

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the coronary magnetic resonance angiography (MRA) method has been in development for more than a decade, no consensus has been reached as to the type of sequence to take or the need for contrast agent (1). Major challenges for this technique include the motion artifacts produced in respiration and cardiac contraction. Respiratory motion can be minimized using the navigator-gated technique, in which a special navigator echo monitors motion of the diaphragm during free breathing. Based on the position of the diaphragm, a decision is made to either accept or reject the data (2, 3). To attenuate cardiac motion, the coronary MRA is usually set to acquire images during mid-diastole. Another relatively quiescent period occurs, however, at the end of ventricular systole. Heart rate (HR) variability affects the duration of systole to a lesser degree than the duration of diastole (4-7). For this reason, end-systole imaging may alternatively be used to minimize the artifacts of HR variability.
The recent instruction of non-enhanced steady-state free precession (SSFP) MRA has met with wide acceptance for its accuracy in coronary MRA at 1.5 Tesla (T) (2, 8-11). This sequence has high blood signal-to-noise (SNR) and blood-myocardium contrast-to-noise ratios (CNR). Using SSFP with coronary MRA at 1.5T, Gerber et al. (12) reported the sensitivity at 62%, specificity at 84%, and accuracy at 80%, even for distal segments of the coronary arteries.
Coronary MRA is conventionally performed by a thin-slab volume-targeted approach. A few studies have reported on whole-heart coronary MRA at 1.5T, but these have shown significantly greater resolution of coronary artery length, higher SNR, and easier setup compared with the volume-targeted approach (13-16). Therefore, the purposes of our study were to validate the optimal cardiac phase and proper acquisition window for three-dimensional (3D) whole-heart coronary MRA with SSFP at 1.5T, and to compare the image quality using SSFP with that obtained using a fast low-angle shot (FLASH) MRI.
MATERIALS AND METHODS
Subjects
Thirty healthy volunteers (M:F = 25:5; mean age, 35 years; range, 24-54 years) underwent a coronary MRA. Volunteers with contraindications to MR imaging (automatic implantable defibrillators, pacemakers, and intracranial aneurysm clip) were excluded from this study. No beta-blocker or nitroglycerine was administered to any patient. The Institutional Review Boards approved this study, and all volunteers gave their written informed consent to participate.
True Fast Imaging with Steady-State Precession Coronary MR Angiography Protocol
Cardiac MR imaging was performed with a 1.5T scanner (Magnetom Avanto; Siemens Medical Solutions, Erlangen, Germany) equipped with 16 channels of body array and a maximum strength of 45 mT/m using a gradient system and a maximum slew rate of 200 mT/m/s. Scout images of the heart were first obtained with true fast imaging with steady-state precession (FISP), and then multi-phase true FISP images showing a transverse section of the middle right coronary artery (RCA), to determine the rest periods at end-systole and mid-diastole of the cardiac cycle (i.e., the periods of least motion for the RCA). 3D whole-heart coronary MRA (specifically, a true FISP respiratory-gated, ECG-triggered, fat saturated, and segmented technique) was then performed three times in random order: 1) at end-systole with a narrow (120-msec) acquisition window (ESN); 2) mid-diastole with narrow window acquisition (MDN); and 3) mid-diastole with a wide (170-msec) acquisition window (MDW) (Fig. 1).
The imaging parameters for the segmented 3D true FISP sequence were as follows: TR/TE = 373.3/1.6 milliseconds, flip angle = 90°, bandwidth = 590 Hz/pixel, field of view = 384×512 mm, matrix = 256×256, slice thickness = 0.8 mm, and voxel size = 1.4×1.3×0.8 mm3. To improve blood-to-myocardium contrast, a T2 preparation (40 msec) was applied. A parallel imaging factor of two was applied in the phase-encoding direction to accelerate data acquisition.
Contrast Enhanced Coronary MR Angiography Protocol
All volunteers underwent a contrast enhanced coronary MRA after undergoing an unenhanced 3D true FISP MRA three times. Contrast enhanced coronary MRA was performed with a respiratory-gated, ECG-triggered, fat-saturated, segmented 3D FLASH sequence without T2 preparation. The imaging parameters were as follows: minimum TR/TE, flip angle = 20°, bandwidth = 200 Hz/pixel, field of view = 256×256 mm, matrix = 256×256, slice thickness = 1.0 mm, and voxel size = 1.0×1.0×1.0 mm3. To minimize HR variability, the acquisition windows were adjusted to mid-diastole with a narrow window (Gd-MDN), which was comparable to the MDN condition in a true FISP sequence. Gadobutrol (Gadovist; Schering, Berlin, Germany) at 0.1 mmol/kg was injected slowly (1 mL/s) using a power injector (Nemoto; Nemoto Kyorindo, Tokyo, Japan), followed by 20 mL of normal saline at the same rate.
Data Analysis
The average acquisition time and trigger delay time were evaluated for each acquisition method.
