

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radiofrequency ablation (RFA) is generally accepted as one of the most promising therapies for treating non-resectable hepatic tumors (1-3). RFA has recently been recognized as a potential alternative to surgery for small HCCs (3-8). However, compared with surgical treatment, a relatively high local tumor progression rate is regarded as a considerable shortcoming of RFA treatment (4, 8, 9). It has already been well-demonstrated in the literature that local tumor progression rates increase with larger-sized tumors (10, 11).
The most significant factor contributing to high local tumor progression rates when using conventional RFA systems with a single electrode is their inability to ablate a sufficient volume in the ablation zone to achieve complete tumor destruction (11-13). Until now, although several types of electrodes (14), including the internally cooled needle (15-17), perfused needle (18), and expandable needle (19, 20), have been developed to achieve a greater ablation volume with a single application of RF energy, there are definite limitations to the ablation volume that can be destroyed using a single electrode. Therefore, consecutive overlapping ablations are required when using a single electrode RF system in order to create an ablation area sufficient to cover the tumor as well as the peripheral safety margins (13, 21-24). However, this is both time consuming and technically challenging as the gas bubbles formed disturb the repositioning of the electrode under ultrasound guidance, thereby leading to incomplete ablation (13, 25).
To increase the volume of coagulation with a single application, multiple electrode approaches have been designated using various modes including simultaneous monopolar (16, 26), switching monopolar (27-30), as well as bipolar and multipolar modes (31, 32). It has been proven that RFA using multiple electrodes creates a larger ablation volume than conventional single-electrode RFA (16, 26-34). Several preclinical in vivo experiments have shown that switching monopolar RFA can create a larger ablation volume than consecutive overlapping RFA (30, 35, 36); however, there have been only two retrospective studies reporting the early clinical experience of switching monopolar RFA for malignant liver tumors (37, 38). In one retrospective study, as the therapeutic results of switching monopolar RFA for treating malignant liver tumors, including HCCs as well as metastases, were described without distinguishing each type of tumor, the clinical efficacy of switching monopolar RFA for HCC has not yet been determined. Furthermore, neither of these studies evaluated the therapeutic efficacy of switching monopolar RFA, depending on tumor size. Therefore, the purpose of this prospective study is to assess the safety and short-term therapeutic efficacy of switching monopolar RFA for treating medium-sized (3.1-5.0 cm in diameter) HCCs.
Go to : 
MATERIALS AND METHODS
Clinical Features of the Study Patients
Thirty patients with medium-sized HCCs (3.1-5.0 cm in diameter) were enrolled in this prospective study designed to evaluate the therapeutic efficacy of switching monopolar RFA at Seoul National University Hospital, from July 2007 to January 2009. The inclusion criteria were as follows: 1) patients with a single HCC measuring 3.1-5 cm in diameter; 2) no evidence of vascular invasion or extrahepatic metastasis; 3) no history of previous treatment for HCC; 3) liver function classified as Child-Pugh class A or B; 4) platelet count greater than 50,000/µL; 5) an international normalized ratio for prothrombin time greater than 1.7; and 6) follow up for six months or more. This prospective study was approved by our hospital's Institutional Review Board, and written informed consent was obtained from each patient.
The clinical diagnosis of HCC in 29 study patients was made on the basis of the radiologic features of the tumors, which consist of a combination of typical arterial enhancement with washout on portal venous phase or equilibrium phase images on dynamic contrast-enhanced CT scans and/or dynamic MR images, and α-fetoprotein (AFP) values according to the clinical guidelines proposed by the American Association for the Study of Liver Diseases (39). In the remaining patients, the diagnosis of HCC was confirmed by percutaneous needle biopsy. Table 1 summarizes the demographic, clinical, and laboratory findings of the study patients, while Table 2 summarizes the radiologic tumor findings.
