

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Metallic stents for inoperable biliary hilar malignancy is a widely accepted palliative treatment (1-10). Although it remains controversial, in hilar malignancies, endoscopic and percutaneous attempts have been made to drain both hepatic lobes utilizing greater than two stents (2-4).
T- and Y-configured stent placements are widely used methods for bilobar biliary drainage that involve two intrahepatic limbs connecting one right-sector duct with the that involves two intrahepatic limbs that connect one right-sector with the left hepatic duct. However, several previous studies have focused on narrowing of the second stent lumen or failure of a second stent insertion in patients with tight strictures (11, 12).
Open cell stents could be easily navigated through tortuous strictures due to their low profile delivery system and high flexibility (13). Furthermore, they can allow full expansion of the second stent at the intersection when assembled in a bifurcating shape (14). In the vascular system, open cell stents are widely used for lesions in bifurcations (15, 16). We aimed to evaluate the feasibility, safety and effectiveness of an assembly of open cell nitinol stents for biliary hilar malignancy.
Go to : 
MATERIALS AND METHODS
Patients
For 10 months between January and October 2007, 26 consecutive patients with malignant biliary hilar obstruction arrived in the interventional radiology suite for percutaneous complex biliary hilar stent placement. The study was conducted under Institutional Review Board approval after informed consent was given by all participating patients. The patients consisted of 21 men and 5 women. Their ages ranged from 41 to 84 years (mean: 64 years). Inclusion criteria were patients with malignant hilar biliary obstruction, who were unsuitable for surgical resection as a result of their tumor extension and physical conditions. Patients who had a large amount of ascites and had a short life expectancy (< 3 months) were excluded. One patient who had sustained cholangitis even after an endoscopic left unilobar stent placement, and who was referred for percutaneous additional stent placement, was enrolled.
In the patient group, the causes of hilar obstruction included: cholangiocarcinomas (n = 16), gallbladder cancers (n = 4), and metastatic cancers (n = 6). The diagnosis was confirmed with tissue samples in 7 patients, through surgical biopsies (n = 2), percutaneous biopsies (n = 4), or endoscopic biopsies (n = 1), and was made in the remaining 19 patients (73%) based on clinicoradiologic findings.
Based on the Bismuth classification system, 3 patients (11%) had type II disease, 9 (35%) had type III, and 14 (54%) had type IV disease. Grading of the tumor extension and determination of the ductal anatomy were based on the findings of multiphase computed tomography (CT), percutaneous transhepatic cholangiography, and transcatheter cholangiography.
Procedures
Sedation and analgesia during the procedures was carried out with an intravenous infusion of remifentanil hydrochloride (Ultiva, GlaxoSmithKline, Abbotsford, Australia). Percutaneous transhepatic biliary drainage (PTBD) procedures were performed under ultrasonographic (US) and fluoroscopic guidance 3-14 days before stent placement. In all patients, the 10 mm diameter Sentinol stent, (Boston Scientific, Natick, MA, USA) preloaded in a 6 Fr diameter 80 cm-long delivery system was used. It is made of laser-cut nitinol, which makes it an open-cell-design stent. Stents were placed according to the ductal anatomy in the hilum. If the hilar angle, which is the angle between the right hepatic duct and the left duct (LHD), was obtuse, two stents were placed in a T-configuration. For an acute hilar angle, two stents were placed in a Y-configuration through bilateral accesses. For a lesion that separated the right anterior duct from the right posterior duct (RPD), two stents were placed in a crisscross configuration, and for a lesion separating all the segmental ducts, multiple stents were placed connecting each major segmental duct.
T-configured stent placement (Fig. 1) was performed with two stents through either the right or left access. The transverse stent was placed first, connecting the right and left lobar duct over a 0.035-inch, 150-cm-long hydrophilic guide wire (Terumo, Tokyo, Japan); then the 2nd stent connecting the transverse stent to the common bile duct (CBD) was inserted over a 0.035-inch, 150-cm-long stiff hydrophilic guide wire (Terumo, Tokyo, Japan), which crossed a cell of the transverse stent and common hepatic duct stricture into the duodenum. For the Y-configured stent placement (Fig. 1), two stents were inserted through both the right and left accesses. The 1st stent was placed connecting one lobar duct and CBD. The 2nd stent was inserted from the contra-lateral lobar duct through a cell of the 1st stent to the CBD over the stiff hydrophilic guide wire. A crisscross-configured stent placement (Fig. 1) was performed with two stents inserted through two unilateral or bilateral accesses. The first stent was placed connecting a right sectoral duct and the LHD. The 2nd stent was inserted from the other sectoral duct crossing the 1st stent to the CBD over a stiff hydrophilic guide wire. When a large area of the undrained segment was excluded from the stent assembly because of anatomical variation (such as RPD joining the CHD or a deeply infiltrating lesion separating each segmental duct) additional stents were inserted connecting the segmental duct to the stent assembly as a multiple intersecting type stent placement (Fig. 2).
