

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Trauma in childhood occurs frequently. Of particular importance is the recognition of fractures caused by child abuse. They are characterized by reporting an inadequate trauma, unusual localizations and more than one fracture of different ages. In radiological diagnostics the primary method is usually X-ray in two or three planes of the injured part of an extremity, including the adjacent articulations. Radiography is an adequate imaging method for all uncomplicated fractures. In addition, good results can be achieved by ultrasound and in some cases radiological occult or missed fractures can be diagnosed (1-3). Some complex fractures, however, require additional imaging to clarify the exact location of the fracture line and the displacement.
A tomographic imaging method such as computed tomography (CT) or magnetic resonance imaging (MRI) is commonly used for further diagnostics. CT, however, exposes the patients to high loads of radiation. This is an important factor since children are up to 10 times more sensitive to radiation exposure than adults (4). However, recent studies have demonstrated that a significant reduction of the dose in skeletal CT is possible without the loss of important details (5-10). Even skeletal CT with doses comparable to doses used in plain film radiography seems possible (11). The aim of this study was to evaluate various doses of CT for pediatric fracture diagnosis and to determine the lowest possible dose for fracture diagnosis that gives reliable results without losing any essential details. Thus, an ex vivo study design was selected that enabled the systematic scanning of the same specimen at different doses.
MATERIALS AND METHODS
Subjects
An animal model was selected for this ex vivo study. The limb bones of young pigs at the age of 4 weeks to 3 months and of an average body weight of 16.6 kg were used. The epiphyseal plates of all bones were not closed and the soft tissue was left intact. The pigs were either land race or a cross-breeding of land race and large white. All pigs, which lived in an experimental farm at the Faculty of Agricultural and Nutritional Sciences of our university, were dead when they were included in the study. None of the pigs were killed for this study. Since non-vital material was used, an approval of the institutional ethical board with regard to the fracturing and imaging of the specimens was not necessary.
The extremities were separated from the pig bodies, and split at the large joints to avoid an exclusive rupture of the joints during the fracturing process. In this way, each extremity was divided into three parts: upper limb, lower limb and paw.
All specimens were fractured with a material testing machine (Lloyd Instruments LR5Kplus, Lloyd Instruments Ltd, Fareham Hants, UK) as a guillotine or a self-made rotation device. In the guillotine, a wedge fell down onto the specimen at a pre-defined velocity and distance. In the rotation device, the specimen was fixed at both ends. One fixation point was rotated against the other by a long lever. Nineteen specimens with 51 bones were examined: 9 paws, 5 upper limbs and 5 lower limbs. On the basis of x-ray diagnosis, 21 bones had simple fractures whereas 11 bones had complex fractures. Another 19 bones had no fracture and were used as controls.
Image Acquisition
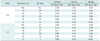
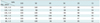
CT examinations were performed with a 64-multislice spiral CT (Siemens Somatom Definition 64, Erlangen, Germany). A special investigative scanner was used under laboratory conditions in which the lower limitation of the tube current was unlocked. Thus even ultra-low dose scans were possible. Ultra-low dose meant 0.05 mSv or less total effective whole body dose. Three different tube voltages of 120 kVp, 100 kVp, and 80 kVp were combined with 6 different tube current time products of 100 mAs, 50 mAs, 40 mAs, 30 mAs, 20 mAs, and 11 mAs as well as with two different pitch factors of 0.9 and 1.5. The systematic combination of these parameters resulted in 36 different dose levels (Table 1). The automatic tube current modulation was deactivated. A gantry rotation time of 0.5 s was chosen. The slice collimation was 64 × 0.6 mm. A very sharp reconstruction algorithm (B 70) was used. The reconstructed slice thickness was 1 mm and 5 mm, whereas the reconstruction increment 0.5. The effective dose was calculated for all scans on the basis of the dose length product, the scan length and, as usual in children, the head phantom. The dose values are shown in Table 1. A digital radiography unit with flat panel detector (Siemens Aristos, Erlangen, Germany) was used for X-rays. The adjustment was 55 kV, 3.6 mAs, and a film-focus distance of 1.15 m without using a Bucky's diaphragm. X-rays were made in two planes perpendicular to each other, in cases of paws in three planes as usually done in clinical practice. The calculated effective dose for routine X-rays is about < 0.01 mSv.