Switching Monopolar Radiofrequency Ablation
All RFA procedures were performed percutaneously under ultrasonographic guidance using a multi-channel RFA system (Taewoong Medical, Goyang, Kyunggi, Korea) with multiple electrodes by one of three attending radiologists with at least five years of clinical experience in performing RFAs (range, 5-14 years). A combination of fentanyl citrate (Hana Pharm, Seoul, Korea), Midazolam (Hana Pharm, Seoul, Korea), and Ketamine (Huons, Hwaseong, Kyunggi, Korea) was administered intravenously in order to induce conscious sedation. Vital signs and cardiac status were monitored by pulse oxymetry and electrocardiography during the procedure.
The multi-channel generators produced a maximum power of 200 W at a frequency of 480-kHz, using the switching monopolar mode to heat tissue, and the application of power in an alternating fashion to two or three probes in order to avoid interference from multiple RF probes (Faraday cage Effect) (36). The switching system is based on the following protocol (36): the maximum power will switch electrodes after approximately 30 seconds if there is no impedance increase of at least 50 ohms above the baseline value. However, if there is an impedance value in one of the electrodes that exceeds 50 ohms above the baseline value, the current will automatically switch to the other electrode. In addition, if the impedance increases to 300 ohms above the baseline value, no power will be applied to that particular electrode for 15 seconds.
We used two (n = 5) or three (n = 25) electrodes depending on the location and size of the target tumors; i.e., single, internally cooled electrodes (Well-point electrode™: Taewoong) were used in 19 patients, a combination of single and clustered electrodes were used in eight patients, and cluster electrodes were used in the remaining three patients. In general, three single electrodes (3 or 4 cm active tip) were preferentially used for HCCs measuring 3.1-3.5 cm in diameter, along with a combination of single and cluster electrodes (2.5 cm active tip) or three cluster electrodes for HCCs larger than 3.5 cm in diameter. The electrodes had 17-gauge diameters and measured 15 cm in length. A chilled normal saline solution was infused into the lumens of the electrodes to maintain a tip temperature of 20-25℃. The electrodes were placed in the target tumors under ultrasonographic guidance, at an interprobe spacing of 1-2 cm, using an epigastric, subcostal or intercostal approach. Interelectrode spacing was generally kept to 2 cm or less in order to prevent coagulation zones from becoming cleft or irregular (36, 37). When electrodes were placed in the target tumors, they were inserted through separate puncture sites and were initially activated for 18 minutes (36). If subsequent ablations of the same tumor were required, they were performed for 8-18 minutes depending on both the tissue impedance and temperature. When ideal electrode placement was unsuccessful and failed to create an adequate ablation volume, the electrodes were repositioned. Repositioning of the applicators was required in 13 of the 30 study patients (43%).
To prevent track seeding after delivering RF energy, track ablation was performed while withdrawing the electrodes; the tip temperature of 90℃ was attained by discontinuing cooling of the electrodes and maintained during retraction of the electrodes. In patients with peripheral tumors in the vicinity of the body wall, diaphragm or bowel artificial ascites were established using a 5% dextrose in water solution (D5W) in order to isolate the liver. Instillation of D5W was performed in 12 of the 30 study patients (33%).
Post-Treatment Assessment and Follow Up
Contrast-enhanced CT was performed immediately following the RFA procedure in order to assess both therapeutic responses and possible complications. Multiphasic liver CT scans composed of precontrast, arterial, and portal venous phase images, were routinely used. In total, 370 mgI/mL of iodinated contrast medium (iopromide, Ultravist 370; Schering, Berlin, Germany) at a dose of 1.5 cc/kg body weight, was injected for 30 seconds using a power injector (Stellant Dual; Medrad, Indianola, PA), followed by 40 mL of normal saline chaser. The timing for the arterial phase scan was determined using a care bolus technique (Sensation 16; Siemens, Erlangen, Germany): the arterial phase scanning was automatically started 17 seconds after the attenuation coefficient of the abdominal aortic blood reached 100 Hounsfield units. The portal venous phase scans were acquired 70 seconds after starting the contrast injection.