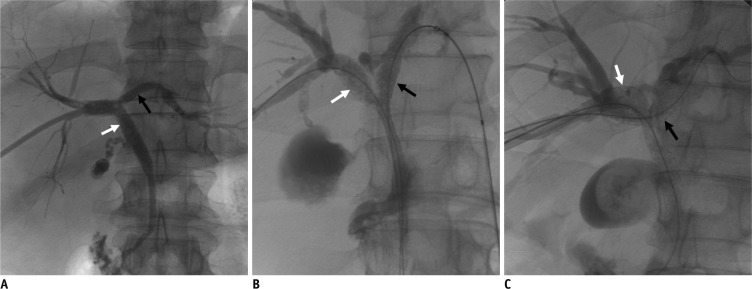 | Fig. 1Stent configurations.
A. T-configured stent placement. 1st stent (black arrow) was placed connecting right and left lobar ducts, then 2nd stent white arrow connecting transverse stent to CBD was inserted through same access. B. Y-configured stent placement. First stent white arrow was placed from right lobar duct to common bile duct. 2nd stent black arrow was inserted from left lobar duct through first stent to CBD. C. Crisscross-configured stent place placement. First stent black arrow was placed connecting one right anterior sectoral duct and left hepatic duct. Second stent white arrow was inserted from right posterior sectoral duct crossing first stent and into common bile duct. CBD = common bile duct
|
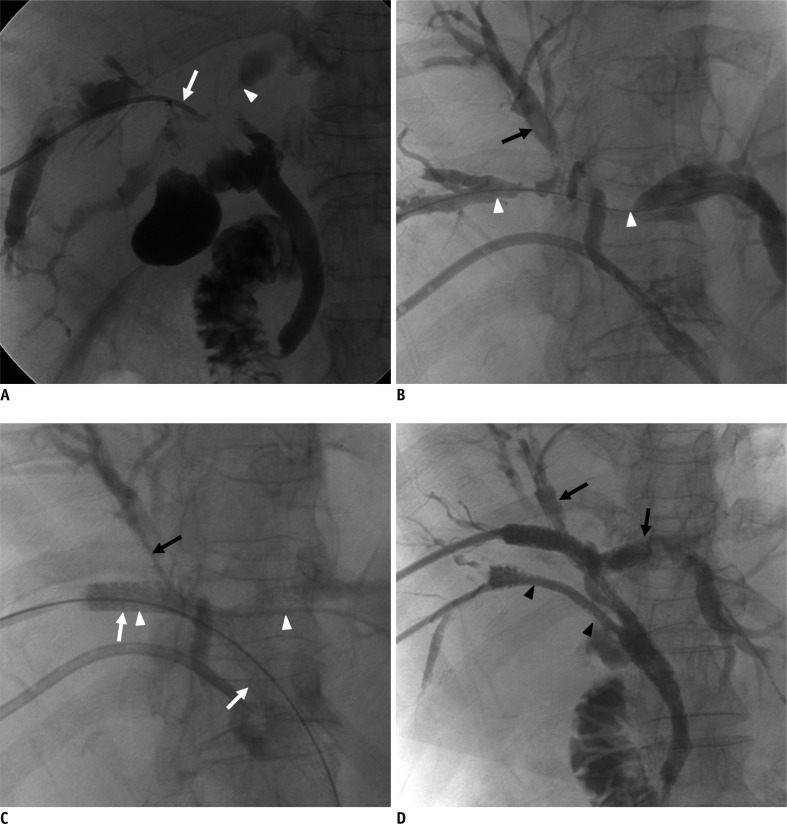 | Fig. 2F/67 patient with cholangiocarcinoma.
