

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Patients with acute massive gastrointestinal bleeding are a most challenging group because this disease is associated with a high mortality rate. Acute massive gastrointestinal bleeding involves symptoms of hematemesis, melena, or hematochezia that causes hemodynamic instability (hypotension with systolic blood pressure < 90 mmHg) or required transfusion of at least four units of blood within 24 hours of symptoms of acute bleeding. By anatomic definition, the blood loss proximal to the ligament of Treitz, from the esophagus, stomach or duodenum, is defined as upper gastrointestinal hemorrhage. And, the lower gastrointestinal hemorrhage is bleeding distal to the ligament of Treitz that originates from the small intestine or colon. Advanced age, rebleeding, respiratory failure, coagulopathy and co-morbidities are the most important risk factors for mortality (1-6). However, the etiologies and risks of patients with acute massive gastrointestinal bleeding are complex and often require a multi-specialty approach to treatment (7).
Early fluid resuscitation, rapid assessment of the rate and volume of blood loss, the appearance of the expelled blood, hypotension, presence of shock and coagulopathy are all important determinants of treatment strategy (7). After patient stabilization, endoscopy is often used to detect active bleeders and to achieve hemostasis; however, this primary hemostatic procedure has a 10-30% failure rate (8-10). If the patient still exhibits ongoing bleeding (> 1 mL/min) after endoscopy or if primary hemostasis cannot be achieved using endoscopic techniques, further aggressive treatment with intra-arterial embolization or surgical intervention is necessary.
Intra-arterial treatment is an alternative method for control of hemorrhage. When patients undergo angiography, the intra-arterial treatment strategy (coil embolization or vasopressin infusion) is usually based on visualization of contrast extravasation. Contrast extravasation on angiography is strong evidence of ongoing bleeding and may facilitate embolization of active bleeders (11-13). In our experience, if active extravasation of contrast material was identified on angiography, the target vessel was treated via superselective transarterial embolization. And, if active extravasation was not demonstrated by the angiographic procedure, the patient was treated by vasopressin infusion. By the two different ways of intra-arterial treatment, the angiographic sign of contrast extravasation may affect therapeutic strategy. In this study, we retrospectively compared the clinical characteristics, endoscopic findings, as well as the 30-day and 90-day mortality rates of acute massive gastrointestinal bleeding patients in who contrast extravasations were detected or not detected on angiography. The purpose of this retrospective study was to determine whether treatment outcome is associated with this angiographic sign.
MATERIALS AND METHODS
Patient Population
This study was conducted retrospectively at a tertiary referral medical centre from January 2007 to December 2009. The study was approved by the institutional review board for human investigation, and written informed consent was waived because of strict maintenance of patient anonymity and the observational nature of the study. A search of the institutional database for interventional radiology identified 92 consecutive patients who experienced a first attack of acute gastrointestinal bleeding after the failure of an endoscopic examination was referred for intra-arterial treatment. Patients with acute massive gastrointestinal bleeding who directly underwent surgery were not enrolled in the study. Endoscopic failure was defined as failure to detect the source of bleeding using endoscopy or failure to achieve primary hemostasis. Acute massive gastrointestinal bleeding was deemed to have occurred if either of the following two criteria was met: hemodynamic instability (hypotension with systolic blood pressure < 90 mmHg) during the angiographic procedure or transfusion of at least four units of blood within 24 hours of symptoms of acute bleeding. We excluded four patients because of a history of gastro-esophageal varices associated with liver cirrhosis or portal hypertensive gastropathy. Nine patients with stable vital signs during angiography who did not fulfill the aforementioned definition of acute massive gastrointestinal bleeding were also excluded. Thus, our study population consisted of 79 patients (M:F = 49:30; mean age, 68.4 years; range, 21-94 years).
The clinical manifestation and laboratory data of each patient were recorded after reviewing their medical charts. Data were collected on demographic characteristics, appearance of expelled blood, hemodynamic status, laboratory findings, co-morbidities, use of adjuvant therapy, endoscopic findings, angiographic interventions, rebleeding, and mortality. The possible cause of mortality was also recorded by reviewing the patient medical charts. Patients who met one of the following criteria were identified as having bleeding tendency: 1) international normalized ratio greater than 1.6, 2) partial thromboplastin time greater than 45 sec, or 3) thrombocytopenia with a platelet count less than 50,000 per cubic millimeter (5 × 1010 per liter). Missing or implausible data were identified and corrected after consultation with the patient's physician.