Ablation was considered to be sufficient when the unenhanced ablation zone was larger than the treated tumor, while there was a tumor-free margin of at least 5 mm (40). If ablation was not sufficient on the CT immediately following the RFA procedure, additional ablations were performed. The assessment and treatment procedures were repeated until sufficient ablation was achieved during one hospital stay. In two of the 30 study patients (7%), an additional RFA was performed under ultrasonographic guidance. When sufficient ablation was confirmed, the ablation volume was carefully examined in the final images. Follow-up consisted of performing contrast-enhanced CT examinations at both the first and third months following ablation as well as subsequent contrast-enhanced CT examinations obtained every three months.
To evaluate the efficacy of the switching RFA for inducing a large ablation volume, the maximum (Dmx) and minimum (Dmi) diameters were measured on a transverse section showing the largest ablation area by immediate follow-up CT. The vertical diameter (Dv), which is the length from the most cranial border to the most caudal border of the ablation zone, was also measured. The surrounding hyperemia area was not included in the ablation zone measurement. The volume of the ablation zone was evaluated by approximating the ablation zone to an ellipsoid using the following formula: π (Dv × Dmx × Dmi)/6 (36).
To evaluate the clinical efficacy of switching RFA for treating HCC, technical effectiveness, local tumor progression, new HCC recurrence, and tumor-free survival time were all determined (40, 41). Technical effectiveness was defined as when marginal nodular enhancements were not seen within the ablation zone on CT scans for at least one month following RFA (41) (Fig. 1). Intrahepatic tumor recurrence was categorized into two groups, which are local tumor progression and new HCC occurrence (41, 42). When a follow-up CT scan showed an enhanced area or enlargements at the margins of the treated tumors in which the technical effectiveness was documented on the one-month follow-up CT scan, it was determined to be local tumor progression (Fig. 2). New HCC occurrence was defined as development of a new HCC nodule away from the previously ablated lesion. Follow-up scans were interpreted by one of three attending physicians who were routinely involved in reading contrast-enhanced abdominal CT scans as well as post-RFA CT scans in the Abdominal Division of Department of Radiology at our institution. Tumor-free survival time was defined as the time between RFA and local tumor progression, and the occurrence of new HCCs, extrahepatic metastasis or final CT examination without overall tumor recurrence.
 | Fig. 171-year-old man with 4.3-cm-diameter hepatocellular carcinoma treated by switching monopolar radiofrequency ablation.
A. Contrast-enhanced T1-weighted image during arterial phase showing hyperenhancing hepatocellular carcinoma in segment VI (arrow). B. Immediate contrast-enhanced CT scan during portal venous phase after radiofrequency ablation procedure demonstrating creation of sufficient ablation zones to cover tumor (arrow). C. 14-month follow-up CT scan during portal phase showing no evidence of local tumor progression in region surrounding radiofrequency ablation zone (arrow).
|
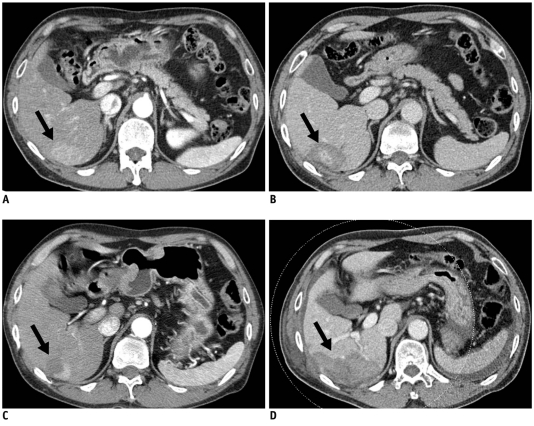 | Fig. 263-year-old man with 4.3-cm-diameter hepatocellular carcinoma treated by switching monopolar radiofrequency ablation.
A. Pre-ablation CT scan during arterial phase showing hyperenhancing 4.3-cm-diameter hepatocellular carcinoma nodule (arrow). B. Immediate post-ablation CT scan during portal phase showing no definite residual enhancing tumor (arrow). C. Arterial phase nine-month follow-up CT scan showing local tumor progression (arrow) on superior side of radiofrequency ablation defect. D. Follow-up CT scan obtained immediately after second radiofrequency ablation using two single electrodes in switching monopolar mode showing complete ablation of recurrent hepatocellular carcinoma (arrow).
|
Complications were classified into major and minor categories according to the Society of Interventional Radiology (SIR) reporting standards for image-guided tumor ablation (41). When complications required treatment, an extended hospital stay resulting from irreversible and adverse sequelae were defined as major complications. All other complications were considered to be minor. Immediate complications were defined as those occurring within 24 hours of the procedure, while periprocedural complications were defined as those occurring within 30 days of the procedure. We did not consider post-ablation pain as a complication.