Image Interpretation and Analysis
All scans were analyzed independently by two experienced pediatric radiologists (JDM, DS) 15 months after scanning to ensure that none of the specimens were kept in mind. All data sets were randomized and blinded with regards to the specimen as well as to the dose level. The analysis was carried out at a 3D workstation (Wizard®, Siemens, Erlangen, Germany) in a multiplanar viewing modus with free use of PACS tools. Both radiologists were allowed to individually use the workstation. The analysis was done over a time period of three months to exclude a recall effect.
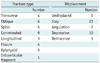
On the basis of the following four defined criteria the quality of the CT scans in the fracture diagnosis was evaluated. The first criterion was the existence or absence of a fracture. For the second criterion, in cases of a fracture, the fracture type was determined according to the following routinely used fracture types: transverse, oblique, spiral, comminuted, longitudinal, and epiphysial fracture, fissure, and intra-articular fragment (Table 2). The third criterion was the description of the displacement according to the following kinds of displacement: step, angulation, depression, and dehiscence (Table 2). In complex fractures a combination of more than one type of fracture and/or displacement was necessary for correct description. Examinations with the highest dose level (120 kVp, 100 mAs, and pitch 0.9) acted as the gold standard separately for each observer. For the fourth criterion, a ranking was specified for the degree of diagnostic certainty: 0 (determination not possible), 1 (determination doubtful), 2 (determination rather certain), and 3 (determination absolutely certain). A ranking of 2 or higher was considered sufficient for diagnostics.
Summarizing the results of these four criteria enabled us to evaluate which of the various dose protocols were sufficient for fracture diagnosis. Only those scans in which a fracture or a non-fracture was correctly detected, the fracture type correctly described, the fracture displacement correctly identified, and the degree of diagnostic certainty 2 or higher obtained a positive overall result. A rate of success was calculated for each dose level. In the style of other statistical analyses we decided to tolerate a portion of maximal 5% incorrect results within a dose protocol. Thus, a rate of success of 95% or higher was considered sufficient for diagnosis.
Statistical Analysis
To obtain a degree for variability, the interobserver agreement was determined for the highest dose. Confidence intervals for binominal probabilities were calculated with the statistics program BIAS for Windows 8.03 Germany. Simultaneous confidence intervals for multinomial probabilities were determined following the method of Goodman (12). Comparison of the two observers was made by means of a McNemar test for 2 × 2 contingency tables and by means of Stuart's test (13) for 2 × 3 contingency tables. A p value of less than 0.05 was considered significant and all tests were two-sided. As measure of agreement between the two observers, the proportion of overall agreement and kappa index was calculated. All calculations were done employing either the statistics program BIAS for Windows 8.03 or the statistics program R (14). Since the study is of explanatory nature, no adjustment for multiple testing was applied and only unadjusted p values are shown.
RESULTS
First Criterion: Existence or Absence of a Fracture
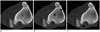
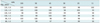
Only the lowest dose level (80 kVp, 11 mAs, pitch 1.5) had a rate of success lower than 95% (91%, 7 wrong out of 102 results) for this criterion and was consequently considered insufficient for diagnostics (Table 3) (Fig. 1). In the entire study, a fracture was missed or wrongly described in just 54 out of 3672 results. The majority of missed fractures were undislocated fissures (n = 44) (Fig. 2). Only in four cases of low dose scans were dislocated fractures missed: three cases of a longitudinal fracture with a minor impression and one case of a fissure with a small step. Two low dose scans achieved a false positive result: a Salter-Harris fracture and a fissure. A total of 73% of missed fractures (n = 39) were related to small tubular bones of the paws, 27% (n = 15) to long tubular bones.
