

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Permanent pacemakers and implantable cardioverter defibrillators (ICD), also known as cardiovascular implantable electronic devices (CIED), are being increasingly employed for the treatment of patients suffering from various cardiac arrhythmias. Overall, there are 4.5 million people worldwide with a CIED (1). CIED implantation has been associated with both acute and delayed complications. Following pacemaker implantation, up to 22% of patients may evidence abnormalities on post-interventional chest radiographs (2). Chest radiographs are helpful in evaluating the lead position and integrity following implantation, and are also helpful in identifying CIED-associated complications. Chest radiographs should be acquired in both posterior-anterior and lateral projection using the hard beam technique (tube potential ≥ 110 kV). Chest CT scans (e.g. tube potential 110 kVp; tube current 100 mAs) may provide more detailed information regarding thoracic complications and CIED. If necessary, ECG-triggered cardiac CT can visualize exact lead positions and potential lead perforations.
Correct Position of Pacemaker Leads according to Pacemaker Types
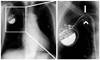
Pacemaker systems are generally composed of a pulse generator and one or more leads (Fig. 1). Pulse generators consist of a titanium body which contains a lithium iodine cell. The pulse generator is preferentially implanted in a subcutaneous pocket at the pectoralis muscle, although other locations such as the abdomen, especially in pediatric patients, can also be used.
Pacemaker leads consist of metal conductors with a silicone or polyurethane isolation. Leads are preferably inserted via the cephalic or subclavian vein, but can also be inserted via the jugular or femoral vein. Generic codes of the North American Society of Pacing and the British Pacing and Electrophysiology Group describe the mode of operation of these devices, which generally consist of three positions describing the chambers that are paced (first letter) and sensed (second letter) and the response to sense events (third letter). A fourth position is used if the pacemaker adjusts the pacing rate in response to exercise (R). A fifth position can be used as well, to describe the chambers in which multisite pacing is delivered (Table 1).
Knowledge of the typical lead positions for each pacemaker and ICD type is essential for correct interpretation of chest radiographs (Tables 2, 3).
VVI Pacemaker
Chronic atrial fibrillation with ventricular bradycardia is the principal indication for VVI pacemakers, which consist of a single ventricular lead (Fig. 2). In the case of ventricular pacing, the atrium might be exposed to a non-physiological retrograde stimulation, which may result in atrioventricular dyssynchrony with reversed atrial blood flow and abnormal atrial pressure waves ("pacemaker syndrome") (3).
AAI Pacemaker
The most frequent indication for an AAI pacemaker is a sick sinus syndrome. AAI pacemakers consist of a single atrial lead (Fig. 3). An intact AV conduction is required for the application of this type of pacemaker. The main disadvantage of this pacing modality is an increased risk of atrioventricular blockade in patients with sick sinus syndrome.
DDD Pacemaker
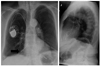
DDD pacemakers consist of two leads--one in the right atrium and one in the right ventricle (Fig. 4). The main indication for a DDD pacemaker is symptomatic failure in AV conduction (AV block °II and °III) in combination with sick sinus syndrome. The majority of newly implanted pacemakers are DDD pacemakers (4).
Biventricular Pacemaker for Cardiac Resynchronization Therapy (CRT)
Severe heart failure with left-sided intraventricular conduction delay is the most common indication for a biventricular pacemaker. Pacemaker electrodes are placed in the right atrium, the right ventricle, and the left ventricle (via the coronary sinus) for the synchronization of atrial and ventricular contractions, which improves the cardiac ejection fraction (5) (Fig. 5).
Implantable Cardioverter Defibrillator
Implantable cardioverter defibrillators (ICD) are employed for primary and secondary prophylaxis of sudden cardiac death from ventricular tachycardia in high-risk patients (Fig. 6). ICDs are mainly implanted in patients with a history of ventricular fibrillation and sustained ventricular tachycardia. A meta-analysis of secondary prevention ICD trials demonstrated a significant (50%) reduction in arrhythmic death (6). ICDs can also have a post-shock pacing function. Depending on the pacing functions, additional leads can be found in the right atrium and branches of the coronary sinus at the left ventricle.