The image sets were transferred to a postprocessing workstation (Aquarius Workstation V3.6; TeraRecon, San Mateo, CA). Curved multiplanar reconstructions (MPR) and maximum intensity projections (MIP) were obtained along the coronary artery courses. The visibility of the coronary segment, image quality, SNR, and CNR were evaluated for the four different methods by two readers who had more than 10 years and three years of experience, respectively in cardiac MR interpretation.
Visibility of the coronary artery was evaluated for the following 11 segments, as defined in the American Heart Association (AHA) guidelines (17): the left main (LM) coronary artery, proximal left anterior descending (LAD) artery, middle LAD artery, distal LAD artery, proximal left circumflex (LCx) artery, middle LCx artery, distal LCx artery, proximal RCA, middle RCA, distal RCA and posterior descending artery (PDA). The readers scored image quality by a 5-point scale: 1, not visible; 2, poor (severe motion artifacts or poor fat saturation); 3, fair (delineated vessel lumen with moderate artifacts); 4, good (vessel delineation with minor artifacts); 5, excellent (clear vessel delineation without artifacts) (Fig. 2). Visibility of coronary segments and image quality were evaluated from the MPR images. SNR and CNR were calculated from the original images. The region of interest (ROI) for measuring the blood signal intensity was placed centrally in the lumen of the proximal (within 3 cm from the origin) areas of the LAD, LCx, and RCA. The electronic cursor was set to be as large as possible in the vessel lumen. Myocardial signal intensity was measured from the myocardium immediately next to each coronary artery. We determined mean values for each signal intensity measured at the proximal area of a coronary artery and at the surrounding myocardium. Noise measurements in parallel imaging techniques with inhomogeneous noise distributions cannot be directly compared. Hence for the background signal intensity value in the noise assessment, we used the mean of the signal intensity values obtained for two large air ROIs outside the chest wall. The SNR and CNR were defined according to the following equations:
SNR = Mean (SIcoronary artery)/SDair and
CNR = SIcoronary artery - SImyocardium / SDair, in which SI is the signal intensity and SD is the standard deviation of the signal intensity of air outside the chest wall (18).
Statistical Analysis
All parameters were determined as the mean ± standard deviation. Friedman's test was used to compare scan times for the acquisition methods, the number of visualized segments of the coronary artery, and image quality, SNR and CNR. A post-hoc Wilcoxon rank sum test with Bonferroni correction was performed to determine between which groups' differences existed. Calculations were performed with SPSS (version 12.0.1, Statistical Package for the Social Sciences, Chicago, IL).
RESULTS
All 30 volunteers completed coronary MRA without complications. The mean HR during MRA was 64.0 ± 5.3. The average of the total MR acquisition time (including scout imaging and four coronary MRA protocols) per each patient was 56.2 ± 8.7 min. A significant difference in acquisition time was found between scan protocols: 12.1 ± 3.4 min in the ESN, 12.0 ± 2.0 min in the MDN, 8.9 ± 2.4 min in the MDW and 22.2 ± 3.5 min in the Gd-MDN (p < 0.05). Mean acquisition time was significantly shorter in the MDW than in the ESN and MDN with an SSFP (p < 0.01). The acquisition time was significantly longer in the Gd-MDN than in the three methods with an SSFP sequence (p < 0.01). The mean trigger delay time determined by the RCA imaging with a multi-phase SSFP sequence was 273.3 ± 27.5 msec (range, 220-330) for the ESN imaging, 621.0 ± 72.1 msec (range, 450-760) for the MDN imaging, and 594.7 ± 73.4 msec (range, 430-740) for the MDW imaging (Table 1).
Of the 330 coronary artery segments evaluated in 30 volunteers, 316 (96%) were visualized in the ESN; 317 (96%) in the MDN; 310 (94%) in the MDW; and 283 (86%) in the Gd-MDN (p < 0.05). The coronary artery segment visibility was significantly lower in the Gd-MDN imaging technique than in the other three methods with an SSFP sequence (p < 0.01). However, the other three methods did not differ significantly in visibility (p > 0.05).
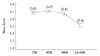
Mean image quality scores were 3.6 ± 0.8 in the ESN, 3.7 ± 0.8 in the MDN, 3.6 ± 0.9 in the MDW, and 2.8 ± 1.1 in the Gd-MDN. The image quality scores for the ESN, MDN and MDW did not differ significantly, but the Gd-MDN sequence produced a lower quality image of the coronary arteries than did any of the other three methods with an SSFP (p < 0.01) (Fig. 3).
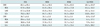
The SNR and CNR are summarized in Table 2. Mean SNR in the coronary arteries was 65.1 ± 6.5 in the ESN, 64.1 ± 2.0 in the MDN, 52.9 ± 3.5 in the MDW, and 48.1 ± 13.8 in the Gd-MDN. Although the mean SNR was a little lower in the MDW than in the ESN or MDN, these values did not differ significantly (p > 0.05). The SNR was significantly lower, however, in the Gd-MDN than in the other three methods with an SSFP (p < 0.05). Mean CNR was 36.7 ± 6.5 in the ESN, 36.1 ± 2.0 in the MDN, 30.3 ± 3.5 in the MDW, and 8.9 ± 13.8 in the Gd-MDN. While CNR in the ESN, MDN, and MDW did not differ significantly (p > 0.05), the Gd-MDN showed a significantly lower CNR than any of the other three methods (p < 0.05).
