

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As the use of CT for diagnosis and intervention increases, radiologists, physicists, and CT scanner manufacturers are required to reduce the radiation exposure from CT (1-8). Radiation dose is directly proportional to the tube current at a fixed peak tube voltage, scanning time, and slice width. However, the image noise is inversely proportional to the square root of the mAs using filtered back projection (FBP) method, which is the currently used CT image reconstruction technique. Thus, increase in the image noise is inevitable when we use lower tube current mode (9). Although several studies have evaluated the use of low- to ultra-low-dose chest CT (10-14), using a lower milliampere-second setting has some potential disadvantages, including high rates of artifacts and false-negative results (12, 14).
Image reconstruction in image space (IRIS) is a new CT reconstruction technique using an iterative reconstruction technique and was recently introduced to CTs. In our previous study, we evaluated whether the IRIS technique improves the image quality (IQ) at a standard dose CT (SDCT) and low dose CT (LDCT), and whether the IRIS can reduce the radiation dose by half. Our results indicated that IRIS generally improves the image quality of a chest CT, but that, even with IRIS, decreased radiation dose by half results in a decrease of the IQ. In that study, we assessed the subjective IQ scores for each image and compared the IQ scores. For clinical application, however, it may be more important to determine the preference of expert radiologists directly from a side-by-side comparison. We, therefore, assessed the effect of the radiation dose and reconstruction algorithms on the radiologists' preferences.
MATERIALS AND METHODS
Patients
This prospective study was approved by our institutional review board. Informed consent was obtained from all participating patients.
From March to April 2010, 50 patients (30 men, 20 women; mean age, 56.4 ± 14.9 years; range, 18-79 years, mean BMI, 23.0 ± 3.0 kg/m2) underwent SDCT and another 50 patients (31 men, 19 women; mean age, 57.2 ± 11.9 years; range, 27-76 years, BMI, 24.0 ± 3.0 kg/m2) underwent LDCT. All patients were evaluated for the check-up or for known abnormalities.
CT Examination and Reconstruction
Detailed CT protocols have been described in our previous report (15). Both full-radiation dose data and half-radiation dose data, from one SDCT scan, were reconstructed using the standard FBP algorithm and the IRIS algorithm. Therefore, 4 CT image sets from one SDCT scan were obtained: 1) FBP images at full radiation dose (F-FBP), 2) IRIS images at full radiation dose (F-IRIS), 3) FBP images at half radiation dose (H-FBP), and 4) IRIS images at half radiation dose (H-IRIS). Finally, a total of 200 CT image sets from 50 SDCT scans, were prepared for review. In FBP images, the CT images were reconstructed in 5 mm thickness at 5 mm intervals with the B30f kernel for evaluation of mediastinal structures, and the CT images were reconstructed at 5 mm thickness at 5-mm intervals, and 1 mm thickness at 1 mm intervals with B70f kernel for the evaluation of the lung parenchyma. For IRIS, we used the I30f (5 mm thickness at 5 mm intervals) for the mediastinum and the I70f (5 mm thickness at 5 mm intervals and 1 mm thickness at 1 mm intervals, respectively) for the lung parenchyma. We also performed the image reconstruction in the same way for LDCT images, and we prepared 200 CT image sets of LDCT for review. Consecutive CT examinations were dicomized and sent to picture archiving and communication system (Petavision; Asan Medical Center, Seoul, Korea). For the evaluations of the mediastinum, the CT images with 5 mm slice thickness and B30f kernel or I30f were the preset at the window level of 35 H and window width of 350 H. For the evaluations of lung parenchyma, the appropriate CT images were preset at the lung window setting (window level of -700 H and a window width of 1500 H). The radiologists were asked not to change the preset window levels and widths, during the evaluation of IQ.
