

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most prevalent malignancies worldwide (1). Monitoring patients at high risk for HCC with imaging studies and blood tests for alpha-fetoprotein levels leads to diagnosis of many cases when there are only one or a few lesions, and the patient is still asymptomatic (2). Furthermore, several nonsurgical modalities have been developed for the treatment of unresectable HCC even with a single HCC, including cryoablation or radiofrequency (RF) ablation, percutaneous ethanol injection (PEI), and transcatheter arterial chemoembolization (TACE). Of those, RF ablation is one of the most widely performed procedures for patients with unresectable HCC because of its effectiveness and safety in the treatment of small (≤ 3 cm) and medium (≤ 5 cm) HCC, with a 3-year survival rate of 62-68%, a treatment-associated morbidity rate of 0-12%, and a treatment-related mortality rate of 0-1% (3-8).
RF ablation has recently gained attention as a more promising technique for the treatment of HCC (8-16). Many investigators have reported that RF ablation for patients with HCC provides favorable survival rates with excellent local recurrence-free rates (17).
Meanwhile, TACE has been widely used in cases of unresectable HCC during the past 20 years. But, some authors report that complete tumor necrosis after TACE is unusual (18), thus alternative treatment is considered. Even when initial remission is demonstrated after TACE, local recurred HCC is frequently observed, and subsequently repeated TACE is considered. To our knowledge, there are few studies evaluating the rate and prognostic factors for local recurrence and survival after RF ablation in patients with incompletely treated HCC who had undergone TACE. The purpose of this study was to retrospectively evaluate the effect of ultrasound-guided RF ablation in patients with incompletely treated HCC after TACE. In addition, possible prognostic factors regarding the efficacy of this therapy were also evaluated.
SUBJECTS AND METHODS
Patients
Between June 2002 and September 2007, 116 consecutive patients with incompletely treated HCCs after TACE were referred to the department of radiology for RF ablation. Inclusion criteria for this study were as follows: 1) a single HCC smaller than or equal to 5 cm in diameter; 2) lesions visible on ultrasonography (US), with an acceptable and safe path between the lesion and the skin as observed on the US scan; 3) no extrahepatic metastases present; 4) no imaging evidence of tumor invasion into the major portal or hepatic vein branches; 5) liver cirrhosis classified as Child-Pugh class A or B; 6) no history of encephalopathy, ascites refractory to diuretics, or variceal bleeding, and 7) no previous treatment for HCC except TACE. Consequently, 39 patients with a single HCC (33 men and 6 women; age range 48-84 years; mean age 66 years) were enrolled in this study. Tumor size ranged from 1.1 to 5.0 cm in diameter (mean, 2.4 cm).
The diagnosis of incompletely treated HCC was made when there were areas within HCC that had not undergone complete necrosis based on the follow-up CT or MR imaging performed within 1 month after TACE. These areas were considered to be present by observing incomplete accumulation of lipiodol within HCC or arterially enhancing portion within HCC on follow up CT or MR imaging (19). Of the 39 patients, 22 patients were treated with one cycle of TACE, 13 patients with 2 cycles and 4 patients with 3 cycles.
Radiofrequency Ablation
All RF ablation was performed percutaneously under real-time sonographic guidance. A 20 or 15 cm long, 17 G, Cool-tip electrode with a 2 or 3 cm long exposed metallic tip (Valleylab, Boulder, CO, USA) was used to deliver radiofrequency energy. A 200 W, 480 kHz monopolar radiofrequency generator (CC-1, Valleylab, Boulder, CO, USA) was used as the energy source. A standard grounding pad (Valleylab, Boulder, CO, USA) was placed on each of the patient's thighs.