Second Criterion: Determination of Fracture Type
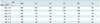
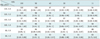
Only two ultra-low dose levels were considered to be insufficient for diagnosis of this criterion: 80 kVp, 11 mAs, pitch 0.9 and 80 kVp, 11 mAs, pitch 1.5 (Table 4). Looking at all dose levels there were a total of 116 cases with a wrongly determined fracture type. An extent of the fracture into the epiphysial plate (Salter-Harris) was not recognized in 27% of cases with a wrongly described fracture type (n = 31), and a comminuted fracture was not identified in 25% (n = 29) of the cases. In 38% of cases with an incorrect fracture type (n = 44), one part of a complex fracture was not recognized. A total of 77% of wrongly determined fracture type (n = 89) were related to small tubular bones of the paws, whereas 23% (n = 27) were related to long tubular bones.
Third Criterion: Description of Fracture Displacement
The results of all dose levels achieved rates of success of 95% or higher in this criterion (Table 5) (Fig. 3). All wrongly described fracture displacements (n = 38) concerned the small tubular bones of the paws. In 15% (n = 6) of cases, one or more components of displacement in complex fractures were not recognized. The most frequently missed type of displacement was an impression.
Positive Overall Result
The analysis of the overall result, which is composed of the three above mentioned individual results as well as a sufficient degree of diagnostic certainty, showed that altogether 10 of the examined dose levels failed to achieve the required rate of success of 95% (Table 6).
Interobserver Agreement
Interobserver agreement was only considered for the gold standard, which was the highest dose level. Concerning the fracture identification the proportion of overall agreement was 96.1%, the kappa index was 0.92 (0.64; 1.00), and the p value for comparison was 0.25. In 2 out of 51 bones, one observer did not identify a fracture, which the other observer described as a fissure. In the category fracture type a proportion of overall agreement of 93.3%, a kappa index of 0.91 (0.7; 1.00), and a p value for comparison of 0.16 were achieved. Only in 2 out of 32 fractured bones were completely different fracture types described. In another 5 cases the fracture type was partially the same. With regards to the displacement, the proportion of overall agreement was 78.4%. In 7 out of 32 fractured bones, the two pediatric radiologists found different types of displacement and in another 4, one observer did not describe one part of displacement. In all cases with different displacements, small steps or discrete impressions were recognized by only one observer.
Comparison of the Radiation Dose
On the basis of the above mentioned criteria, a protocol of 120 kVp, 11 mAs and a pitch of 1.5 was the lowest one considered as sufficient for diagnostics. At this dose level, none of the individual diagnostic criteria had a rate of success lower than 98%, and the rate of success was 96% for the overall result. Its effective dose of 0.03 mSv was about three times the effective dose accumulated by standard X-rays in two planes. The CTDIvol of this dose was 0.48 mGy. A standard protocol for trauma diagnosis in children in our clinic (120 kVp, 60 mAs, pitch 0.75) has a CTDIvol of 4.97 mGy, which is 10 times higher than the value of this ultra-low dose protocol.
DISCUSSION
Up till now, only a few studies have used low dose CT for the detection of skeletal lesions in multiple myelomas (15, 16) or of skeletal landmarks in the temporal bone (9, 10). There are only some studies that have indicated low dose CT offers adequate image quality for fracture diagnosis of the spine (6, 11).This study examined tubular bones of the extremities of pigs and demonstrated that in these bones an adequate fracture diagnosis is possible even with ultra-low dose CT. There were some difficulties in the identification of undislocated fissures with ultra-low dose CT. CT, however, is usually used to examine complex fracture types, typically with displacement, which could be identified reliably, even with a distinct reduction of dose levels in this study.