Radiologists' Preference and Data Analysis
To evaluate the effect of radiation dose on the radiologists' preference and for internal validation of these preferences, 10 F-IRIS/H-IRIS image pairs from both SDCT and LDCT were prepared. The effect of the reconstruction algorithm on the radiologists' preferences was assessed, using 40 F-IRIS/F-FBP pairs and 10 H-IRIS/H-FBP pairs from both SDCT and LDCT, and the mixed effects of radiation dose and reconstruction algorithm on radiologists' preferences were determined, using 40 F-FBP/H-IRIS pairs from both SDCT and LDCT. The 100 pairs of CT images retrospectively from both SDCT and LDCT were randomized and evaluated independently by two chest radiologists (reader 1 with 16 years of experience and reader 2 with 20 years of experience in thoracic imaging), who were blinded to the reconstruction methods and radiation doses. The radiologists, independently determined their preferences for the clinical usage with a 5-point-scale system (A/B, 1, strongly preferred A; 2, somewhat preferred A; 3, no preference; 4, somewhat preferred B; 5, strongly preferred B), based on the image noise, contrast, and anatomic region definition of mediastinal and lung structures. Preferences for mediastinal images were assessed on B30f and I30f/5 mm slice thickness images, and for lung parenchyma on B70f and I70f/5 mm and 1 mm slice thickness images. The two radiologists were asked to consider the same categories in determining the image preference, as those of our previous study (Table 1) (15). Wilcoxon's signed rank tests were used to evaluate the statistical significance of radiologists' preferences on F-IRIS/F-FBP and F-FBP/H-IRIS pairs, with p values < 0.05 considered as statistically significant.
RESULTS
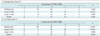
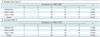
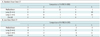
When we compared the H-IRIS images and F-FBP images for the evaluation of the combined effects of radiation dose and reconstruction algorithm, we found that both radiologists preferred the IRIS images, even though the radiation dose was reduced by half, over the FBP images with full radiation dose for the evaluation of the lung parenchyma and overall IQ in both SDCT and LDCT (p < 0.05 each, except for overall IQ in SDCT) (Table 2) (Figs. 1-3). The evaluation of the effects of the reconstruction method, by comparisons of F-FBP and F-IRIS pairs and of H-FBP and H-IRIS pairs, showed that the IRIS images were preferred for the evaluation of the lung and the overall IQ (p < 0.001 in full dose images; Tables 3, 4). In contrast, both radiologists preferred the FBP over the IRIS images for evaluation of the mediastinum in both SDCT (p = 0.035) and LDCT (p < 0 .001) (Tables 2, 3) (Fig. 4). Both radiologists preferred CT images at higher radiation dose in all the assessed categories (Table 5). Figures 1, 2 and 3 illustrate the lung parenchyma in F-FBP, F-IRIS and H-IRIS images of the SDCT and LDCT. Figure 4 shows the mediastinal images in F-FBP, F-IRIS and H-IRIS of the SDCT.
DISCUSSION
We have evaluated the radiologists' preferences for CT images, reconstructed with the FBP and IRIS algorithms for the clinical usage. In our previous study, we evaluated the subjective IQ scores on each assessment contents, such as noise, sharpness, and contrast on FBP and IRIS images, but we did not evaluate the radiologists' overall preferences for clinical practice. The IRIS method uses a non-linear image processing algorithm, called "regularization", not just simple noise reduction, which makes the image characteristics of IRIS unique and different from those of the FBP images. Therefore, even if the individual IQ scores of the assessed contents could be high in the IRIS images, radiologists' preferences for clinical usage may be influenced by imaging characteristics and overall image quality, making it important to determine experts' overall opinions about which the image is favored for the clinical practice by comparing the images, side-by-side.
We found that both expert radiologists preferred the IRIS images even with the reduced radiation dose by half over the FBP image with full radiation dose for the evaluation of the lung parenchyma in both SDCT and LDCT. Our explanation is that the improved back ground noise reduction of the lung parenchyma and concurrently preserved the sharpness of the vessel and bronchial in the regularization step of the IRIS images may affect the preference of the radiologists. However, although we used the same imaging data, as in our previous study (15), in which we investigated whether the IRIS technique can reduce the radiation dose by half, using the radiologists' subjective IQ scoring system, the results of these two studies differed from each other. In the previous study, the reduced radiation dose resulted in reduced IQ, even with the IRIS technique, and the subjective IQ scores were significantly higher in the F-FBP than in the H-IRIS images. This discrepancy is difficult to explain, although, the distribution of the image noise may have had a greater effect on radiologists' preferences than other image characteristics for the overall IQ. In our previous study, the measured image noise of the H-IRIS image was significantly lower than that of the F-FBP images. Alternatively, the discrepancy may be due to the use of different readers in these two studies. Radiologists may have different preferences for the IQ and image characteristics, and then the standards for the evaluation of IQ may be subjective and different from each other.