DISCUSSION
This study demonstrates superior results overall for coronary MRA with SSFP, compared to a Gd-enhanced FLASH, using a 1.5T scanner. The SSFP sequence produces significantly higher visibility of the coronary artery segments, better image quality, higher SNR and CNR than Gd-enhanced FLASH sequence. The narrow acquisition window at mid-diastole with an SSFP gives a relatively good image quality and good SNR. However there was no significant difference in the ESN, MDN, and MDW with the SSFP sequence.
An SSFP sequence produces good results in coronary MRA at 1.5T using a volume-targeted approach because of its intrinsically high blood signal intensity and bloodmyocardial contrast (2, 8). Contrast medium is not required in this approach because it does not significantly improve the visibility of coronary segments, length of vessel visualized, or image quality (19). Recently, however, Weber et al. (2) introduced 3D whole-heart coronary MRA that reveals the entire group of coronary arteries in a single acquisition. This technique permits subsequent reformations in arbitrary orientations and reformations for manifold imaging. These advantages, not shared with the conventional volume-targeted approach, simplify the planning and performance of coronary MRA. In this study, we found that 3D whole-heart coronary MRA using an SSFP sequence provided excellent image quality, and good CNR and SNR in the coronary artery images. In contrast, a 3D whole-heart FLASH sequence at 1.5T did not improve the coronary segment visibility, image quality, SNR, and CNR.
The long acquisition time for 3D whole-heart coronary MRA presents a challenge because it may lead to motion artifacts such as HR variations and respiratory drifts. The use of parallel imaging techniques may help to reduce acquisition times (13, 20). Nehrke et al. (14) reported that a short scanning time of about four minutes with free breathing increases patient comfort and allows a whole-heart coronary MRA with sufficient SNR and spatial resolution to show the main trees and major branches of the coronary arteries. Sakuma et al. (13) also reported reliable 3D imaging of the coronary arteries with 82% sensitivity and 91% specificity in detecting coronary artery stenosis.
Reducing cardiac motion artifacts may significantly improve image quality in the coronary MRA. Motion correction in the coronary CT angiography is generally performed by means of retrospective rearrangement of multi-section partial scan data relative to an ECG signal that is recorded during image acquisition (21). In contrast to coronary CT angiography, coronary MRA usually limits the data acquisition window to a portion of mid-diastole, in which cardiac motion is expected to be minimal. To acquire the data sets at end-systole during the other low motion period in the cardiac cycle, we need to perform an additional scan. The low motion period at the completion of ventricular systole occurs in approximately 34% of the cardiac cycle, and lasts for approximately 118 msec (range 0-223 msec) (4). The duration of systole is less affected by HR variability than the duration of diastole (22). Gharib et al. (23) found no significant differences in image quality when comparing mid-diastole and end-systole, nor for comparing vessel lengths, suggesting that imaging during end-systole is least affected by HR variability. In our study, we found no significant differences between end-systole and mid-diastole images with respect to coronary segment visibility, image quality, SNR or CNR.
One advantage of coronary MRA is the ability to manipulate the scan window for image acquisition, and therefore, the acquisition time: the wider the acquisition window, the shorter the acquisition time (24). Although the acquisition time in our study did not differ significantly between the narrow window (120 msec) and the wide window (170 msec) at mid-diastole, the narrow window acquisition slightly increased acquisition time. However, the narrow window acquisition produced a much higher SNR (but not CNR) than the wide window acquisition. A higher SNR facilitates the evaluation of coronary artery disease and the 3D reformation of image data.
An MRA to evaluate the vascular system is most commonly performed with an intravenous administration of contrast material. Recent studies suggest, however, that an SSFP sequence gives better results for the abdominal and thoracic aorta with its branches than contrast-enhanced MRA (25-27). Our study showed consistently better performance for an SSFP without contrast material than for the Gd-enhanced coronary MRA. The coronary MRA with SSFP gives better image quality, as well as SNR and CNR than the Gd-enhanced coronary MRA and is also faster. The SSFP may therefore provide an excellent method for 3D whole-heart coronary MRA at 1.5T, although the contrast-enhanced coronary MRA with a FLASH sequence may be superior at 3.0T (28-30).
Our findings present several limitations. First, we performed our study in healthy volunteers. We did not evaluate the diagnostic accuracy of the 3D whole-heart coronary MRA as compared to a coronary CT angiography or conventional coronary angiography. Second, we based the coronary rest period determination on cross-sectional RCA images only. On average, the RCA moves more than twice as much as the LCA, and had a significantly shorter and later rest period (4, 6).
In conclusions, the application of contrast enhanced coronary MRA with the FLASH sequence does not help to improve the visibility of coronary segments, image quality, SNR, and CNR in 3D whole-heart coronary MRA at 1.5T. The use of an SSFP sequence provides an excellent method for the 3D whole-heart coronary MRA. Use of a narrow acquisition window improves the SNR, although it increases the acquisition time.



 XML Download
XML Download