

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
For patients with end-stage renal disease (ESRD) undergoing hemodialysis, appropriate care of vascular access is essential to optimal management (1). The recommended order of the type and location of long-term hemodialysis access is as follows: 1) via an arteriovenous (AV) fistula, rather than a prosthetic AV graft; 2) distal placement; and 3) in the upper extremities, whenever possible (1). In some cases, when there is a prior history of autogenous AV fistula access abandonment with no remaining vessels for creating autogenous AV fistulae, or when there is no candidate for the creation of a primary AV fistula due to small vein diameter (< 2.5 mm), a prosthetic AV graft is recommended.
Frequent thrombosis is a well-known and notorious problem in prosthetic AV grafts, and in 1989 the pulsed-spray pharmacomechanical thrombolysis (PMT) technique was introduced for prosthetic AV graft declotting (2). Since that time the PMT technique has been widely accepted for the treatment of prosthetic AV graft thrombosis, although the long procedure time was problematic. Thus, several mechanical thrombectomy devices, such as the AngioJet rheolytic catheter (AngioJet AVX; Possis Medical, Inc., Minneapolis, MN, USA) and the Arrow-Trerotola percutaneous thrombolytic device (Arrow International, Inc., Reading, PA, USA), have been introduced for the treatment of thrombosed prosthetic AV grafts. Despite the established effectiveness and safety, the increased costs of these devices place a burden on patients, resulting in limited use for patients who have organized thrombi.
Generally, with the traditional PMT technique, a few hours are required for infusion and maintenance of the fibrinolytic agent within the AV graft, and the total amount of the fibrinolytic agent is relatively high (approximately 250,000-1,000,000 IU of urokinase) (2-7). Therefore, even though the traditional PMT technique is the effective method, the long procedure time and hemorrhagic complications related to the amount of fibrinolytic agent are major concerns. We propose that the infusion of a lower dose of urokinase through the AV graft within a shorter time without the use of special devices, such as mechanical thrombectomy devices or multiside-hole infusion catheters, will reduce the procedure time, improve the clinical outcomes, and decrease concerns about hemorrhagic complications, all without incurring additional medical expenses. We applied a modified PMT technique for thrombosed prosthetic AV grafts without the use of special devices, such as mechanical thrombectomy devices or multiside-hole infusion catheters. The aim of this study was to evaluate the efficacy of the modified PMT technique in the endovascular treatment of thrombosed prosthetic AV grafts by analyzing postintervention primary and secondary patencies, and to identify the prognostic factors affecting the outcome.
MATERIALS AND METHODS
Patients
Between March 2005 and October 2009, 761 cases with hemodialysis vascular access in 344 patients were referred from our hospital hemodialysis center and satellite hemodialysis clinics for diagnostic fistulography and/or endovascular treatment. The cases included 548 cases (72%) of prosthetic AV grafts in 169 patients and 213 cases (28%) of AV fistulas in 175 patients. Among the 169 patients with a prosthetic AV grafts, 82 patients (M:F = 42:40; age, 59.6 ± 12.8 years; age range, 29-85 years) with prosthetic AV grafts presented with complete graft occlusion with thrombosis and were treated with the modified PMT technique, followed by angioplasty of the stenotic lesion using a balloon catheter. The material used in all of the prosthetic AV grafts was expanded polytetrafluoroethylene. The other 87 patients presented with a draining vein and/or central vein stenosis with preserved graft patency.
If a decreased or absent thrill was noted on the physical examination through the AV graft, the patient was referred for diagnostic fistulography and endovascular therapy. Exclusion criteria for endovascular treatment of AV graft in our angiography suite were as follows: 1) recent AV graft placement or surgical revision (< 2 weeks); 2) the presence of a risk factor for bleeding from anticoagulation or fibrinolytic therapy; 3) a suspected AV graft infection; or 4) a severe contrast allergy.
Inclusion criteria of the study were as follows: 1) prosthetic AV graft occlusion with thrombosis; and 2) endovascular treatment was attempted for the AV graft salvage. Exclusion criteria were as follows: 1) AV graft occlusion occurring over 48 hours; and 2) a history of endovascular treatment for AV graft salvage performed at outside hospitals.
