlation between the two examinations, each LS value obtained on the two examinations is not interchangeable.
Regarding the technical success rates of SWE and MRE, they were 92.2% (141/153) and 96.4% (160/166), respectively, and there was no significant difference in technical success rates between the two examinations (p = 0.17). All technical failures occurred in liver recipients with liver cirrhosis and they did not occur in liver donor candidates. SWE also showed 13.1% of unreliable LSM, although MRE did not show unreliable LS measurements. Therefore, when we counted the cases of reliable LS measurements on both MRE and SWE, there was a significant difference in the reliable LS measurements rates in MRE and SWE, i.e., 96.4% for MRE and 79.1% for SWE (p < 0.0001). Our technical failure results with SWE (7.8%) were inferior to those of TE (4%) obtained in the previous study (20), although our MRE results (3.6%) were similar to those of the previous MRE study (4%) (47). With regard to the unreliable measurements of LS, in our study SWE (13.1%) showed similar or slightly better results than those of TE (17%) seen in the previous study (20). Considering that our study population included many LT recipients with severe hepatic dysfunction and who were not able to cooperate with even short-time breath hold as they were instructed to do, relatively lower technical success rates would have been expected. Also, the markedly decreased liver volume made it difficult to have a clear sonic window in order to place an ROI on SWE. In our study, both MRE and SWE were effective examinations for patients who were able to cooperate well for breath control, although both examinations have only limited applicability in advanced liver cirrhosis patients with poor breath-holding capability. With regard to MRE, iron deposition, which is common in cirrhosis, is a well-known compounding factor that interferes with shear wave visualization on the gradient echo sequence. Shear wave interference can also cause artifacts in the stiffness calculation determined on MRE (48).
A higher CV of the LS values was also found on SWE compared with that on MRE, although the sampling volume was smaller on SWE than on MRE. These results are also in agreement with the results of a previous study (49). The probe position, angle, and the distance from the measurement site during the SWE examination may influence the direction of the push pulse, and consequently the LS measurement (49). It is of note that in our study, the CV values of the measured stiffness values in LT recipients were larger than those of the liver donors on both SWE and MRE examinations. These results were expected because of the limited resolution of the LFE algorithm of MRE for revealing wide wavelengths, as well as of the limited temporal resolution related to the shorter propagation time of the shear waves of SWE, which decrease the accuracy of the stiffness estimation of both techniques (18, 32, 49, 50). Nonetheless, as expected, liver cirrhosis showed a wide range of SD values of LS values, and which suggests the heterogeneity of liver with HF.
Given the basic differences in MRE and SWE, each technique may have its own advantages and disadvantages for the evaluation of HF. MRE provides a spatial map of stiffness at different locations throughout the liver, and more comprehensive data regarding the LS (31), as well as providing a multiparametric approach for HF and focal liver lesions at the same time. MRE results are also highly reproducible (51, 52) even in obese patients or in patients with ascites. It also showed better diagnostic performance than TE (52). On the other hand, SWE provides an average stiffness estimate from a small sampling area in the liver. However, SWE is a portable and inexpensive examination, which requires a shorter procedure time (< 2-5 minutes) at the patient's bed side, and it provides immediate results comparable to those of MRE. As the LS value correlates to the severity of HF and may, therefore, predict the clinical outcomes of HF, including the development of HCC (53-56), the role of stiffness imaging has been expanding rapidly. Due to the various advantages of elastography based on MR and US, patients can undergo follow-up examinations using differing modalities. Therefore, cross-validation of the two examinations is essential in order to establish the optimal follow-up strategy in HF. In our study, MRE and SWE showed similar diagnostic performance for excluding the presence of HF. As SWE showed a higher incidence of unreliable LSMs in cirrhotic liver, MRE may have a more significant role than SWE for the evaluation of liver cirrhosis and portal hypertension. However, for the evaluation of cirrhosis detection and determination of the HF staging capability, further studies will be required, including those with patients in various stages of HF.
Our study has several limitations. First, we only included living liver donors and LT recipients. Therefore, we could not evaluate the real diagnostic performance of SWE and MRE techniques for the staging of HF. However, the primary goal of this study was to cross-validate LS measured on SWE and on MRE in the same individuals, rather than evaluating the diagnostic performance of these two modalities. Second, this retrospective study may have a selection bias due to its retrospective nature. Third, the amount of liver necroinflammatory activity and the fibrosis stage were evaluated, according to the Standardized Guidelines Proposed by the Korean Study Group for the Pathology of Digestive Diseases rather than by the METAVIR scoring system, which is used worldwide for liver fibrosis staging (34-36). Fourth, all of the MRE and SWE examinations in our study were performed using the same MR or US scanner. Therefore, it might not be possible to extrapolate our study results to those of an actual clinical situation in which multiple MR examinations would be performed using various MR scanners or multiple US scanners. Therefore, further studies with a larger number of patients may be required using different MR scanners or US scanners obtained from more than one manufacturer.
In conclusion, detailed in vitro cross-validation of MRE and SWE in liver donor candidates and LT recipients with end-stage liver diseases, has demonstrated moderate correlation in the measurement of LS of the liver. Despite the potential limitations of both elastography techniques, we expect that these two, noninvasive methods can provide clinicians with important new options as potential alternatives to liver biopsy for improving the quality of care for those patients with liver diseases, in terms of the diagnosis, prognosis, and monitoring of fibrosis progression as well for evaluating the treatment efficacy.




 XML Download
XML Download