With the same radiation dose setting, both radiologists preferred IRIS over FBP images for the evaluation of the lung parenchyma in both SDCT and LDCT (Tables 3, 4) (Figs. 1-3). In contrast, the readers generally preferred FBP over IRIS images for evaluation of the mediastinum (Tables 2, 3) (Fig. 4). These results are similar to those of our previous study. In the previous study, the subjective IQ in the lung image was generally improved with the IRIS technique, comparing with that of the FBP images with the same radiation dose, and this improvement was more distinct in the images with the reduced radiation dose, whereas the subjective IQ scores for the evaluation of the mediastinum were higher in FBP than in the IRIS images at the same radiation dose. The lower preference for IRIS in the evaluation of the mediastinum seems to be due to an excessive reduction of the image noise in the "regularization" step of the I30f kernel, with this excessive smoothing effect of the IRIS technique, which affected the subjective IQ.
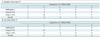
For internal validation of the radiologists' preferences, we also included H-IRIS/F-IRIS sets. In most data pairs, the two radiologists consistently preferred the higher radiation dose images in both SDCT and LDCT, and this means that the readers reached consistent results in this study (Table 5).
We found that the IRIS technique was effective in reducing the radiation dose in a CT, especially in the lung parenchyma images, and that the two radiologists preferred IRIS images at 50% reduced radiation dose to FBP images, with higher radiation dose. In the recent studies by Pontana et al. (16) and Prakash et al. (17), they also reported the radiation dose reductions in a chest CT by 35% by using an IRIS technique and by 26% to 29% with the adaptive statistical iterative reconstruction technique (different iterative reconstruction technique), retrospectively, without compromising the IQ. In their study, they used a follow up CT scan in same patients or a weight matched CT scan from different patients for the CT images with reduced radiation dose to compare with the initial full dose CT scan with FBP technique. However, at these settings, the differences in the scanning levels, respiration status and lung abnormalities can influence the measurement of image noise and subjective IQ. Moreover, differences in the sizes of thoracic cages and other structures in different patients may affect the subjective IQ, including the image noise. In contrast, we could compare the full dose and reduced dose CT images from CT scans of same patients. These images were obtained at the same time, without additional CT scanning, using the modified dual energy CT scan mode in the dual source CT. This made possible for the evaluation of the image noise and other IQs at the same scanned level and in the same patient without the interference from different CT scan levels or different disease conditions. The importance of this intrapatient comparison, without additional CT scanning, is also described in recent studies (17).
Although the radiologists preferred the IRIS images, even at the reduced radiation dose in our study, it is difficult to investigate how much the radiation can be reduced. Because, the quantitative comparisons of IQ are difficult, due to the non-linear image processing algorithm used to reduce the image noise in the IRIS technique, making the appropriate CT imaging characteristics and quality for various different diseases. Together with the results of subjective IQs and reader's preference, we think that it may be possible to reduce the radiation dose by 30 to 40%, which is well agreed with the results of the previous studies (16, 17). Further, according to our preference study, for the evaluation of lung parenchyma, such as lung cancer screening CT or nodule follow up CT, IRIS image with 50% reduced radiation dose can be feasible.
This study had several limitations. Firstly, the complete blinding of the radiologists was impossible. Although the radiologists were blinded to the reconstruction method, the characteristics of the IRIS and FBP images were different and the IRIS image was somewhat unique. However, the readers were also blinded to the radiation dose, and we used the various combinations of the each 10/10/40/40 image pairs to weaken this limitation. Secondly, we only evaluated the radiologists' preferences for CT images in clinical practice, but we did not evaluate the diagnostic acceptability and lesion conspicuity of the IRIS images. We could demonstrate the improvement or preservation of the general IQ in the IRIS image with the reduced radiation dose does for the lung image, but the influence of the characteristics of the IRIS image on the specific disease pattern is not known. The effect of the IRIS technique on diagnostic performance in patients with abnormal lesions remains to be investigated. Thirdly, BMI of our patient is relatively low due to the characteristics of being Asian; thus, it is uncertain if our results can be generalized for more adipose patients. Finally, we used a DSCT scanner with a modified dual energy mode to evaluate the half dose CT images, without the additional CT scanning. However, the two X-ray tubes and two detector arrays give rise to a cross scattering radiation (7), or the scattering of X-ray photons from one source to the detector array of the other source. Accordingly, cross scattering radiation may have affected the IQ. However, this effect may be negligible because the DSCT scanner we used employs scatter correction algorithms to minimize any cross scattering effect.
In conclusion, radiologists' preferences for chest CT are influenced by the radiation dose and reconstruction algorithm. According to our preliminary results, dose reduction at 50% with IRIS may be feasible for the lung parenchymal evaluation.





 XML Download
XML Download