

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Image-guided radiofrequency ablation (RFA) has been widely accepted as a minimally invasive treatment option for primary and secondary liver malignancies as it has several advantages, including less morbidity and mortality (1). However, until now a major limitation of image-guided RFA is its higher local recurrence rate compared with those of surgical resection, although several previous studies showed that both RFA and surgical resection provided comparable five-year survival rates for patients with hepatocellular carcinomas (HCCs) (2). The main cause of the higher local recurrence rate of RFA, in the range of 1.7-14% (3-7), is perhaps its inability to reliably create adequate volumes of complete tumor destruction with sufficient safety margins. In clinical practice, the overlapping ablation technique with the single placement of an electrode, is widely used to create a sufficient coagulation volume which can include the target tumor, although this technique is technically challenging due to the echogenic bubble clouds created during the procedure. To overcome this major obstacle, several researchers have shown that RFA using new electrodes, such as the multi-tined expandable needle electrodes with saline infusion, perfusion electrodes, or RFA in a different mode of radiofrequency (RF) energy applications and using multiple electrodes, such as the multipolar mode or the switching monopolar mode, was able to create a larger ablation and were more efficient for creating coagulation (8-14).
In order to improve the efficiency of the multiple-overlapping technique for creating a large ablation which can provide enough safety margin of 0.5-1 cm around the target tumor in a reasonable time, a separable clustered electrode (Octopus®, STARmed Co., Ltd. Goyang, Korea) was developed which has a specialized handle portion that can be incorporated into a larger handle in a single unit. Recently, Lee et al. (15) demonstrated that RFA using 17-gauge Octopus® (17-G Octopus®) electrodes with three, separate, individual electrodes at a 10-mm inter-electrode distance, was able to provide greater efficiency for creating larger coagulation than conventional, monopolar RFA using clustered electrodes at a 5-mm interelectrode distance. However, in their study, the minimum effective diameters of the coagulation necrosis created by the clusted electrode and the Octopus® electrodes, were 2.99 cm and 3.49 cm, respectively. Therefore, the tumor size which could be successfully treated with a single placement of the Octopus® electrode, was 2.5 cm if creation of a 5-mm safety margin around the tumor was the goal of the procedure. There is subsequent room to develop an electrode with better efficiency for creating coagulation necrosis during each use.
According to a previous report by Goldberg et al. (16), there was a linear correlation between increase of the electrode gauge from 12-through 24-gauge (G) the ablated lesion diameter. Increasing the electrode gauge can increase the contacted surface, thereby increasing the active electric field. As the heat production caused by RFA in tissue is directly proportional to the total amount of RF energy delivered, if we enlarge the diameter of the electrode, we should be able to create larger coagulation necrosis. Until now, the diameters of commercially available elctrodes were in the range of 17 to 14 gauge (17). Although there is some concern over higher complication rates, including bleeding or tissue laceration, related to larger diameter electrodes, there was no difference in the complication rates in the study using a 17-G, cooled-tip electrode or a 14-gauge electrode with multiprongs (18). Therefore, we assumed that RFA using three, 15-G, Octopus® electrodes may improve their ability to create a large coagulation necrosis each time, without increasing the frequency of major complications, compared to the use of a 17-G electrode.
Before its clinical application, we attempted to demonstrate the in vivo efficacy of RFA using 15-G Octopus® electrodes to create a large area of coagulation necrosis. We also evaluated their in vivo safety regarding possible postprocedural bleeding or potential mortality.
Go to : 
MATERIALS AND METHODS
Our Institutional Animal Care and Use Committee approved (IACUC No. 10-0024) this animal study.
RF Equipment
In this experiment we used a multichannel RF generator (SSP-2000; STARmed Co., Ltd., Goyang, Korea), consisting of three generators with a maximum power of 200 W for each at a frequency of 480 kHz. With the multichannel RF generator, we used a 15-G Octopus® electrode with 2.5-cm active tips (STARmed Co., Ltd., Goyang, Korea) in either the monopolar or switching monopolar mode in order to create a larger coagulation.