Statistical Analysis
Descriptive statistics for the following factors were obtained: demographic, clinical, laboratory and imaging findings in patients at the time of RFA; characteristics of the RFA procedures (number of needle insertions, total procedure time, ablation time, and delivered energy); ablation zones (diameter and volume); and complications.
The Kaplan-Meier method was used to estimate the interval between RFA treatment and local tumor progression or tumor-free survival. A p value < 0.05 was considered to indicate statistical significance. All statistical analyses were performed using a statistical software program (SPSS for Windows, version 13.0; SPSS, Chicago, IL).
Go to :
RESULTS
Characteristics of Radiofrequency Ablation Procedures
The mean ablation time was 25.4 ± 8.9 minutes (range, 15-48 minutes), while the mean time occupying an ultrasound suite for the RFA procedure, including conscious sedation, the RFA procedure, post-procedure evaluation, and recovery from the sedation, was 64 ± 19.8 minutes (range, 35-120 minutes). The mean energy delivered was 165.5 ± 66.9 kJ (range, 67.9-323.5 kJ). Table 3 summarizes the treatment characteristics. The mean volume of the ablations zones was 73.8 ± 56.4 cm3 (range, 18.9-229.7 cm3). The maximum, minimum and vertical diameters of the ablation zones on CT scans are summarized in Table 3.

Table 3
Characteristics of Radiofrequency Ablation Procedures and Ablation Zone
Note.- *Data are expressed as mean value ± standard deviation, with ranges in parentheses.
°Data are expressed as frequency.
Total duration of intervention consists of time occupying ultrasound suite for entire radiofrequency ablation procedure; Dmx = maximum diameter on of largest transverse ablation area on portal phase dynamic CT scanning, Dmi = minimum diameter of largest transverse ablation area on portal phase dynamic CT scanning, Dv = length from cranial to caudal border of ablation zone.
![]()
Complications
There were no major, immediate or periprocedural complications. However, during the follow-up period one major complication occurred, which was RFA-related bile duct stricture accompanied by jaundice occurring six months following RFA (Fig. 3). Percutaneous biliary drainage was performed in this patient and eventually biliary stent placement was required. In addition, there were five minor complications: i.e. one immediate complication of mild hemoperitoneum and four minor biliary strictures involving peripheral intrahepatic bile ducts. None of the five minor complications was of clinical significance and therefore required no treatment.
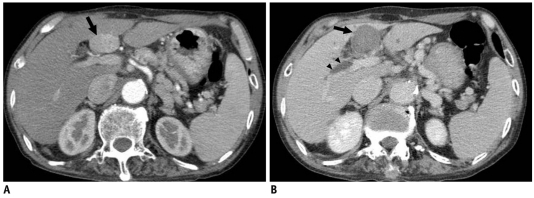 | Fig. 372-year-old man with 3.2-cm-diameter hepatocellular carcinoma treated by switching monopolar radiofrequency ablation.
A. Pre-ablation CT scan during arterial phase showing hyperenhancing 3.2-cm-diameter hepatocellular carcinoma nodule (arrow) in segment VI of liver. B. Six-month follow-up CT scan during portal phase showing mildly dilated intrahepatic ducts (arrowheads) with stricture at hilar level. No evidence of local tumor progression from radiofrequency ablation zone is evident (arrow).