A. Right posterior ducts (RPD; arrow) and left hepatic ducts (LHD; arrowhead) are nearly completely separated by deeply infiltrating lesion in hepatic hilum. Right anterior ducts (RAD) are not visible. B. RAD (black arrow) was visualized by percutaneous cholangiography. RAD are in hepatic dome and acutely angled to be accessed percutaneously, thus left access was made and followed by crossing of guide wire (arrowheads) from RPD to LHD. C. Crisscross configured stent placement connecting LHD-RAD and RPD-CBD was attempted but pathway connecting LHD-RAD could not be found. Thus 1st stent was placed from RPD to LHD (white arrowheads). 2nd stent was placed from RPD to CBD through 1st stent (white arrows). Then we found way (black arrow) to connect LHD and RAD through stent. D. 3rd stent was placed from LHD through stents to RAD. Because RPD anomalously joined CBD, 4th stent was placed from RPD through stent to CBD. Nearly complete internal drainage was obtained with 4 open cell stents.
|
Dilatation of the stricture before stent insertion (pre-dilatation) was done with a 4 mm or 8 mm balloon catheter (Rider; Leventon, Barcelona, Spain) to facilitate insertion of the stent delivery system. Balloon dilatations were performed after stent insertion (post-dilatation) in patients who had a tight strictures. A 4 mm balloon (5 F shaft diameter via 5 F introducer system) was used prior to advancing the 8 mm balloon (5 F shaft diameter via 6 F introducer system) when the 8 mm balloon could not be advanced across the lesion. If expansion of the stents was less than 80%, the stents were dilated (post-dilatation) with the 8-mm balloon catheter. After stent placement, 10 F external drainage catheters (A & A, Seongnam, Korea) were inserted through the PTBD tracts. An early follow-up cholangiographic study to confirm the position and patency of the stents was done 3 days after stent placement. After confirmation of good stent patency, the external drainage catheters were removed after at least 3 weeks later for tract maturation.
No patient had chemotherapy after stent placement. Intraluminal brachytherapy (ILBT) was performed in 3 of 26 patients (11.5%). Patients who received ILBT were selected on a clinical basis. Of the patients scheduled to undergo ILBT, we replaced one of the external drainage catheters with a 12 F catheter with no side hole (A & A) through the stents after the 3-day follow-up. ILBT was performed in the radiation oncology department with the use of an iridium wire (15-30 Gy) inserted through the catheter. The catheter was capped when it was not used for ILBT.
Definitions
Technical success was defined as successful placement of every stent resulting in successful decompression of bile ducts. The expansion degree of the second stents were estimated using fluoroscopic images during the early follow-up study.
All the procedural complications were divided into major and minor categories in accordance with the reporting standards of the Society of Interventional Radiology (14). Clinical success was defined as adequate palliation of the obstructive jaundice without recurrent cholangitis. Palliation of the jaundice was considered adequate when the serum bilirubin level was maintained or decreased in relation to the catheter drainage during the 1-month period following removal of the external drainage catheter.
The study endpoints were checked with clinical findings and laboratory tests including serum bilirubin levels at 1, 3, 6 and 12 months after stent placement during the follow-up period. In cases of recurrent jaundice, patients were evaluated by US, PTC, or CT. A stent was considered to be occluded if the patient had a hyperbilirubinemia (> 3 mg/dL) with increased bile duct dilatation on the imaging study. When stent occlusion occurred, an attempt at correction was made by inserting an external drainage catheter or an additional stent.
Statistical Analysis
The primary stent patency period was calculated as the interval between stent placement and its obstruction. The patient survival period was calculated as the interval between stent placement and the patient's death. For the analysis of stent patency and patient survival, patients who were followed for at least 25 days after stent placement were included. If no exam data of stent occlusion during the follow-up was found, the patients were censored at the time of analysis. Cumulative stent patency and patient survival were estimated by the Kaplan-Meier method and supplemented by the log-rank test for the assessment of difference affected by age, sex, cause of obstruction, Bismuth type and ILBT A p value of < 0.05 was considered statistically significant. All analyses were performed with statistical software (SPSS version 18.0; SPSS, Chicago, IL, USA).
Go to :
RESULTS
Technical Results
Stent placement was performed through the right access (n = 17), the left access (n = 3), or the bilateral accesses (n = 7). Stent placement was attempted through one access in 9 (6 right, 3 left), two accesses in 12 (7 bilateral, 5 right unilateral), or three accesses in 5 (4 bilateral, 1 right unilateral). Technical results including the number of stents used according to stent configurations are summarized in Table 1.

Stent placement was primarily successful in 24 of 26 patients. Two primary technical failures were the crushing of the left limb of the first stent by the second stent delivery during T-configured stent placements through a left access (Fig. 3). Stent placements due to technical failure were corrected secondarily by adding a stent through a new right access to overcome the left limb crushing. Follow-up cholangiographies revealed successful drainage of both hepatic lobes in all 26 patients. Expansion degrees of the intersecting stent were > 80% in all patients. Thus the primary technical success rate and the secondary technical success rate were 93% and 100% respectively.