Electrode Design
The 15-G Octopus® electrode (Octopus®, STARmed Co., Ltd., Goyang, Korea) was developed in order to improve the efficiency of RFA for creating a large ablation. Basically, the Octopus® electrode is composed of three, cooled-tip electrodes with a 2.5-cm active tip similar to that of a clustered electrode (15). However, the Octopus® electrode differs from the conventional clustered electrode regarding the separability of each individual electrode using a special adaptor which connects the three cables to one piece. As each electrode has a 50-cm-long, flexible cable, an Octopus® electrode can be placed in the liver with a variable, inter-electrode distance determined by the size of the tumor (Fig. 1).
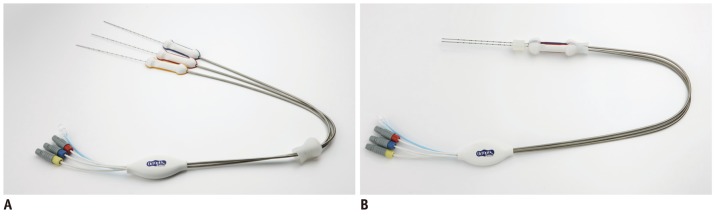 | Fig. 1Photographs of Octopus (R) electrodes which is composed of three, cooled-tip electrodes with a 2.5-cm active tip.
A. Each individual electrode can be separated with variable inter-electrode distance depending on tumor size and shape. B. Each electrode can be also combined, similar to clustered electrode, using special adaptors which assemble three electrode holders to one piece. Photograph of Octopus® electrodes, all of which have three individual needles. Each individual electrode can be combined (A) or separated (B) with variable inter-electrode distance depending on tumor size and shape.
|
Animals, Anesthesia, and Surgery
We obtained approval of this protocol from the Animal Use and Care Administrative Advisory Committee of our institution. All experiments were designed and performed in accordance with the general guidelines issued by the National Institutes of Health for the care of laboratory animals (http://oacu.od.nih.gov/regs/guide/guide_2011.pdf). When we performed surgery, we placed 14, domestic, male pigs (mean weight, 70 kg) under inhalational anesthesia using isoflurane (IsoFlo, Abbott Laboratories, Abbott Park, IL, USA) following an intramuscular injection of 30 mg/kg of Zolazepam hydrochloride (Zoletil, Virbac, Carros, France) and 5 mg/kg of xylazine (Rumpun, Bayer Korea, Ansan, Korea). The pigs were placed in a supine position and were draped in the sterile manner. After draping, an upper midline incision was made which extended from the xiphoid process to the umbilicus. In order to minimize potential variations in the RFA procedures, two authors performed all of the ablations with one or two ablations performed in each pig during the entire experiment.
