

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Endoscopic ultrasonography (EUS) is one of the most recent advances in gastrointestinal endoscopy. Available EUS devices include radial scanning and linear array echoendoscopes, as well as catheter ultrasound probes. Endoscopic ultrasonography has various applications, such as staging of gastrointestinal malignancy, evaluation of submucosal tumors, and has grown to be an important modality in evaluating the pancreaticobiliary system. Advances in EUS imaging have enhanced its diagnostic potential. For example, EUS with real time tissue elastography can be more useful than EUS with only a B-mode imaging ability. Elastography is an imaging modality for the evaluation of tissue stiffness, which has been used for the analysis of superficial organs, such as those of the breast and prostate (1, 2). The measurement of tissue elasticity has been reported to be useful for the diagnosis and differentiation of tumors, which are stiffer than normal tissues (3). Endoscopic ultrasonography elastography (EUS-EG) is a promising imaging technique with a high accuracy for the differential diagnosis of solid pancreatic tumors (4-9). Recent introduction of second generation EUS-EG allows for the quantitative analysis of tissue stiffness. Here, we review our knowledge and preliminary experience with the use of EUS-elastography for the diagnosis of pancreatic disease.
The Principles of EUS Elastography
The principle of EUS elastography is explained by using a spring model (Fig. 1). Thus, when a one-dimensionally connected hard spring and soft spring are compressed, the hard spring is negligibly deformed, but the soft spring is compressed. This difference in deformation results in displacement differences among the areas, as well as the amount of distortion obtained by spatial differentiation of this displacement distribution, which provides elasticity information.
Generally, tissue hardness is thought to correlate with malignancy potential; malignant tumors are harder than benign tumors (10). The elastic characteristics of the tissue appear to be fairly uniform throughout the benign lesions. By contrast, cancer grows in a much-unorganized way, such that its elastic properties are rather heterogeneous throughout the tumor. On the basis of this concept, real tissue elastic imaging with EUS has been introduced for clinical use.
The Instruments and Techniques of EUS Elastography
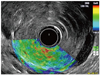
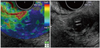
The instruments used at our institute were the EG-3670 URK electronic radial type ultrasonographic endoscope (PENTAX Co, Ltd, Tokyo, Japan) and the EUB-7500HV ultrasound (Hitachi Co, Ltd, Tokyo, Japan). Real-time EUS elastography can be thus performed with the conventional EUS probes without any need for additional equipment that induces vibration or pressure. Due to its similarity with color Doppler examinations, EUS elastography is performed with a two panel image with the usual conventional gray-scale B-mode EUS image on the right side and with the elastography image on the left side (Fig. 2).
A region of interest (ROI) for the elastography calculations is manually selected and should include the targeted lesion, as well as the soft surrounding tissues. The ROI needs to be set to include sufficient surrounding tissue because elasticity values are displayed relative to the average strain inside the ROI. The system also displays a compression threshold which has to be set up between 3 and 4. To visualize tissue elasticity patterns, different elasticity values are marked with different colors (on a scale of 1 to 255) and the sono-elastography information is shown to be superimposed on the conventional gray-scale image. The system is set-up to use a hue color map (red-green-blue), where hard tissue areas appear as dark blue, medium hard tissue areas as cyan, intermediate tissue areas as green, medium soft tissue areas as yellow and soft tissue areas as red.
Recently second-generation EUS elastography allows for quantitative analysis of tissue stiffness. Two different areas (A and B) from the region of interest were selected for quantitative elastographic analysis. Area A is a representative area of the mass and included the biggest possible area of the tumor. Area B refers to a soft (red) peripancreatic reference area outside the tumor. The quotient B/A (strain ratio) is considered as the measure of the elastographic evaluation (Fig. 2). Because selection of area B can to some extent be biased, the elasticity of area A is also independently considered for analysis as another measure of the elastographic evaluation.
In addition, and to limit selection bias of areas A and B, the strain ratio and the elasticity of area A are calculated in triplicate for each patient; the mean of the 3 measures is considered as a reliable result.
Results of EUS Elastography
Normal Pancreas
Elastographic imaging of the normal pancreas is characterized by a uniform, homogenous green color distribution (representing intermediate stiffness) throughout the organ and the reproducibility of the signal is comparatively good (Fig. 3) (4).
