

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant melanomas, which originate from cells of the neural crest, account for 1.5% of all cancers. Although the skin is the most common site for a melanoma to develop, primary malignant melanomas can occur in the central nervous system, rectum, gastrointestinal tract, bronchus, and esophagus. Primary malignant melanoma involving the mediastinum, however, is very rare, and has only been documented in a few case reports (1-5, 8). Only one case has been reported in the radiology literature (4). These tumors may be confused with other mediastinal masses such as lymphomas, thymic carcinomas and malignant germ-cell tumors. Exclusion of other primary melanoma sites is mandatory to confirm a primary mediastinal melanoma. We describe here two adults with pathologically confirmed primary malignant melanomas, which formed a huge anterior mediastinal mass encasing the major vascular structure.
CASE REPORT
Case 1
A 45-year-old man was referred to our hospital for evaluation of alleged cardiomegaly discovered on a chest radiograph. He had a 6-week history of chest pain, dyspnea, and dysphasia. The initial chest radiograph demonstrated a large, well-defined, mediastinal mass obliterating the left cardiac border. Pleural effusion in the left hemithorax was also observed. Enhanced chest CT images showed a 13 × 8.5-cm sized, poorly enhancing mass involving the anterior mediastinum, encasing the aortic arch and large mediastinal vessels. Diffuse narrowing of the left main bronchus was also observed, as were diffuse and nodular pericardial thickening, pericardial effusion, and left pleural effusion (Fig. 1A-C). A small, enhancing lymph node in the left phrenic area and a distant metastasis to the right adrenal gland were also found (not shown).
Whole body 18F-fluorodeoxyglucose positron emission tomography (FDG PET) CT showed a hypermetabolic (maximum standardized uptake value: 16.8), huge malignant mass in the anterior mediastinum with a right adrenal metastasis, but there was no evidence of abnormaluptake at other sites in the body.
Computed tomography-guided percutaneous core needle biopsy of the mediastinal mass was performed. A histologic analysis showed evidence of brown melanin pigment that was immunohistochemically positive for both S-100 and Anti-Melanoma antibody (HMB)-45. The pathologic findings were consistent with primary malignant melanoma in the mediastinum (Fig. 1D).
The patient refused chemotherapy and was discharged after 7 days, with no further oncology follow-up.
Case 2
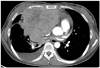
A 41-year-old woman was admitted to our hospital with a three-month history of right shoulder pain. The initial chest radiograph showed a large, lobulating contoured mass in the right hemithorax with obliteration of the right cardiac border. A small amount of pleural effusion was also seen in the right hemithorax. Enhanced chest CT showed a 12 × 9-cm sized, huge, heterogeneously enhancing mass in the anterior mediastinum, displacing and compressing the heart and the great vessels. CT demonstrated right pleural effusion, pericardial effusion, and mediastinal lymphadenopathy (Fig. 2). Abdomino-pelvic CT showed a 3-cm, low-attenuation mass in the pancreatic tail, suggesting metastasis (not shown). There was no evidence of a primary pigmented lesion on the skin or on any other organs. Whole body FDG PET CT showed a hypermetabolic (maximum standardized uptake value: uncertain outside image), huge malignant mass in the anterior mediastinum with pancreatic metastasis, but there was no evidence of abnormal uptake at other sites in the body.
We performed a CT-guided percutaneous core needle biopsy of the mediastinal mass and transbronchial bronchoscopic needle biopsy of the lymph nodes. Histologic examination showed that the tumor cells contained focal melanin pigment and expressed HMB-45, indicating malignant melanoma and metastatic lymph nodes.
The patient was placed on chemotherapy treatment, consisting of dacarbazine and doxorubicin, and was discharged seven days after admission. A follow-up CT scan 2 months later showed that the mediastinal mass had increased in size and that the subcarinal lymph nodes had become enlarged. Four months later, she developed dyspnea and expired.
DISCUSSION
Primary malignant melanoma in the mediastinum is extremely rare, with only a few cases reported to date (1-5, 8). These tumors have been diagnosed only in patients with no history of extrathoracic primary melanoma or other malignancy.
Histologically, melanomas are malignant tumors composed of melanocytes, which are derived from neural crest cells. Neural crest cells are transient and multipotent cells that develop into melanocytes, peripheral and enteric neurons and glia, craniofacial cartilage and bone, and smooth muscle (6). Malignant melanoma most often develops in the skin, but also occurs in the eyes, oronasal mucosa, and anorectal junction, all sites of melanin cell occurrence.
Nevus cells are a variant of melanocytes found in lymph nodes and the thymus. Aggregates of nevus cells in the thymus or a mediastinal lymph node may be sources of malignant melanomas in the anterior mediastinum (5). The autonomic ganglion cells are similarly derived. A case of malignant melanoma of the posterior mediastinum arising from the sympathetic chain was reported (7).
We describe here two patients with huge primary malignant melanomas of the anterior mediastinum. Computed tomography showed that primary malignant melanomas were found to be lobulated masses with mild enhancement in the anterior mediastinum. In both of our patients, the mediastinal masses appeared to involve the pericardium, pleura and lymph nodes, along with distant metastases. MRI scans were not performed in our cases.
A previous case report described the findings on magnetic resonance imaging of a primary malignant melanoma in the anterior mediastinum (4). The mass was mildly hyperintense to muscle on T1-weighted images and heterogeneously hypointense to muscle on T2-weighted images. When correlated with pathology findings, the focal areas of T1 hyperintensity and T2 hypointensity were found to be composed of melanocytes with rich melanin granules (4).
The major considerations of differential diagnosis of primary malignant melanoma in anterior mediastinum include a lymphoma, thymic carcinoma, malignant germ-cell tumor, and, more rarely, a mediastinal soft tissue sarcoma such as an angiosarcoma.
The prognosis of primary malignant melanoma in mediasinum is unfavorable and surgical resection is the best treatment. Systemic chemotherapy and immunotherapy can be used to treat advanced disease (8).
In conclusion, although rare, primary malignant melanoma in the anterior mediastinum can present as a large mediastinal mass with displacement or invasion of the adjacent mediastinal structure, metastatic mediastinal lymph nodes and distant metastasis, similar to CT imaging patterns of other malignant mediastinal masses.

 XML Download
XML Download