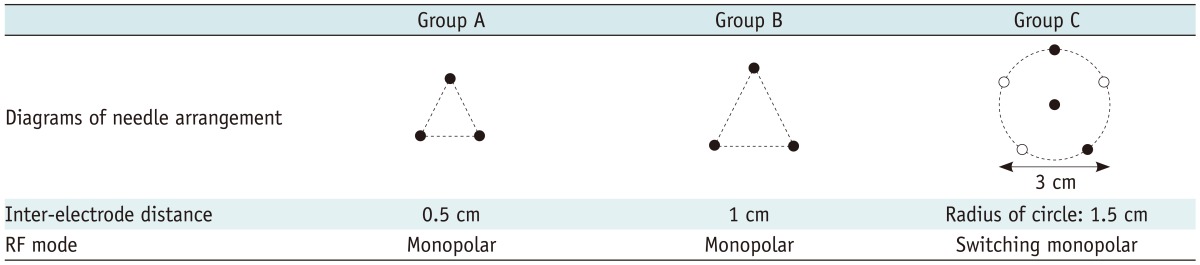
The current in vivo experiment was performed using three groups of pigs (Table 1). Groups A and B were used for testing the efficiency of the 15-G Octopus® which could be used in the percutaneous RFA model, and group C was used for testing the efficiency of multiple, 15-G Octopus® electordes which could be used in the intraoperative RFA model. Using 15-G Octopus® electrodes, a total of 18, RF-induced coagulation lesions were created: group A, monopolar RFA using a single Octopus® electrode with a 5-mm, inter-electrode distance for three, individual electrodes (n = 4); and group B, monopolar RFA using a single Octopus® electrode with a 1-cm, inter-electrode distance for three, individual electrodes (n = 6). In groups A and B, RF energy was delivered to the electrodes for 18 minutes, and the energy delivery was done at the maximum wattage, i.e., 200 W, using an impedance-controlled algorithm in order to optimize energy administration to the tissue. In group C, switching monopolar RFA using two, Octopus® electrodes composed of six, individual electrodes arranged in a pentagonal fashion 1.5 centimeters from the center (n = 8) and with an additional electrode in the center. During the RFA procedure, the temperature at the tip of the electrode was automatically and continuously measured within the generator. Based on the previous ex vivo optimization study (15), RF energy was delivered to the electrodes for 24 minutes.
CT Examination Performed to Evaluate Procedure-related Complications
All pigs underwent a dynamic CT study seven hours following the procedure in order to evaluate any procedure-related complications, such as bleeding or possible injury to another internal organ. The CT examinations were performed on a multi-detector CT scanner (SOMATOM Definition; Siemens, Forchheim, Germany) with 1.5 mL/kg of nonionic contrast medium (Ultravist 370, Bayer, Wayne, NJ, USA).
Assessment of Coagulation Necrosis
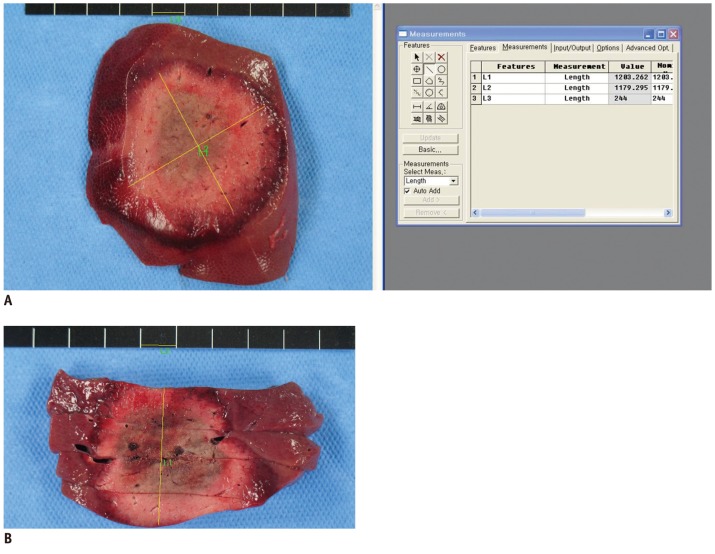
All of the pigs were sacrificed by intravenous injection of potassium chloride which was administered eight hours after the CT scan; all livers were removed en bloc. Livers containing RF-induced coagulation were sliced in the transverse plane perpendicular to the electrode tracks. A histopathologic study was then performed on the specimens and included staining for mitochondrial enzyme activity by incubating the representative tissue sections for 30 minutes in 2% 2,3,5-triphenyl tetrazolium chloride (Sigma, St. Louis, MO, USA) at 20 to 25℃. This test was performed to determine the possibility of irreversible cellular injury sustained during the early stages of RF-induced necrosis. After staining, the slices were placed on an optical platform for photography (N90s, Nikon, Dusseldorf, Germany), and the images were saved to an image management software program (PhotoShop; Adobe, San Jose, CA, USA). Diameter measurement and area analysis were performed on a computer equipped with Image-Pro Plus (Media Cybernetics, Inc., Acton, MA, USA) and Image J software (http://rsbweb.nih.gov/ij).