Table 1 shows the patient characteristics of the study group. Before the procedure was performed, written informed consent was obtained from all the patients. Institutional Review Board approval was obtained for this study.
Collection of Information
We retrospectively reviewed hospital medical records, hemodialysis unit records, angiography suite records, and surgical records of the 82 patients in relation to the hemodialysis and endovascular treatments.
Techniques
All procedures were performed percutaneously in angiography suites by two interventional radiologists with nine and 12 years of experience. The modified PMT technique included the following steps:
1) Pre-procedural examination. A physical examination was performed through the entire prosthetic AV graft.
2) Venous access. After local anesthesia, the AV graft was cannulated approximately 3-5 cm from the arterial anastomosis with an 18-gauge access needle (Becton Dickinson Korea, Ltd., Seoul, Korea) pointing towards the venous anastomosis. A 0.035-inch hydrophilic guidewire (Terumo, Tokyo, Japan) was then passed up to the central vein under fluoroscopy, if possible. Next, a 6-Fr introducer sheath (Terumo) was inserted over the guidewire toward the central vein following the insertion of a 5-Fr catheter (Cook, Bloomington, IN, USA), if possible. An angiogram of the draining and central veins was subsequently performed.
3) Arterial access and thrombolysis. A second AV graft cannulation was performed under local anesthesia, 3-5 cm away from the venous anastomosis using a 5-Fr micropuncture introducer set (Cook) directed towards the arterial anastomosis. The catheter tip was advanced near the arterial anastomosis. After the gentle injection of a small amount of diluted contrast material through the 5-Fr coaxial outer catheter, including a micropuncture introducer set (Cook) to evaluate the arterial anastomosis, while avoiding reflux of the thrombus, 200,000 IU of urokinase (Yuhan, Seoul, Korea) were dissolved in 5 mL of sterile normal saline and the solution was slowly infused over 5 minutes through the catheter to start the thrombolysis under manual compression of the arterial anastomosis. This was followed by gentle manual massage of the AV graft to spread the solution through the clot and to intermittently obstruct the venous limb to aid the penetration of the arterial limb. No additional urokinase infusion was performed. A concomitant systemic intravenous injection of 3000 U of heparin (heparin sodium injection; Choongwae, Seoul, Korea) was performed, as needed, to maintain an activated clotting time > 200 seconds. The urokinase solution was left in situ for approximately 20 minutes. Next, the 5-Fr coaxial outer catheter (Cook) was exchanged for a 0.035-inch guidewire, and the venous anastomosis site stenosis and/or central venous stenosis were dilated using a non-compliant balloon catheter (Blue Max; Boston Scientific, Natick, MA, USA) with a 60-second balloon inflation time. The detailed angioplasty technique was previously described (4). Balloon maceration of the thrombus was subsequently performed first via venous access, and a 6-Fr vascular sheath (Terumo) was then inserted toward the arterial anastomosis, followed by balloon maceration. Balloon maceration was performed through the entire AV graft using an over-the-wire non-compliant balloon catheter (Blue Max) or a semi-compliant balloon catheter (Power Flex; Cordis, Bridgewater, NJ, USA) inflated with 50% contrast solution under fluoroscopy. With respect to the arterial plug, a partially inflated angioplasty balloon was used and gently pulled back through the arterial anastomosis. Then, an angiogram was performed. If a large residual thrombus remained within the AV graft, repeat balloon dilatation was performed to dislodge the thrombus and re-establish flow. Brisk injection of a burst of saline into the AV graft was occasionally used to dislodge the thrombus and re-establish flow. During this thrombolysis procedure, the vascular sheath, which was within the arterial segment, could be temporarily removed over a guidewire to facilitate thrombus removal.
The balloon diameter was chosen at the operator's discretion, generally starting with a balloon 1 mm larger in diameter than the AV graft and/or the patient's previous fistulography or angioplasty report, if available.
Regarding the loop AV graft, the apex-puncture technique was used for the venous and arterial access processes using 5-Fr micropuncture introducer sets (Cook) (8). The arterial and venous access and thrombolysis procedures were performed in the same manner with the above maneuver. In case of clinically significant apical stenosis or thrombus behind the sheath, an additional puncture was performed at the venous limb, followed by PTA or balloon maceration, respectively.