RF ablation procedures were performed with the patient under local anesthesia in the ultrasonography suite. The most appropriate approach was determined to avoid damaging large vessels near the targeted HCC, and then a single electrode was directly inserted through the skin and positioned at the center of the HCC under US guidance using a 3.75 MHz convex probe. The tip of the electrode was then further advanced to the deepest margin of the tumor. RF energy was applied for 8-12 min in each treatment session. During the procedure, a thermocouple embedded within the electrode tip continuously measured the temperature of the tip; tissue impedance was monitored by circuitry incorporated within the generator. When the desired current could not be applied without observing an elevation in impedance suggestive of tissue boiling, the generator automatically switched to the pulsed-RF technique. At the end of treatment, the RF ablation application and cooling circuits were simultaneously interrupted, and the heated tissues were allowed to heat the electrode by diffusion until the maximum temperature was recorded. To prevent bleeding, bile leakage, and tumor seeding, the intrahepatic needle track was treated with thermocoagulation and the electrode was removed. Tumors larger than 3.5 cm needed multiple overlapping ablations (20).
Posttreatment Assessment and Follow-up
One hour after the initial treatment, contrast-enhanced dynamic CT was performed. When the thickness of the ablative margin was at least 0.5 cm for ablation of index tumor, the treatment was completed. When a residual enhanced lesion was seen on dynamic CT, an additional RF ablation was performed for the residual enhanced lesion. The effectiveness of the RF ablation technique was evaluated with dynamic CT performed 1 month after the first RF ablation session was performed. When no enhancing lesion was seen on CT, the technique effectiveness was defined as complete. When residual enhancing lesion was still seen on CT, the technique effectiveness was defined as incomplete. The HCCs showing incomplete technique effectiveness were not treated with additional RF ablation but rather with TACE.
Thereafter, the patients were evaluated on scheduled follow-ups every 2-4 months with contrast-enhanced dynamic CT to detect local recurrence. Local recurrence was defined as the development of tumoral enhancement in or around the ablation zone as observed on follow-up CT. Additionally, overall survival was evaluated and defined as the interval between the first RF ablation and either death or last follow-up visit. At each follow-up visit, blood tests, including those for liver function and serum alpha-fetoprotein levels, were performed.
Possible Prognostic Factors Influencing Local Recurrence and Overall Survival
Ten possible prognostic factors were postulated and each was divided into two categories for analyses. The possible prognostic factors were tumor size (≤ 2 cm or > 2 cm maximum dimension), number of previous TACE treatments (1 or ≥ 2), patient age, patient gender, antibody against hepatitis C virus (anti-HCV) (positive or negative), hepatitis B surface antigen (HBs Ag) (positive or negative), Child-Pugh class (A or B), history of alcoholic liver disease (yes or no), level of alpha-fetoprotein (≤ 100 ng/mL or > 100 ng/mL), and interval between TACE and RF ablation (≤ 2 months or > 2 months).
Statistical Analyses
The complete ablation rate and major complication rate were calculated. The local recurrence free rate and overall survival rate were evaluated using the Kaplan-Meier method. Possible prognostic factors influencing local recurrence and overall survival were analyzed using a Cox proportional hazards regression model. The level of significance (p value) was set at 0.05 for all tests. SPSS statistical analysis software (SPSS Inc.) was used.
RESULTS
RF Ablation Procedures and Complications
In 36 (92.3%) of 39 patients, complete tumor ablation was depicted on dynamic CT performed 1 month after treatment (Fig. 1). The 3 patients with a single HCC showing an incomplete response were not treated with a second RF ablation treatment because of the heat sink effect from the adjacent portal vein in one patient and large diameter (5 cm and 3.8 cm, respectively) in other 2 patients (Fig. 2). Afterward, the 3 patients in whom RF ablation treatment failed underwent subsequent TACE.
No procedure-related death was observed. Complications were observed in two (5.1%) of 39 patients. Hepatic abscess, which was a major complication, occurred in one patient. The patient had developed a high fever 7 days after RF ablation and the CT findings in the ablated zone was similar to those of a hepatic abscess. Subsequently, US-guided percutaneous drainage was performed. Portal venous thrombosis was observed in the other patient which was a minor complication.