|
Treatment Outcome and Follow Up
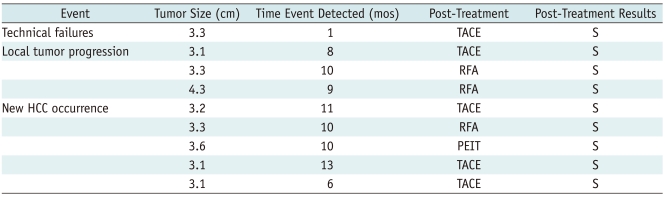
The mean follow-up duration was 12.5 ± 4.7 months (range, 6-22 months). No patient death and no extrahepatic recurrence occurred during the follow-up period. Technical effectiveness was achieved in 29 of 30 patients (97%). Local tumor progression occurred in three of 29 patients in whom technical effectiveness was achieved (10%). The mean local tumor-progression-free survival period was 18.1 ± 1.0 months. New HCCs were detected in five of 29 patients (17%). Both local tumor progression and a new HCC were seen in one patient. In this patient, occurrence of the new HCC nodule as well as the local tumor progression was detected on the 10-month follow-up CT scan, and the nodules were treated simultaneously with the RFA procedure. Overall tumor recurrence, local tumor progression, and/or new HCC occurrence, were detected in eight of 29 patients (28%). The mean tumor-free survival period was 17.5 ± 1.4 months. The cumulative tumor-free survival rates estimated at six months and one year post-RFA were 97 ± 3.4% and 88 ± 6.8%, respectively. Table 4 summarizes our study results with respect to technical failure, local tumor progression, and new HCCs.
Go to :
DISCUSSION
In our prospective study, switching monopolar RFA using multiple electrodes in patients with medium-sized HCCs, showed a high technical effectiveness rate (97%) and a good local tumor control rate (90%, 26 of 29). For achieving complete necrosis with RFA, treatment outcomes in our study using the multichannel RF generator and multiple electrodes, were significantly better than in previous studies in which percutaneous RFA used a conventional overlapping technique with a single electrode (11, 43). In a study using an internally cooled electrode by Livraghi et al. (11) and another study using an expandable electrode by Cabassa et al. (43), complete tumor necrosis was achieved in 61% and 53% of medium size HCCs (3.1-5.0 cm in diameter), respectively. Furthermore, our local tumor recurrence rates achieved by switching monopolar RFA are comparable to those of a previous study with overlapping RFA with cluster electrodes (8-13%) using a percutaneous or surgical approach (44). The improved therapeutic efficiency of switching RFA can be attributed to its ability to produce a greater ablation volume compared with conventional RFA using a single electrode (37, 38).
In addition, our study demonstrated that switching monopolar RFA was more time efficient compared with conventional RFA using a single electrode. In our study, it took 25.4 ± 8.9 minutes to sufficiently ablate tumors, which was a much shorter time than we had previously experienced using a conventional RFA system with a single electrode (four to six, 12-minute, single RF energy applications requiring 48-72 minutes). In our study, the mean ablation time using the switching RF system was also shorter than the times reported in previous studies using single-electrode RF systems (2, 45, 46). A previous study by Laeseke et al. (37) also demonstrated that the total ablation time of multiple-electrode RFA was reduced by approximately 54% compared with an equivalent number of ablations performed using a single-electrode system. Based on our study results, we believe that switching monopolar RFA provides a greater ability at achieving a satisfactory ablation zone for medium-size HCCs during a reasonable procedure time compared with the conventional and consecutive overlapping RF systems using single electrodes. Compared with the previous study (36) in which the switching controller system (Covidien, Boulder, CO) and 200 W generator was used, we used a multichannel RF generator having 3 RF amplifiers whose control is based on independent impedance changes. Although the basic mechanism of the multichannel RF generator for RF energy instillation is very similar to that of the switch controller of the Covidien RF system, it provides a potential advantage of controlling RF energy delivery to each electrode independently, based on impedance changes, and therefore, in a situation when one of the multiple electrodes has a markedly elevated impedance due to charring or placement of tip in a tissue with poor electrical conductivity, the multichannel RF generator may provide better heating efficiency than the switch controller system.