4) Angioplasty. Angioplasty of the stenotic lesions (arterial anastomosis, AV graft venous outflow, and draining or central veins) was performed using a balloon catheter (Boston Scientific or Cordis). The balloon size was determined using a 10-20% oversized balloon, compared with an adjacent normal vein, proximal to the stenosis, and/or the patient's previous fistulography or angioplasty report, if available.
The angioplasty balloon was inflated gradually until the stenosis was eliminated, then the inflation pressure of the balloon was maintained for 60 seconds. If the waist of the stenosis was not eliminated after maximal inflation pressure for 60 seconds, either a cutting balloon (Peripheral Cutting Balloon; Boston Scientific) or a non-compliant high-pressure balloon (Conquest Balloon; Bard, Inc., Covington, GA, USA) was used to eliminate the stenosis (9, 10). If significant residual stenosis was again noted, stenting was performed using a self-expandable nitinol stent (Zilver; Cook or Smart Control; Cordis).
5) Completion angiogram. After a good clinical thrill was detected, a diagnostic angiogram was performed from the arterial anastomosis to the central vein.
6) Hemostasis. The sheath was removed, immediately followed by a circular suture around the cutaneous incision, and additional manual compression, if needed, was performed until hemostasis was achieved (11). The puncture sites were covered with Band-Aid adhesive bandages (Johnson & Johnson Medical Korea, Seoul, Korea).
After successful thrombolysis, the AV graft was immediately used for hemodialysis. No prophylactic antibiotics were used in relation to the procedure. In the case of stenting, anti-platelet treatment was recommended.
Follow Up
All patients were followed up at the hemodialysis units. Follow-up examinations were the same as those used in the surveillance protocol. Patients with abnormal clinical parameters suggestive of AV graft dysfunction, including persistent swelling of the arm, presence of collateral veins, prolonged bleeding after needle withdrawal, or altered characteristics of pulses or thrills in grafts, were referred for repeated fistulography and endovascular treatment. In addition, static pressure in the graft of each patient was directly measured at least monthly using transducers on hemodialysis machines. Therefore, patients with an AV graft exhibiting a venous segment static pressure ratio > 0.5 or an arterial segment static pressure ratio > 0.75 were also referred.
Study Outcome and Definition
The reporting standards from the Committee on Reporting Standards of the Society for Vascular Surgery and the American Association for Vascular Surgery were used to define the AV graft patency (12-14).
Technical success was considered the presence of a patent AV graft at the conclusion of the procedure, as a reduction of the stenosis to < 30% of the luminal diameter on angiogram, based on a good thrill. Clinical success was considered to be at least one successful subsequent hemodialysis session (1).
Post-intervention primary patency was defined as the interval from the time of intervention until thrombosis or until the time of measurement of patency. Secondary patency was defined as the interval from the time of access placement until any intervention designed to maintain or re-establish patency, until access thrombosis, or until the time of measurement of patency (12-14).
Statistical Analyses
Statistical analyses were performed using SPSS for Windows (version 16.0; SPSS Inc., Chicago, IL, USA). Access patency rates were calculated using the Kaplan-Meier method and were compared using the log-rank Mantel-Cox test. Independent predictors of patency were calculated using Cox regression analysis. A p value < 0.05 was deemed to indicate a statistically significant difference.
RESULTS
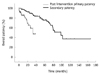
The total number of modified PMT sessions was 279 in 82 patients. The mean follow-up period after the first interventional treatment was 782.2 days (range, 0-2377 days). During the follow-up evaluation, 21 patients (26%) underwent no additional interventions, and the other 61 patients (74%) underwent at least one more intervention. Two patients (2%) were lost to followup. The modified PMT was technically successful in 95% of 82 patients with 279 sessions, and clinically successful in 95% of the patients with technical success. The post-intervention primary patency rates at 3, 6, 12, and 24 months were 80 ± 4.7%, 56 ± 5.9%, 45 ± 6.0%, and 22 ± 5.4%, respectively. The secondary patency rates at 3, 6, 12, and 24 months were 100 ± 0.0%, 98 ± 1.7%, 96 ± 2.1%, and 91 ± 3.2%, respectively. The Kaplan-Meier survival curves for the overall post-intervention primary and secondary patencies of the thrombosed AV grafts are shown in Figure 1. The median durations of the post-intervention primary and secondary patencies were 9.1 ± 3.2 and 97.4 ± 12.7 months, respectively.