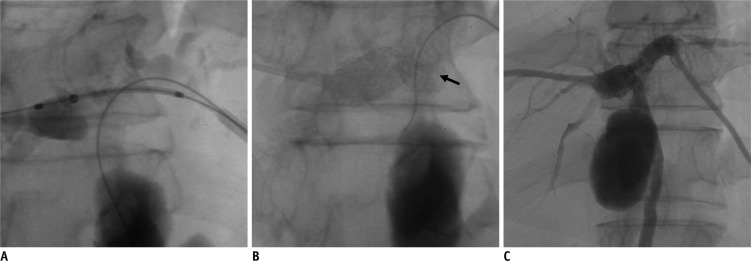 | Fig. 3Stent crushing during T-configured stent placement in patient with cholangiocarcinoma.
A. T-configured stent placement was attempted via left. B. Crushing of left limb of first transverse stent (arrow) occurred during insertion of second stent. C. Stent placement was secondarily completed after insertion of additional transverse stent through new right access. Follow-up cholangiographies revealed successful drainage of both hepatic lobes.
|
Clinical Results
Patients were recommended to visit the hospital 1, 3, 6 and 12 months after stent placement for follow-up clinical findings and laboratory tests. A total of 24 patients were followed for 25-354 days (mean 141.5 days). Two patients were Two patients were lost during the follow-up due to being discharged in one week discharge within one week. Clinical success was achieved in 21 of 24 patients (88%); serum total bilirubin levels (STBL) were less than 2 mg/dL in 19 patients and between 2 and 3 mg/dL in 2 patients. The mean STBL of clinically successful patients was 8.2 ± 2.3 mg/dL before stent insertion and 1.8 ± 0.9 mg/dL after stent placement. Stent placement was clinically unsuccessful in 3 patients; 1 patient, showed acute elevation of serum total bilirubin level after catheter removal from the early occlusion. Two other patients showed gradual aggravation of jaundice without evidence of stent occlusion. No early mortality (within 1 month) was observed.
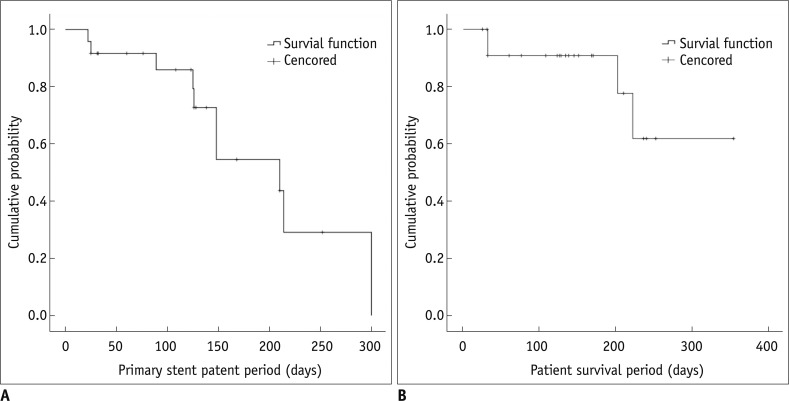
Eight patients died without the confirming stent occlusion. Stent occlusion during the survival period occurred in eight patients (33%) by tumor in-growth or over growth (4 patients with T-configuration, 3 patients with crisscross-configuration, and 1 patient with Y-configuration). The mean primary stent patency period was 191.8 days (95% CI, 144.2-239.5 days). The mean patient survival period was 299 days (95% CI, 205.6-392.4 days) (Fig. 4). Statistically significant differences were not observed in the stent patency or survival rates in relation to age, sex, cause of obstruction, Bismuth type or ILBT.
No deaths occurred as a result of the stent insertion procedures. However, a major complication occurred in 2 of 26 (7.7%) patients. A hemorrhage from the segment III branch of the hepatic artery occurred post-dilatation of the first stent, via left access, in one patient. A Y-configuration stent placement by right and left access was attempted in this patient. Bleeding was treated successfully by embolization of the segmental artery. In another patient, sepsis occurred immediately after the procedure, and was treated by intravenous antibiotics. No minor complications occurred in any patients. Repeated interventions were performed in 10 patients. Bilobar drainage with one PTBD catheter was possible in 8 patients with T-configured stent placements. Bilobar drainage with two PTBD catheters was performed in 2 patients with Y-configuration stent placements. Additional stent placements were performed in 4 patients that provided successful drainage of both hepatic lobes on follow-up cholangiographies.
Go to :
DISCUSSION
Bilobar drainage for malignant biliary obstruction via percutaneous or endoscopy guided T- or Y-configured stent placements using stent-in-stent techniques have gained widespread acceptance in recent studies (2-4). In patients with a separation of the sectoral duct by hilar malignancy or congenital variation, crisscross configured stent placement or multiple intersecting stent placement over two stents could be considered an alternative method to achieve sufficient drainage from each sectoral or segmental duct (18).