Local Recurrence Analysis
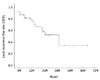
The follow-up periods ranged from 90 to 1950 days (mean 767 days). The local recurrence free rates at 1, 2, 3, and 5 years were 81.7%, 63.1%, 53.6%, and 35.7%, respectively (Fig. 3). During the follow-up period, local recurrence developed in 13 (33.3%) of 39 patients. At the time of local tumor recurrence, distant recurrence was observed in 3 (7.7%) of 39 patients. Tumor diameter was found to be a significant prognostic factor affecting local recurrence (p = 0.047) (Table 1).
DISCUSSION
TACE is a widely used therapeutic modality for unresectable HCC and has an excellent anti-tumor effect (21-23). However, the efficacy of TACE remains controversial (24) because HCC is sometimes resistant to TACE treatment. Hashimoto et al. (25) reported that TACE induced complete necrosis only in 50% of single nodular type tumors.
While treatment of TACE-resistant HCC is a major clinical objective, RF ablation has been accepted as a safe and useful technique for the local treatment of HCC. In the present study, we found that RF ablation for incompletely treated HCC after TACE produced a relatively high complete ablation rate. Our findings are consistent with previous studies. Shibata et al. (26) reported that complete ablation was achieved in 46 (96%) of 48 HCCs (≤ 4 cm) treated with RF ablation. Lencioni et al. (16) reported that complete ablation was achieved in 63 (91%) of 69 HCCs (≤ 5 cm). Moreover, the side effects and the long-term impairment of liver function associated with TACE (27, 28) further supports the use of RF ablation rather than subsequent repeated TACE treatments.
Of the three cases we considered to result in incomplete ablations, two cases were relatively large tumors that were 5 cm and 3.8 cm in diameter, respectively. It was reported that in HCCs less than 3 cm in diameter, complete ablation rate was 90%, but complete ablation rate was 71% in HCCs ranging 3-5 cm and 25% in HCCs over 5 cm in diameter (9, 12, 29). In the third case, we found the HCC was located between large branches of hepatic vessels, so it may have caused incomplete ablation because blood flow promotes heat loss, creating a so called heat sink effect.
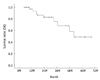
Our study achieved comparable local recurrence-free rates and survival rates as demonstrated in previous studies of RF ablation alone for the treatment. Other studies have reported rates of local recurrence after RF ablation for HCC of 19% to 36% (30-35), which is in accordance with the results of our study. Also, numerous studies demonstrated the 5-year post-RF ablation overall survival rates ranged from 33% to 58%, supporting that RF ablation may be accepted as primary treatment for patients with HCC for whom hepatectomy or liver transplantation was not suitable (5, 8, 17, 31-33, 36).
We were concerned about possible influences of prognostic factors on local recurrence-free rates and survival rates. However, we found only HCC size was a significant prognostic factor in local recurrence-free rates. Local recurrence-free rate was higher in patients with small HCC (≤ 2 cm). Generally, RF ablation treatment is known to induce a spherical thermal lesion measuring approximately 3 cm at its greatest dimension in a single session (37). Accordingly, ablation of HCCs larger than 3 cm may require repeated sessions. Komorizono et al. reported that an HCC dimension > 2 cm was associated independently with local recurrence after a single session RF ablation, which is in accordance with the results of our study (38).
Complications after RF ablation for HCC have been reported. The rate of complications for the treatment of HCC was reported to be greater than 5% (12, 14, 17, 26). The relatively high rate of complications may be due to the prevalence of liver cirrhosis in patients treated. The complications we observed in our investigation were similar to those of studies dealing with HCC associated with liver cirrhosis.
Our study has several limitations. First, this study was retrospectively performed and was not randomized in design. Second, most HCCs were not pathological confirmed. Third, this study included a relatively small number of patients.
In conclusion, ultrasound-guided RF ablation could be an effective and safe method for treating incompletely treated HCC after TACE. The diameter of HCC was a significant prognostic factor for local recurrence.




 XML Download
XML Download