Two observers (radiology technicians with three years of clinical experience with animal experiments) who were blinded to the information regarding the RFA techniques used in the study, measured the maximum (Dmx) and minimum (Dmi) diameters of the central, white region of the RFA zones on the slice showing the maximum area; they also measured the vertical diameter (Dv) as determined by consensus. To determine the volumes of the RF zones as well as the effectively ablated volumes (Volume-eff), we used the following formulas:
After the gross examinations and analyses, all of the RF-induced, ablated regions were then fixed in 10% formalin for routine histological processing and were finally processed using paraffin sectioning and hematoxylin-eosin staining as used for a light microscope study.
Statistical Analysis
For all of the in vivo experiments, the results were reported as median values. The Dmx and Dmi diameters of a coagulation zone perpendicular to the device axis, were used as measures of the primary outcome in all of the statistical analyses. In order to test the variability of the coagulation necrosis dimensions in the three groups, we calculated the coefficient of variation (CV) of Dmi and the coagulation necrosis volume. CV was defined as the ratio of the standard deviation to the mean size of the coagulation necrosis in each group. Statistical analysis was performed using the Summary statistics, Mann-Whitney test, and the Wilcoxon test with MedCalc statistical software, version 12.2.1 (MedCalcSoftware, Mariakerke, Belgium).
Go to :
RESULTS
In all cases, the temperature of the ablated area was maintained above 50℃ during RFA. All of the pigs except one tolerated RFA under laparotomy. In this pig, sudden cardiopulmonary failure occurred during the RFA procedure.
Gross and Histopathologic Results
Overall, the ablated lesions were round or elliptical in shape in all of the experimental groups of pigs (Fig. 2). The mean values of the circularity measured with Image J, were 0.68, 0.78, and 0.68 in groups A, B and C, respectively. Histopathologically, in all cases the ablated regions contained a central necrotic zone surrounded by a peripheral hemorrhagic zone consisting of necrotic hepatocytes, interstitial hemorrhage, and polymorphonuclear leukocyte infiltrates. Within the central necrotic zone, no viable cells were found, although within some of the hemorrhagic lesions, areas of sinusoidal congestion and hemorrhage were accompanied by advanced necrotic changes and patches of living cells.
Size of the Coagulation
The mean ablated volumes (Volume) and Volume-eff of each group were 49.23 cm3 and 51.40 cm3 in Group A, 64.11 cm3 and 69.42 cm3 in B, and 72.35 cm3 and 76.28 cm3 in C, respectively. There was no significant difference between the ablated Volume and the Volume-eff according to the Wilcoxon test performed in each group (p > 0.05).
The mean values of Dmx and Dmi were 5.68 cm and 4.58 cm in Group A and 5.97 cm and 4.97 cm in Group B. In Group C, the mean diameters of Dmx and Dmi were 6.80 cm and 5.11 cm, respectively. The mean ratios of Dmi/Dmx were 1.25, 1.20, and 1.35 for each group.
The CV values of Dmi and the Volume were 0.11 and 0.29 in group A, 0.07 and 0.49 in group B, and 0.19 and 0.53 in group C, respectively (Table 2).