In general, self-expanding metallic stents can be divided into two types, closed cell stents and open cell stents. For now, most information and data are available on the closed cell stents for the biliary system. Due to its relatively smaller cell size, there is a technical difficulty in insertion of the first stent through the second stent when using closed cell stents for bilobar biliary drainage. To overcome this, a "side by side" method or a "stent-in-stent" method using newly designed stents with a wide central mesh is suggested (19, 20). However, there is a decline in stent radial force in the newly designed closed cell stents as the central segment consists of wide open mesh with omitted struts.
In contrast, when two open cell stents are overlapped, a minimal number of connecting bars which link z-components of the stents tend to break. Such interaction facilitates enough space for full expansion of the second stent as well as minimizes decline in the radial force of the stent. Müller-Hülsbeck et al. (21) reported that an open cell nitinol stent has more flexibility and adaptability compared to a closed cell design. Due to these physical properties, open cell stents appeared more suitable for bifurcating lesions or tortuous anatomy and have been widely used, especially in vascular system (16). Expansion of the second stent at the intersection was good (> 80% in diameter) in all cases in our study. We thought that this property could be useful when adding a stent to a previous closed cell stent. In this study, one patient in whom the volume of the drained left lobe was sufficient, underwent endoscopic left unilobar drainage with a closed cell stent. After one week, symptoms and laboratory findings of cholangitis due to the right undrained duct were aggravated and immediate right external drainage (PTBD) was performed. Two open cell stents were added via additional right PTBD sites with a 'stent-in-stent' method, and revealed good expansion and good contrast flow on follow-up cholangiographies.
Open cell nitinol stents have good pushability and trackability owing to their more rigid and low profile delivery system compared to the knitting type of the closed cell nitinol stent. Its rigid and low profile system enable an open cell stent to pass through a tight stricture or complexly overlapped stents, and it is effective in trying to connect the segmental biliary duct through a tortuous tract.
However, there are several factors that should be considered when applying an open cell stent in the biliary system. First, in a percutaneous biliary stent insertion, a stent passes through the tortuous and angulated tract in many cases, and the jagged edge of an open cell can act as an interruption. In the acute angle of tract access, the second stent insertion is disturbed by the intersection with struts from the first stent. Crushing of the 1st stent at the intersection during the 2nd stent insertion occurred in 2 patients (66%) that had T-configured stent placement via the left hepatic access (Fig. 2). Second, the surface of an open cell stent was uneven and had sharp struts, which were more prominent when the stent curved in an angled tract. In the angled tract, triangular shaped Z-components of open cell stents dig into the surroundings. Open cell stents can cause hepatic artery and portal vein injury because they travel around the bile duct in the liver. In this study, bleeding from the S3 segmental hepatic artery occurred in 1 patient after post-dilatation of the stent, and transcatheter arterial embolization was required.
The stent patency period of bilobar open cell stent placement in the biliary system appears to not be as inferior to the prior studies, which used closed cell stents (3, 15, 19). In a previous report of a T-configured biliary hilar stent placement (3), the mean stent patency time was 170.3 days (range, 7-305 days). The study included small numbers of Bismuth IV lesions (seven of 57 patients; 8.8%) and gallbladder cancer (seven of 57 patients; 8.8%). In a report of crisscross configured stent placement (18), which obtain nearly complete drainage, the median primary stent patency time was 187 days (95% CI, 136.2-237.9 days). The study included 50% of Bismuth IV lesions (21 of 42 patients) and 31% of gallbladder cancer (13 of 42 patients). Our study included 54% of Bismuth IV lesions (14 of 26 patients) and 16.7% of gallbladder cancer (4 of 24 patients). Although there is some lack of reliability in stent patency because of the small number of cases and censored data (18 of 26: 69.2%) in our study, we postulate that two factors, nearly complete drainage with multiple stents and good expansion with adequate radial force, could contribute to a longer stent patency period.
We thought that sharp jagged strut of the open cell stent could interrupt passing of a catheter through the intersecting segment to the contralateral lobar duct. However, the passing of drainage catheters or additional stent deliveries were successful without technical difficulty during the re-intervention procedure. Additionally newly placed stents, following the occluded prior stents were also well expanded in the intersection.
In conclusion, applying open cell stents in the biliary system is feasible, and can be effective especially in multiple intersecting stent insertions in the hilum, and additional stent insertion through previously inserted stents. However, it is unfavorable in accesses with acute angles and the possibility of surrounding vessel injury should be considered.
Go to :
 XML Download
XML Download