Lead Positions in Patients with Anatomic Variations and after Cardiac Surgery
Persistent Left Superior Vena Cava
Persistent left superior vena cava (PLSVC) is the most common venous anomaly of the thorax and can be seen in 0.5-2% of the general population and up to 10% of patients with congenital heart diseases (7). Venous blood from the PLSVC is generally directed to the right atrium via a large coronary sinus (Fig. 7). Pacemaker implantation has been reported to be more challenging in patients with a PLSVC, particularly in the absence of a bridging vein between the PLSVC and the right superior vena cava (7).
Tricuspidal Valve Surgery
Following cardiac surgery, up to 21% of patients may require a permanent pacemaker (8). The ventricular lead can be guided through a reconstructed tricuspidal valve to the right ventricle (Fig. 8). In patients having undergone a mechanical tricuspidal valve replacement, the ventricular lead should not traverse the mechanical valve. The ventricular lead can be placed at the right ventricle via the coronary sinus as an alternative to epimyocardial leads (Fig. 9).
Mustard Procedure
Transposition of the great arteries (TGA) accounts for 5-7% of congenital heart diseases. Arterial switch surgery is currently regarded as the therapy of choice in patients with TGA. However, the Mustard procedure was generally performed in the past to direct venous blood via a "baffle" to the left atrium and oxygenated blood from the pulmonary veins to the right atrium (Fig. 10). In up to 65% of patients having undergone Mustard surgery, cardiac arrhythmias might develop, possibly requiring ICD and/or pacemaker implantation (9).
Malposition and Complications Following Pacemaker Implantation
According to recent literature, the overall incidence of short-term implantation-related complications has been reported to be as high as 12% (10) (Table 4). Aside from pocket hematoma, which may not be visible on chest radiograph, lead dislodgement and unsatisfactory lead positions are the most common complications, and may account for up to 27% of all complications (10-12) (Figs. 11, 12, 13, 14).
Twiddler Syndrome
Twiddler's syndrome describes a rare condition of pacemaker malfunction. Patients cause lead dislodgment by often unconscious manipulation of the pacemaker generator in its subcutaneous pocket (15). Twiddler's syndrome can be readily diagnosed on chest radiograph and generally appears within the first year after implantation (Fig. 15). Besides female gender, obesity and older age, dementia is generally regarded as the most important risk factor (15).
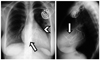
Lead Fractures
Lead fractures can occur at any timepoint following implantation. The incidence ranges between 1 to 4% (16, 17). Lead fractures may appear as a complete disruption of the lead or as subtle damage to the lead. The most common sites are the connection point to the generator and the area lateral to the subclavian venous entry site, where the lead might be compressed between the clavicle and the first rip (subclavian crush syndrome) (18) (Figs. 16, 17).
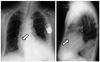
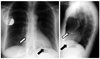
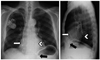
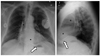
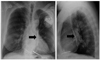
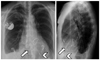
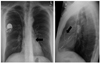
Cardiac Perforation
Symptomatic heart perforation in the short-term after pacemaker implantation is rare (0.4-1%) and may be associated with pericardial effusions, which may result in cardiac tamponade (19, 20). Additionally, a handful of case reports have described contralateral pneumothorax as a result of myocardial and pleural lead perforation (21). Delayed asymptomatic perforation has been described to occur in 15% of patients. Asymptomatic atrial perforation occurs more frequently than ventricular perforation (22) (Figs. 18, 19, 20, 21).
Postcardiotomy Syndrome
The postcardiotomy syndrome (PPS), also referred to as Dressler syndrome, has been widely described after cardiac surgery. It generally manifests 1-3 months after surgery with the most clinical symptoms of fever, chest pain, and pericardial effusion. The underlying pathophysiology has yet to be thoroughly understood, although an autoimmune response to disturbance of the pericardial integrity is believed to play an important role in this phenomenon. In rare cases, PPS has also been reported following pacemaker implantation in adults and children (23) (Fig. 22).
















 XML Download
XML Download