

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endobronchial fibroepithelial polyps are a rare neoplasm with only a few case reports in the English literature (1-4). Histologically, these lesions are composed of collagen fibers in a stroma covered by normal respiratory epithelium (3). We report a case of a fibroepithelial polyp of the bronchus, of which a lobulating contour is well visualized at computed tomography (CT).
CASE REPORT
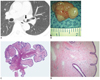
A 47-year-old man presented with mild dyspnea and sputum. A physical examination was unremarkable. On a posteroanterior chest radiograph, no abnormal findings were seen in both lungs. However, a non-contrast chest CT scan (Brilliance 6, Philips Healthcare, Cleveland, OH, USA) revealed a 1 cm, endobronchial polypoid nodule abutting the anterior wall of the left main bronchus, which had a soft-tissue attenuation of 40 HU. The endobronchial nodule showed a conspicuous lobulating contour that resembled an appearance of a blackberry (Fig. 1A).
At bronchoscopic examination, a lobulated endoluminal nodule with a glossy surface was arising from the anterior wall of the left main bronchus, resulting in significant luminal narrowing. The polypoid nodule was removed using an electrosurgical snare during rigid bronchoscopy under general anesthesia.
At gross examination of the polypectomy specimen, the tumor measured 1.2 × 1.0 cm in diameter with a lobulating contour and a glossy surface (Fig. 1B). Histopathologically, the nodule showed marked papillary projections, which resulted in the gross morphology of a lobulating contour of the polyp (Fig. 1C). It consisted of fibrovascular stroma covered by normal respiratory epithelium, enabling the histological diagnosis of a fibroepithelial polyp (Fig. 1D).
DISCUSSION
A fibroepithelial polyp is a common type of tumor in the skin or the genitourinary tract. Especially, it is the most common benign tumors of the ureters (5-8). However, fibroepithelial polyps of the bronchus are rare with only a few case reports in the English literature (1-4). According to these case reports, it manifests as an endobronchial polypoid nodule that is covered with normal respiratory mucosa, consisting of fibrovascular stroma with or without few inflammatory cells and adipocytic components (1-4).
The etiology of fibroepithelial polyps of the bronchus is unclear. In general, benign endobronchial polyps can be classified as inflammatory or noninflammatory. However, the exact classification of fibroepithelial polyps still remains indeterminate. Some reports have classified fibroepithelial polyps as inflammatory, while others have argued that the inflammation is a result of the intermittent respiratory tract obstruction caused by its mass effect (4).
Histologically, fibroepithelial polyps of ureters are known to be predominantly composed of urothelial epithelium and fibrovascular stroma, showing a finger-like or polypoid growth pattern (8). Such a papillary growth pattern on histology may result in a lobulating contour of the nodule on gross morphology, which can be readily identifiable on radiological images. The gross appearances of fibroepithelial polyps arising in the tracheobronchial tree and the ureter described in the previous case reports are summarized in Table 1. The majority of appearances of the polyps suggested their lobulating contours, and many of those figures actually shown in reports revealed quite a similar appearance of the nodules to that of our case. Although these appearances had not been emphasized in those reports, the lobulating contour of the polyp was clearly identified on CT images in our case, and this feature had been derived from a typical papillary growth pattern of the fibroepithelial polyp. It has been known that an endobronchial nodule can develop in a variety of neoplasms including squamous cell carcinoma, adenoid cystic carcinoma, mucoepidermoid carcinoma, neurogenic tumor, leiomyoma, hamartoma and lipoma, and so on. These tumors, however, are not known to show a specifically lobulating contour. Therefore, we think that an awareness of the implication of such a lobulating contour of an endobronchial tumor might be important in the differential diagnoses of various tracheobronchial polypoid nodules.
In summary, we report a case of a fibroepithelial polyp of the bronchus in which a lobulating contour of the endophytic nodule was well identified at CT scan, and we believe that its lobulating shape represents a typical papillary growth pattern of the tumor on histopathology. Although endobronchial fibroepithelial polyps are a rare neoplasm, such a characteristic lobulating contour of the polyps might be helpful in the differential diagnosis from other various endobronchial polypoid nodules.

 XML Download
XML Download