We experienced of EUS elastography on 12 healthy subjects. None of the healthy subjects had a history of pancreatic disease, symptoms of dyspepsia, history of alcohol abuse, or increased serum levels of pancreatic enzymes. In addition, none of the healthy subjects was a smoker. On qualitative analysis, a healthy pancreas appears to be predominantly green in color with a homogenous (41.7%) or heterogeneous (58.3%) pattern. On quantitative analysis, a healthy pancreas showed a mean elasticity value of 0.55% (95% CI 0.42-0.68%).
Solid Pancreatic Tumors
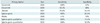
Several recent studies have shown EUS elastography as a promising technique with a high degree of accuracy for the differential diagnosis of solid pancreatic tumors (4-8). Actually, features of the elastographic patterns with respect to homogeneity or heterogeneity, and predominant color, closely correlate with the histologic features of the lesion. In the first study published by Giovanni et al. (4), pancreatic masses appearing mostly blue were considered to be malignant, whereas other patterns were considered as benign (Fig. 4). In a multicenter study including 121 patients with pancreatic masses, sensitivity and specificity of elastography for malignancy were 92.3% and 80%, respectively (7). Iglesia-Garcia et al. (8) published a qualitative analysis of EUS elastography in 130 patients with a solid pancreatic mass. In the study, diagnostic sensitivity, specificity, and overall accuracy of elastography for diagnosing malignancy were 100%, 85.5% and 94%, respectively. However Hirche et al. (9) published disappointing results on the elastography in terms of its ability of predicting the nature of pancreatic lesions with poor diagnostic sensitivity (41%), specificity (53%), and accuracy (45%). Variable diagnostic accuracy among elastographic studies may result from intrinsic limitations of qualitative elastography; it is the subjective interpretation of the elastographic pattern. Igelsia-Garcia et al. (11) published the quantitative analysis for the differentiation of solid pancreatic masses with higher specificity (92.9%) and accuracy (97.7%) compared to the qualitative analysis (Table 1). Based on the results, a strain ratio higher than 6.04 or a mass elasticity lower than 0.05% is 100% sensitive for correctly classifying tumors as malignant. A strain ratio higher than 15.41 or a mass elasticity value below 0.03% is 100% specific for malignancy.
Differential Diagnosis Between Pancreatic Cancer and Chronic Pancreatitis
Differential diagnosis between pancreatic cancer and chronic pancreatitis may be difficult, particularly in cases of advanced pancreatitis (12). Accuracy of EUS in this setting may not be higher than 75% (13). Histology is the gold standard, but even a biopsy can be difficult because cancers can produce a marked fibrotic reaction or necrosis and give false results. EUS-FNA sensitivity and diagnostic accuracy are 75-92% and 79-92%, respectively (14). EUS elastography may add some important information in this setting. Diffuse abnormalities of pancreatic parenchyma in chronic pancreatitis are not a limitation for elastography because only the solid mass under evaluation is included in the ROI. Based on Iglesias-Garcia study, the accuracy of qualitative EUS analysis was up to 20% if inflammatory masses are misclassified as cancer. Importantly enough, false positive but not false negative results for malignancy occurred (6). The quantitative EUS analysis improved the diagnostic accuracy for diagnosing malignancy (8). Therefore EUS elastography might be particularly helpful in situations in which the accuracy of EUS-FNA is suboptimal.
Limitation of EUS Elastography
The main pitfall of EUS elastography is the inability to control tissue compression by the EUS transducer (5). The use of EUS elastography is also hampered by the induction of motion artifacts determined by respiratory or heart movements, which cannot be adequately eliminated or quantified. The presence of nearby structures with very low or high density and stiffness, such as the heart, major vessels or spine are also difficult to be excluded from the ROI analyzed. Selection of the ROI has to carefully include surrounding soft tissues only, since the methodology of elastography assumes computations relative to the average strain inside the ROI. The qualitative pattern analysis of the EUS elastography still images may also be associated with significant intra-and interobserver variability. Adequate and reproducible elastographic imaging of focal pancreatic disease is confined to lesions less than 30 mm in diameter. In larger lesions, elastographic delineation was incomplete.
Summary
Endoscopic ultrasonography elastography is a useful tool for the characterization of solid pancreatic masses. During the EUS procedures, the qualitative and quantitative evaluation of tissue stiffness, which shows an excellent sensitivity and acceptable specificity for the diagnosis of pancreatic malignancy, could be obtained. These results deserve further confirmation in multicenter studies.


 XML Download
XML Download