Angiography and Embolization Technique
In our interventional radiology section, all procedures were performed in a similar fashion by three interventional radiologists, whose experience ranged from 6 to 20 years. Continuous electrocardiographic and pulse oximetry cardiopulmonary monitoring were performed by a nurse throughout the procedure; if necessary, intravenous sedation was administered or intubation was performed by an anesthesiologist. At the commencement of angiography, a 5-Fr introducer was inserted into the common femoral artery under local anesthesia. The celiac trunk and superior mesenteric artery were routinely examined using a 4.1-Fr catheter (Cook Incorporated, Bloomington, IN). The inferior mesenteric artery and iliac arteries were selectively checked if there was suspected bleeding in the distal colon or rectum. If indicated, we used a 2.7-Fr microcatheter system (Terumo Corporation, Tokyo, Japan) to approach the target vessel. Iodinated contrast medium (Ultravist, Bayer Schering Pharma AG, Berlin, Germany; iodine content, 300 mg/mL) was used.
If active extravasation of contrast material was identified on angiography, the target vessel was treated via superselective transarterial embolization. The target vessels were embolized using metallic coils (and in some cases, coils supplemented with a Gelatin sponge) to the point of flow stasis. We used 0.035-inch stainless macrocoils (Cook Incorporated) or 0.018-inch platinum microcoils (Boston Scientific, Ireland) for embolization. The procedure was considered technically successful if there was complete occlusion of the target vessel. An example of successful treatment of active bleeding from the right colic artery is shown in Figure 1. If active extravasation was not demonstrated by the angiographic procedure, the patient was treated with intra-arterial administration of vasopressin for two days via a catheter extending to the suspected target vessel (most commonly the gastro-duodenal artery or the superior mesenteric artery). In such cases, the suspected target vessel was selected on the basis of clinical appearance of the patient and the appearance of the expelled blood on endoscopy. Vasopressin administration typically began with a loading dose of 0.2 U/min, which was then increased to a maximum of 0.4 U/min, followed by tapering of the dose over 12-24 hours.
Clinical Follow Up
A successful hemostasis was defined as the cessation of active bleeding and stabilization of the hemoglobin levels. Clinical success was defined as a patient surviving 90 days from this bleeding episode. The follow-up medical records were reviewed to determine whether the patients experienced ongoing blood loss and whether subsequent surgery or repeat angiographic procedures were required. After completion of the angiographic intervention, a rebleeding episode was defined as a subsequent bleeding episode with a drop in hemoglobin of 2 g/dL, that occurred after the initial bleed had stopped within 72 hours. The 30-day and 90-day mortality rates were recorded. We also checked whether the patient had further blood transfusions to replace ongoing blood loss, whether the patient required further intervention in the form of a repeat embolization or surgery to stop bleeding, and whether the patient died because of acute hemorrhage or hemorrhage-related complications.
Statistical Analysis
Statistical analyses were performed using SPSS version 14.0 (SPSS INC., IBM Company, Chicago, IL). Descriptive statistics are expressed as the mean ± standard deviation (SD) and range for continuous variables. Categorical variables are expressed as frequencies and percentages. A one-way ANOVA was used to compare the two groups of patients. A p value of < 0.05 was considered to be statistically significant. Survival was estimated using the Kaplan-Meier method. In order to find out the potential risk factors for 90-day mortality, a univariate logistic regression analysis was conducted with age, gender, presence of shock, number of blood transfusions, rebleeding, cormorbidities, time intervals between endoscopic failure to angiography, location of acute bleeding (upper or lower), treatment methods (coil embolization versus vasopressin infusion), successful hemostasis and laboratory values (including hemoglobin, creatinine, platelet counts, presence of metabolic acidosis and bleeding tendency) as factors. A multivariate analysis was conducted using the significant risk factors on the univariate analysis.
RESULTS
Clinical Variables between the Positive and Negative Extravasation Groups
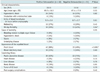
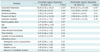
Our study population consisted of 79 patients. Forty-eight patients had detectable contrast extravasation (positive extravasation group), while 31 patients did not (negative extravasation group). The clinical characteristics; appearance of the expelled blood and coexisting illnesses in patients with acute massive gastrointestinal bleeding, are summarized in Table 1. All 79 patients were resuscitated in the intensive care unit or in the emergency ward. There were no significant differences in sex, age, incidence of hypovolemic shock or units of blood transfused 24 hours before angiography. Eleven patients (14%) were intubated before or during the angiographic procedure and a mean of 8.9 units of blood (range, 4-16 units) were administered 24 hours before the procedure. Mortality differed significantly between the positive and negative extravasation groups (20% and 42%, respectively; p < 0.05), but the rebleeding rate did not differ between the two groups. Bleeding-related multiple organ failure and hypovolemic shock were the most common causes of mortality in the both groups of patients. The appearance of the expelled blood was classed as fresh blood in 57 instances (n = 42 in positive extravasation group; and n = 15 in negative extravasation group; 88% versus 48%) and as clotted blood or melena in 15 instances. The incidence of blood expelled as fresh blood differed between the two groups (48% versus 88%, p < 0.05). The most common co-morbidity in the positive and negative extravasation groups was peptic ulcerative disease (n = 30 in positive extravasation group, n = 22 in negative extravasation group; 63% and 71%, respectively).