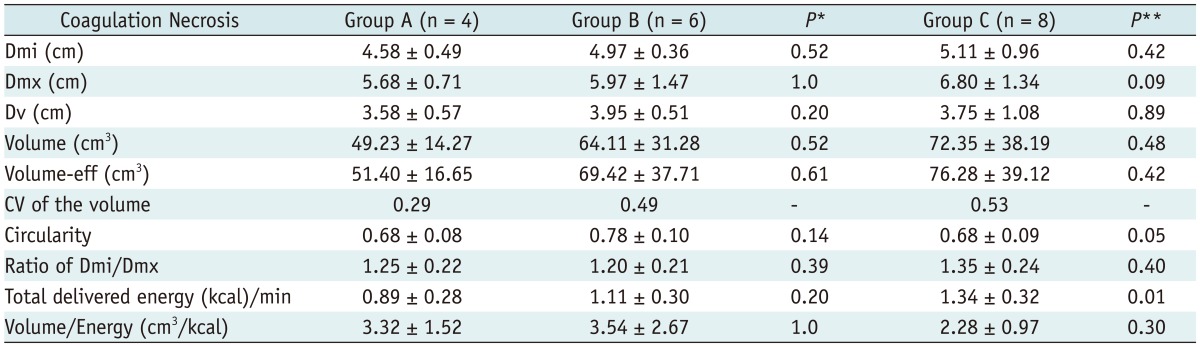
Table 2
Mean Values of Each Parameter in Each Group
Note.- Values are mean ± standard deviations; *P stands for statistical difference between group A and group B and **P represents difference between group A + B and group C. Dmi = minimum diameter of ablation zone, Dmx = maximum diameter of ablation zone, Dv = vertical diameter of ablation zone, Volume = ablated volume, Volume-eff = effectively ablated volume, CV = coefficient of variation
![]()
Electrical Measurements
The mean of the total delivered energy according to the ablation duration (per minute) in groups A, B, and C were 0.89, 1.11, and 1.34 kcal/min, respectively. The ablated volumes per each energy delivery, which refers to the energy efficiency, were 3.32 cm3/kcal in group A, 3.54 cm3/kcal in B, and 2.28 cm3/kcal in C, respectively.
Procedure-Related Complications
As described above, there was one death of unknown cause during the RFA procedure. However, the seven-hour delayed CT scans revealed that there were no significant post-RFA complications such as bleeding or damage to another internal organ. In addition, the autopsy revealed that there was no severe bleeding, liver laceration or unexpected burn injury to the adjacent organs. Therefore, although the exact cause of death in this pig remained unknown, acute cardiac distress caused by RF energy could have been the possible cause of death.
Among all the 14 pigs, portal vein thrombosis was developed in 3 pigs after RFA; two cases of the left main portal vein thrombosis and one case of peripheral portal vein thrombosis. There was not any case of hepatic venous thrombosis or bile duct injury on seven-hour delayed CT scans.
Go to :
DISCUSSION
In our study, RFA using a single Octopus® electrode in the conventional monopolar mode or two Octopus® electrodes in the switching monopolar mode, created a coagulation zone with a minimum diameter of 4.6-5.1 cm. Considering that creating at least a 5-mm safety zone around the tumor is necessary in order to decrease local recurrence after RFA for primary and secondary liver malignancies, our study results indicate that RFA using an Octopus® electrode can successfully treat a 3.5-cm-diameter tumor without creating an overlapping ablation. In clinical practice and under ultrasound guidance, it is quite difficult to reposition the probe during overlapping ablations as numerous microbubbles form in the heated tissue during RFA and may thus also make it difficult to see the electrode tip and the untreated portions of the target tumor on ultrasound (17). One of the advantages of the Octopus® electrode is that it can be separated into three, separate electrodes or can be assembled into a single unit similar to the cluster electrode (Cool-tip™; Covidien, Burlington, MA, USA). Therefore, with the Octopus® electrode, the operator can place each of the three electrodes in the most desirable position before delivery of the RF energy, and can then choose the RF energy delivery mode using either the conventional monopolar or switching mode. We believe that this factor also may help to lower the local tumor recurrence rate after RFA by ensuring an adequate safety margin even with only a single application of RF energy, and it may also increase the RFA indications to include larger liver malignancies.