In addition, we believe that the proposed multiple electrode RFA technique could be valuable for treating small tumors (2-3 cm in diameter) with a goal of obtaining similar local recurrence rates comparable to surgical resection (< 5% local recurrence rate), which can be possible only by creating enough safety margin (5-10 mm) around the tumor. Furthermore, it can be used for treating small malignant tumors (< 3 cm) located in the capsular or subcapsular portion, as a multiple electrode approach, can be used for creating large ablation zones without placing the electrode through the tumor (no tumor touch technique). However, there are also a few disadvantages of switching monopolar RFA with multiple electrodes including technical complexity and increased equipment cost related with the use of multiple electrodes.
In our study, the ablation volume with the switching monopolar RFA (73.8 cm3) was comparable to the results of several preclinical studies using switching monopolar RFA (30, 36, 42, 47). In our study, the maximum diameter of the ablation zone was 5.4 ± 1.6 cm with 2-3 (mean, 2.89) electrodes spaced 1-2 cm apart. Several preclinical in vivo studies using switching monopolar RFA (30, 36, 42, 47) reported an ablation zone with a maximum diameter of 4.2-5.1 cm using three single electrodes spaced 1.5-2.0 cm apart; this was larger than the ablation volumes obtained with monopolar RFA using a single electrode. This improved efficiency of switching RFA may be attributed to the synergistic effect of proximal, concurrently inserted electrodes, as was proven by an in vivo study using porcine livers (30). The synergistic effect of switching the RF system was explained by thermal and electrical synergy, as well as the cooling effect of the vessels. First, multiple electrodes are placed in close proximity and heat is trapped among the electrodes, thus further raising the temperature of the treated tumors (thermal synergy). Furthermore, the switching system is not simultaneously powered, but alternately powered in order to avoid electrical shielding between multiple electrodes. In the switching system, the electrical current flowing from the powered electrodes to the region that is not powered following a voltage gradient, leads to higher temperatures within the spaces (33, 34). Lastly, vascular thrombosis of the ablation zone can reduce the cooling effect of the blood flow around adjacent electrodes.
Recently, several studies evaluating the long-term outcome of consecutive overlapping RFA demonstrated various one-year local recurrence rates from 4% to 17% (48-50). In our study, during a 12.5 ± 4.7-month follow-up period (range, 6-22 months), three of 29 patients with technical effectiveness showed local tumor progression within one year (10%). Indeed, it was very difficult to compare our study results with those of previous studies because the basic values included different mean tumor sizes, follow-up duration, type of electrode used, and major etiology of the HCCs. However, considering the fact that our study included medium-sized HCCs (3.1-4.4 cm in diameter), our results of switching RFA with multiple electrodes are clinically acceptable and have better time efficiency than conventional overlapping RFAs using a single electrode.
There may also be theoretical concerns over the safety of switching monopolar RFAs using multiple electrodes; these concerns include an increased risk of bleeding due to the placement of multiple electrodes, unexpected thermal damage to vital structures, and tumor seeding. However, our complication rates were similar to those of previous reports regarding complications using the conventional RF system with a single electrode (51-54). Only one major complication (3%, 1 of 30) and five minor complications (17%, 5 of 30) were noted in our study. Considering the usual types of complications, most are related to thermal damage to structures adjacent to the treated lesion, such as bile ducts. The risk of thermal damage may increase when a higher temperature is achieved with the more efficient ablation system used to achieve a larger ablation zone. Although all but one of our complications were clinically insignificant, further clinical studies in a larger population will be required in order to demonstrate the safety of switching monopolar RFAs using multiple electrodes.
Our study has limitations. First, as many tumors were located in subcapsular area (within 1 cm from the capsule), ablation size and volume created by switching monopolar RFA could have been underestimated. Second, the follow-up period was too short to assess treatment outcomes regarding tumor progression and patient survival. Finally, as our study consisted of just one series of patients, it did not provide sufficient evidence to prove the superiority of switching monopolar RFA over that of consecutive overlapping RFA. Therefore, a randomized, controlled trial will be needed to prove this. Despite these limitations, our study was adequate as a preliminary report to evaluate the short-term efficacy of using switching monopolar RFA to treat medium-sized HCCs.
In conclusion, switching monopolar RFA is safe, time-efficient, can achieve an adequate ablation volume, and shows short-term therapeutic effectiveness for treating medium-sized HCCs.
Go to :
 XML Download
XML Download