Estimated Endoscopic Etiologies, Adjuvant Therapy, and Intra-Arterial Treatment between the Positive and Negative Extravasation Groups
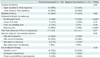
Table 2 shows a comparison of the estimated endoscopic etiologies, adjuvant therapy, and intra-arterial treatment between the two groups of patients. Upper gastrointestinal endoscopy was performed on all 79 patients. A bleeding ulcer was the most common endoscopic finding (31 of 48, 65%) in the positive extravasation group, compared with no detectable lesion (17 of 31, 55%) in the negative extravasation group. Of the endoscopic findings, the incidence of bleeding ulcers and the incidence of the absence of detectable lesions differed between the two groups (p < 0.01). Due to acute gastrointestinal bleeding, which is typically intermittent in nature, the endoscopic finding of non-bleeding ulcer found in the two groups did not show evidence of bleeding at the time of endoscopy, but they still presented symptoms of acute blood loss after endoscopic hemostasis. None of the patients underwent a push enteroscopy or balloon-assisted gastroscopy. Of the 79 patients, 24 (30%) also underwent a colonoscopy, which revealed a massive amount of fresh and old blood in the course of the colon. The mean time from endoscopic failure to angiography in the 79 patients was 8.3 hours (range, 60 min to 35 hr). In this study, patients with positive contrast extravasation (n = 48) all underwent a coil embolization in the selected bleeding artery, including 12 (25%) in gastro-duodenal artery, 25 (52%) in superior mesentery artery, eight (17%) in inferior mesentery artery, and three (6%) in iliac artery. In contrast; patients with negative contrast extravasation (n = 31) underwent an intra-arterial vasopressin infusion; nine (29%) in the gastro-duodenal artery, 18 (58%) in superior mesentery artery, and four (13%) in inferior mesentery artery. However, there is no statistical difference of these bleeding arteries between the two groups (p = 0.5). Fifty-eight patients (73%) received adjuvant therapy consisting of vitamins (n = 36), H2 blockers (n = 9), and proton pump inhibitors (n = 13).
Hemodynamic and Laboratory Characteristics between the Positive and Negative Extravasation Groups
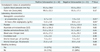
Table 3 lists hemodynamic and laboratory findings for the two groups of patients. Hemoglobin concentration was lower in the positive extravasation group than in the negative extravasation group (p < 0.05). After embolization, an elevation in hemoglobin level was observed in both the positive and negative extravasation groups, and was significantly greater in the positive extravasation group compared to the negative extravasation group (p < 0.05). There was no difference in hemodynamic status (systolic blood pressure or pulse rate) between the groups at presentation. The other laboratory data (platelet count, liver and renal function and arterial blood gas level) at presentation did not differ between the groups. Bleeding tendency showed no statistical difference between the two groups (n = 13 in positive extravasation, n = 10 in the negative extravasation group, and p = 0.62).
Follow-Up Studies and Short-Term Outcomes
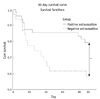
Fifty-six patients (n = 38 for the positive extravasation group, and n = 18 for the negative extravasation group; 79% versus 58%) survived from this bleeding episode. The overall clinical success rate was 71%. Moreover, the overall median time from endoscopic failure to angiography in the 79 patients was 6.4 hours (range, 60 min to 20 hr), and there was no significant difference in the time interval between the positive and negative extravasation groups (7.7 ± 6.6 versus 9.2 ± 5.1; p = 0.27). A successful hemostasis was recorded and showed no statistical difference between the two groups (n = 38 for the positive extravasation group, n = 20 for the negative extravasation group, and p > 0.05). In ten positive extravasation patients that experienced a failed coil embolization, seven underwent surgery, two underwent a second angiographic embolization and one refused a secondary intervention. In eleven negative extravasation patients without successful hemostasis, nine underwent surgery and two died without receiving any further intervention. Rebleeding rate also did not differ between the two groups (p = 0.43). At follow-up, 19 patients experienced rebleeding; six patients (6 of 31, 19%) in the negative extravasation group and 13 (13 of 48, 27%) in the positive extravasation group. Twenty-three patients (overall mortality, 29%) died within 90 days. The Kaplan-Meier technique showed there was no difference between the groups for 30-day mortality, but 90-day mortality was significantly higher in the negative extravasation group compared to the positive extravasation group (42% versus 20%, p < 0.05). The relative survival curves are presented in Figure 2. In the period of the 90th day to the one-year follow-up, we found that there was two additional patients in the positive extravasation group that died of sepsis and their underlying disease, and no additional patient in the negative extravasation died during this period.