In our study we also compared the in vivo efficiency of conventional monopolar RFA using the 15-G Octopus® electrodes at different inter-electrode distances, i.e. 5 mm vs. 10 mm. Although a 10-mm inter-electrode distance was used in the group B pigs and created a larger coagulation necrosis than that of group A at the 5-mm inter-electrode distance, it did not attain statistical significance (p > 0.05). However, the coefficient of variation which indicates the extent of the variability of coagulation necrosis related to the mean size of the coagulation, was much higher in group B than in group A. Therefore, further studies at inter-electrode distance between 5 mm and 1 cm may be necessary in order to demonstrate the maximum performance of the Octopus® electrode in creating coagulation necrosis. In our study, the mean value of the ablated volume using the single 15-G Octopus® electrode method with a 1-cm inter-electrode distance (group B) was 64.11 cm3. According to a previous literature report (15), the mean value of the ablated volume using a single 17-G Octopus® electrode was 33.08 cm3 under the same conditions. Based on these results, we suggest that a 15-G Octopus® electrode may exhibit better performance than that of a 17-G Octopus® electrode under the same conditions. Furthermore, our study also reveals that there is no additional risk using the 15-G bore size of electrodes in terms of procedure-related bleeding or injury to other internal organs. Therefore, for large-sized tumors as well as for creating adequate safety margins, we suggest the use of a 15-G Octopus® electrode which may not cause additional complications.
In addition, in group C, although RFA using two Octopus® electrodes in the switching monopolar mode created a larger area of coagulation necrosis than conventional monopolar RFA using an Octopus® electrode as was done in groups A and B, there was no statistical significance. These results differed from our initial expectations and could possibly be attributed to the improved performance of the 15-G electrode for creating larger coagulation necrosis than that seen in a previous study using a 17-G electrode, and which might be possible with increasing RF energy delivery by increasing the area of the active tip of the 15-G electrode in groups A and B (15). In addition, considering the improved performance of a 15-G Octopus® electrode, swine liver is not an optimal animal model for testing the 15-G Octopus® electrode because it is more widely split and thinner than the human liver. Therefore, the minimum Volume-eff of coagulation necrosis were even larger than the mean Volume in each group because the vertical diameter was limited due to the thickness (height) of the lobes of the swine liver. Therefore, we believe that in group C the performance of switching monopolar RFA using two, 15-G Octopus® electrodes to create a large coagulation necrosis might have been underestimated due to the limited dimensions of swine liver. Further studies on a bovine liver phantom using a perfusion pump may be a better model for testing the efficiency of RFA using multiple Octopus® electrodes (19). Furthermore, in humans, placement of multiple Octopus® electrodes at regular inter-electrode spacing intervals under imaging guidance might be difficult in percutaneous RFA procedures. However, as this might not be a serious problem on laparotomy, our study results may be more easily applicable to intraoperative RFA used to treat patients with large liver tumors.
Our study had several limitations. The major limitation was the small number of animals in each group. Second, as described above, the swine livers are not large enough to test the in vivo efficiency of switching mode RFA using Octopus® electrodes. In particular, RFA in the swine livers in our study was affected by the liver thickness itself, as swine liver is much thinner than human liver. We believe that this factor resulted in the relatively large standard deviation in the size of the coagulation necrosis seen in our study. Third, post-RFA follow-up was limited to only seven to eight hours. Although the length of the observation time might have been long enough to evaluate the short-term safety of RFA using Octopus® electrodes, the long-term safety still remains questionable. Lastly, although a unique feature of the Octopus® electrode is that it allows two different methods of RF energy delivery, either in the conventional monopolar mode or in the switching monopolar mode, in our study we only tested the in vivo efficiency of the 15-G Octopus® electrode in the conventional monopolar mode. Therefore, further studies will be required in order to compare the in vivo efficiency of the Octopus® electrode when used in the switching mode. However, based on the previous study regarding the use of a 17-G Octopus® electrode, switching mode RFA yielded a larger coagulation zone than conventional the monopolar mode RFA (15).
In conclusion, the 15-G Octopus® electrodes were very useful and were also safe for creating a large ablation using both a single-electrode model and a multi-electrode model.
Go to :
 XML Download
XML Download