Age, gender, history of previous vascular access procedure, AV graft shape (loops, straight, or curved), and AV graft side (right or left) showed no effect on the post-intervention primary or secondary patency rates. The post-intervention primary patency had no effect on the secondary patency rate. There were eight overall stent insertions for the treatment of residual venous stenosis.
There were no major complications that required prolonged hospitalization with surgical or medical treatment. Among all 279 procedures, 29 cases (10%) of minor complications occurred. Vein rupture following percutaneous transluminal angioplasty was a common complication, occurring in 17 cases (16%; 13 venous anastomosis sites and 4 draining veins) treated with ballooning in 14 cases or with a stent in 3 cases). Seven cases (3%) of AV graft extravasation occurred and were treated with manual compression. Three cases (1%) of arterial embolization occurred and were treated with local urokinase infusion. One case (0.4%) of arterial rupture occurred and was treated with ballooning, while one case (0.4%) of arterial dissection occurred and was treated with stent placement. There were no mortalities related to the procedure.
DISCUSSION
Thrombosis is the leading cause of AV graft patency loss. Thus, timely intervention for a thrombosed access is mandatory to re-establish the connection to the artificial kidney.
Since the late 1980s, endovascular treatment methods, such as PMT and mechanical declotting techniques, have been replaced with the AV graft occlusion recanalization treatment method, rather than surgical treatment, and have been shown to be efficacious and safe (2, 4, 6, 15). As a result of technical innovations, several mechanical devices were introduced in the early 1990s, and currently several commercial mechanical devices are widely used for the endovascular treatment of thrombosed AV grafts (16-20). Despite the convenience of handling, the short procedure time, and the effectiveness and safety of these devices, a major drawback associated with the use of these mechanical devices is the high cost.
The current study showed that a modified PMT technique, coupled with close monitoring and early referral, is a highly successful procedure with acceptable long-term secondary patency rates. Based on our modified PMT technique, a urokinase infusion was performed over a relatively short time as the arterial anastomosis site was compressed. This modified PMT technique does not require a multiside-hold infusion catheter for fibrinolytic agent infusion, making it simpler than traditional PMT techniques (3, 4, 6, 21, 22). Also, the total amount of urokinase was 200,000 IU, which may reduce the risk of hemorrhagic complications related to urokinase. In addition, the overall lytic time was 25 minutes, which was much shorter than the traditional PMT technique, and may effectively reduce the overall procedure time. Our study outcomes demonstrated the effectiveness of the technique, with 95% and 95% technical and clinical success rates, respectively. These results are comparable with previous reports using mechanical thrombectomy devices, which reported rates between 80% and 98% (19, 23-27). Moreover, our modified PMT technique results have acceptable post-interventional primary patency and secondary patencies, with low complication rates. Furthermore, our post-intervention primary patency results far exceeded the recommended target of 40% patency at three months, as set by the KDOQI guidelines (1). Continuous AV graft surveillance and early referral for endovascular treatment could improve the long-term patency of AV grafts, and these modalities will contribute to improving the quality of life for hemodialysis patients.
Based on our modified PMT technique, urokinase was infused into the AV graft under manual compression of the arterial anastomosis. However, compared with manual compression, the use of a balloon catheter is expected to result in more effective occlusion of the arterial anastomosis. Although arterial embolization may occur during balloon catheter manipulation, an experienced operator could achieve more effective occlusion.
There were some limitations to our study. This was a retrospective study confined to patients with acute AV graft thrombosis. However, for patients with chronic AV graft thrombosis, endovascular treatment using a mechanical thrombectomy device is an excellent treatment option. In the current study we excluded AV graft occlusion occurring over 48 hours previously from the study analysis, but not the treatment itself, because thrombus age is a bias for analysis of the modified PMT technique. In addition, the overall procedure times and relationship between the lytic time and overall procedure time remain to be evaluated.
In conclusion, our modified PMT technique for thrombosed prosthetic AV grafts is a highly successful procedure with acceptable long-term post-intervention primary and secondary patencies, provided that an endovascular treatment is established to manage subsequent thrombosis.

 XML Download
XML Download