Post-procedural complications included inguinal hematoma, bowel ischemia and acute renal failure. In the positive extravasation group, we found two inguinal hematomas, one bowel ischemia, and one acute renal failure; in the extravasation group, one inguinal hematoma and one acute renal failure. No bowel ischemia was noted in negative extravasation group.
A univariate and multivariate logistic regression analysis for the potential risk factors was listed in Table 4. The univariate analysis showed that successful hemostasis (odds ratio [OR] = 36.83; 90% CI: 9.3-146.2), presence of shock (OR = 3.51; 90% CI: 1.21-10.24), bleeding tendency (OR = 3.36; 90% CI: 1.19-9.49), rebleeding (OR = 2.96; 90% CI: 1.00-8.72), and treatment methods (OR = 2.74; 90% CI: 1.01-7.44) are significantly associated with mortality after intra-arterial treatment. For the multivariate analysis, we found that successful hemostasis (OR = 28.66; 90% CI: 6.53-125.68; p < 0.01) is the most important predictor affecting the mortality in the two groups of patients.
DISCUSSION
Our study revealed that successful therapeutic embolization is usually associated with visualization of contrast extravasation (20% mortality in the positive extravasation group versus 42% mortality in the negative extravasation group). An angiographic sign of contrast extravasation is a direct indication of a bleeding artery, and subsequent coil embolization is more effective in terminating acute massive gastrointestinal bleeding than intra-arterial vasopressin infusion therapy. We found that angiography with subsequent therapeutic embolization was successful in controlling hemorrhage in 56 (71%) of 79 patients. Although there is still controversy about the preferred bleeder localization and treatment method for patients experiencing acute life-threatening blood loss after endoscopic failure, it is always important to detect the bleeding artery as soon as possible to optimize treatment and decrease mortality (14). This may be achieved way of surgery or transarterial angiography (13). However, surgical interventions are invasive, may cause hypoxia in hemodynamically unstable patients, and require general anesthesia, which may cause cardiac arrhythmia, bronchospasm, and even sudden death. The advantages of angiography are that it is less invasive than surgery and often does not require general anesthesia. In addition, therapeutic embolization and intra-arterial vasopressin infusion can be performed during the procedure.
In clinical practice, it is assumed that the selection of intra-arterial treatment (coil embolization or vasopressin infusion) is usually based on visualization of contrast extravasation on angiography. Patients with positive contrast extravasation can be directly treated for a bleeding artery and undergo a guided coil embolization of the active bleeder. In patients who do not have angiographic signs of contrast extravasation (negative contrast extravasation), the catheter is often placed in the suspected target artery for intra-arterial vasopressin infusion therapy. In a retrospective study of 47 patients (15), Gomes et al. (15) compared the effectiveness of intra-arterial vasopressin infusion with that of transarterial embolization therapy in patients with acute major gastrointestinal hemorrhage. Contrast extravasation was noted in all of their patients on angiography, and the overall success rate with embolization therapy was significantly higher than that of intra-arterial vasopressin therapy (88% versus 52%, respectively). We saw similar results in our study. The clinical success rate was 79% in the positive extravasation group (treated with embolization) and 58% in the negative extravasation group (treated with vasopressin infusion). Although both a coil embolization and intra-arterial vasopressin infusion have a therapeutic effect on the control of acute gastrointestinal hemorrhage, Gomes et al. (15) concluded that a coil embolization offers several advantages over intra-arterial vasopressin infusion, including a more permanent and faster control of hemorrhage and lower mortality rate.
To our knowledge, there were only older scientific papers to evaluate the efficacy and safety of intra-arterial vasopressin infusion in patients with angiographic signs of acute gastrointestinal bleeding (16, 17). With modern transarterial embolization techniques, coil embolization has advantages over vasopressin infusion therapy in terms of quicker completion of therapy and decreased likelihood of systemic complications (18). However, in some difficult cases, especially when superselective catheterization is technically difficult to approach or for multiple bleeders, vasopressin is still preferable. It has been well known that mesenteric arterial constriction in response to vasopressin infusion may cause unfavorable complications (e.g. intestinal ischemia) (19, 20). Further clarification of the role of vasopressin infusion in patients with no angiographic sign of active bleeding requires prospective randomized controlled trials or meta-analyses.