Modern multi-detector CT (MDCT) offers different possibilities for a reduction of the radiation dose. By modulation of the tube current to the diameter of the object to be scanned, a significant decrease of the radiation dose is possible. In this study, however, this feature was deactivated to avoid an automatic increase in the tube current in ultra-low dose scans. Another possibility for reducing the radiation dose is the use of lower tube voltage settings. Although a decrease of the kVp causes a lower effective dose, it was shown that if the mAs could be reduced significantly, lower patient doses could be obtained with the advantage of greater X-ray transmission and decreased absorption of energy by the patient per exposure (16, 17). The highest possible savings in radiation dose can be achieved by a reduction of the tube current in addition to an increase of the pitch factor (7). According to these criteria, CT scans can be produced with radiation doses that are comparable to those of plain film radiography. These scans have sufficient diagnostic certainty for specific problems (11, 18, 19). In accordance with this, the best results were detected by a reduction of the tube current in combination with an increase of the pitch factor in this study. The effective dose of the lowest dose level sufficient for diagnostics was about three times the effective dose accumulated by standard X-rays in two planes. Even CT scans with radiation doses equivalent to plain film radiography were diagnostically accurate for the detection and characterization of some fractures.
Certainly the image quality declines and the image noise increases as the radiation dose declines. Although the image quality was poor in the lowest dose levels of this study and soft tissue structures were differentiated with difficulty, cortical detail remained adequate in the majority of cases allowing sufficient diagnosis of nearly all fractures except a few undislocated fissures. Pediatric orthopedics and surgeons demand high quality imaging. However, it is important to determine whether a scan is adequate as long as it makes high quality pictures or allows sufficient diagnostics with detection of all relevant details. There are some possibilities to decrease image noise by mathematical noise reduction algorithms (20) and to generate pictures of better quality. This was not tested in our study and will be the objective of further studies.
Some Limitations of This Study
It was not practicable to make a precise statistical analysis for comparison of the different dose levels in CT due to the numerous examined variables and the high number of different dose levels. Thus, we calculated a rate of success for the overall result of each dose level. Due to unavoidable errors we could not expect a rate of success of 100% even in scans with adequate dose levels. Thus, we decided to tolerate a portion of 5% incorrect results within a specific dose level. According to this limitation all dose levels with a rate of success below 95% were considered insufficient for diagnostic.
As it is common for standard dose skeletal CT, we used a sharp reconstruction algorithm to optimize the assessment of osseous structures. The sharp reconstruction algorithm, however, leads to an increase in visible image noise, especially in low dose and ultra-low dose scans. This causes further impairment of soft tissue differentiation. In whole body scans a middle-frequency reconstruction algorithm (B50f kernel) proved beneficial for all energy protocols (15). By smoothing the image and reducing the visible noise, the contrast resolution improved to some degree. In this study it was necessary to limit the scan reconstruction to one algorithm. More than one reconstruction algorithm would increase the number of variables resulting in a non-justifiable amount of scans to be analyzed. The evaluation of different reconstruction algorithms must be included in further studies limited to fewer dose levels.
A test of different dose levels in CT is not allowed with patients, especially with children, for reasons of radiation protection. One possible approach is an ex vivo study such as the one performed here. Some studies demonstrated that the structures of pigs' bones are comparable to human bones and therefore these studies used pig bones for simulating pediatric bones (21-23). In addition, bones of young pigs with open growth plates simulate pediatric bones. With intact soft tissue the young pig model is sufficiently similar to the scanning conditions used for children and this approach allows actual examinations. The limitation of this approach is that copying the results one to one from the experimental model to children is not allowed. Thus, it must be proved whether the lowest sufficient dose of this study is also suitable for fracture diagnosis in patients with regards to radiation load and diagnostic certainty. Nevertheless, this study permits the conclusion that a significant reduction of CT dose is possible in pediatric fracture diagnosis even in patients.
The CT scan with the highest radiation dose was chosen as the gold standard. Preparation of specimens with removal of complete soft tissue would have been optimal to achieve a gold standard, but such a procedure would change the fracture displacement because the fragments are fixed by the soft tissue in most complete fracture cases. Moreover, a change of fracture type could not be excluded since additional fractures in thin fragments could occur during preparation.
Conclusion
This study demonstrates that an ultra-low dose CT offers the potential of a dose reduction down to 10% of the standard, and only three times the dose of plain film radiography, when imaging fractures in this animal model. A protocol with the lowest dose level sufficient for diagnosis is 120 kVp, 11 mAs, pitch 1.5. This study indicates that CT protocols for pediatric trauma scans should be reviewed.


 XML Download
XML Download