Treatment of lesions that exhibit positive extravasation of contrast material using embolization reportedly has a high success rate, presumably because it targets the bleeding artery directly (13, 21-23). Padia et al. (24) evaluated the effectiveness of coil embolization in a large series of 108 patients with acute upper gastrointestinal hemorrhage, with or without contrast extravasation on angiography. In patients without contrast extravasation on angiography, Padia et al. (24) performed blind embolizations of the gastro-duodenal artery using coils. The treatment success rate and short-term outcome (30-day mortality) did not differ between the two groups, even though the negative extravasation group had a higher incidence of co-morbidity with respiratory compromise. Similarly, our results also showed that 30-day mortality was similar for the two groups; however, the 90-day mortality differed significantly between our two groups. We believe that, although both embolization methods can temporarily stop bleeding, coil embolization is better for permanent cessation of acute massive gastrointestinal bleeding than intra-arterial administration of vasopressin, and has a success rate similar to that of surgery.
Although we found that the rebleeding rate in negative extravasation group is lower than positive extravasation group, the short-term (90-days) and long-term (one-year) mortality rates are still higher in the negative extravasation group. When analysing the cause of death, patients with bleeding from an unknown origin may have a higher propensity die of hypovolemic shock or bleeding-related multiple organ failure during an acute episode of bleeding, and because of the difficulty in identifying the active bleeders, the mortality rate is higher than the positive extravasation group. Moreover, it was concluded that patients with negative bleeders on angiography died soon after without a timely hemostasis. We thought that the use of vasopressin infusion in the negative extravasation group could not effectively stop acute massive gastrointestinal bleeding in a timely manner (25). Based on our results, alternative methods such as early surgical intervention should be considered in patients with negative angiographic findings of contrast extravasation.
A variety of embolic agents such as Gelatin sponges, metallic coils, polyvinyl alcohol, glue, N-butyl cyanoacrylate (NBCA), and autologous blood clots have been used in embolization for acute gastrointestinal bleeding (6, 26-28). The choice of the embolic agent usually depends on the diameter of the bleeding artery and the expected duration of the embolic effect. In our institution, we implant coils as close as possible to the bleeding artery and supplement them with Gelatin sponges to prevent rebleeding from potential collaterals. Like most interventional radiologists, we are reluctant to use liquid adhesives such as glue and NBCA because of the potential risk of bowel ischemia and the difficulty of handling liquid adhesives, although Toyoda et al. (29) reported that transarterial embolization using NBCA is life-saving for urgent hemostases and is particularly useful in cases of acute massive gastrointestinal bleeding and coagulopathy.
Our study has several limitations. First, there was a selection bias in our study population. Patients with acute massive gastrointestinal bleeding who received surgery without prior angiographic intervention were not included in the study. Moreover, we only included patients who fulfilled with the definition of acute massive gastrointestinal bleeding, that is hemodynamic instability (hypotension with systolic blood pressure < 90 mmHg) during the angiographic procedure or transfusion of at least four units of blood within 24 hours of symptoms of acute bleeding, and directly underwent angiography. Besides, the optimal time to perform angiography is a difficult clinical decision. Beyond this definition of acute massive gastrointestinal bleeding, it may be difficult to identify a definite source of bleeding on angiography patients with minor gastrointestinal hemorrhage (30). Radiologists may hesitate to perform angiography, and in this study, we also do not perform an angiography in such cases. Second, visualization of contrast extravasation is sometimes not objective. In a few cases, subtle or equivocal contrast extravasation on angiography makes it difficult to assess whether a patient had ongoing bleeding or not. Third, this study was retrospective. Although criteria were applied for transarterial embolization, the use of coils and the number of Gelfoam pieces used were not standardized. The experience of the three radiologists differed. Fourth, only a small number of our patients underwent CT angiography, although this method now has been proven to provide useful diagnostic value in patients with acute massive gastrointestinal bleeding. However, for dealing with emergent acute blood loss, we believe that angiography with timely transarterial embolization offers a more important therapeutic role that CT angiography cannot achieve.
In this study, we noted that patients with active massive gastrointestinal bleeding after endoscopic failure are at high risk of dying. Intra-arterial treatment (coil embolization or vasopressin infusion) is an alternative method to achieve hemostasis. However, visualization of contrast extravasation on angiography can target the bleeding artery directly and guide the coil embolization of the active bleeder. Among the two groups of patients, our findings suggest that patients with positive contrast extravasation on angiography have a higher survival rate than patients with negative contrast extravasation.

 XML Download
XML Download