

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Brain function and activation is strongly correlated to blood supply and perfusion, respectively. These effects are known as neurovascular coupling (1). On the other hand, the cerebral blood flow (CBF) is altered in tumors (2) or in ischemic areas (3). Several approaches have been developed in the past for measuring regional cerebral blood flow (rCBF): positron emission tomography (PET), single photon emission computed tomography (SPECT), Xenon-enhanced computed tomography (XeCT), dynamic perfusion-computed tomography (PCT), contrast-enhanced MRI, and dynamic susceptibility contrast (DSC)-MRI highlight these methods. Those techniques use contrast agents and are therefore not completely non-invasive (4, 5), while Doppler ultrasound shows the limitations of the applicability in an intra-cerebral areas.
Arterial spin labeling (ASL) is a completely noninvasive technique for perfusion assessment using MRI. ASL techniques apply endogenous arterial water as tracer. The method consists of a preparation part and a data acquisition part. A commonly used preparation technique is the flow-sensitive alternating inversion recovery (FAIR) method (6, 7).
The most common image acquisition technique for ASL is echo planar imaging (EPI) (6-8), which is, unfortunately, highly sensitive to susceptibility artifacts occurring especially in areas with pronounced susceptibility differences such as the skull base.
An alternative image acquisition technique for ASL is the "true fast imaging in steady precession" (TrueFISP) sequence. This method is much less sensitive to susceptibility artifacts than EPI and delivers especially high image quality in areas prone to susceptibility effects such as the brain stem or other areas aside from the skull base. Boss et al. (9) compared the FAIR-TrueFISP sequence with the EPI method and found relevant differences in image quality.
Due to marked differences in susceptibility near the skull base with bone structures on one hand and air filled areas (sinus) on the other hand, CBF measures of the amygdala and hippocampus are technically challenging.
Especially, the amygdala, hippocampus, and rhinonasal cortex are highly involved in the etiopathology of dementia (10). The aim of this study was the application of the FAIR-TrueFISP method for quantitative determination of CBF in the amygdala/rhinonasal cortex bilaterally, and the brain stem (pons) (for comparison). Those techniques were applied in a clinical routine setup and the results were to be compared with perfusion data in the literature, and measured using different methodical approaches.
Go to : 
MATERIALS AND METHODS
Subjects
The study was approved by the local ethics committee. The volunteers of this study were patients of our department, which underwent an MRI for different reasons. Twenty- three subjects participated after giving informed consent. All participants had no incidence for mental impairment like dementia or affections of structures at the basal brain. The cohort consisted of seven men and 16 women, with an age range of 39 to 84 years and a mean of 60 ± 13 years.
MR Scanner
The investigations were performed using a clinical 1.5 Tesla whole-body MR scanner (Magnetom Sonata, Siemens Healthcare, Erlangen, Germany). The body coil was used for homogeneous radiofrequency (RF) transmission, while the 8-channel head-coil was used for signal detection. The gradient system operates with a maximum gradient strength of 40 mT/m and a slew rate of 200 T/m/s.
Anatomical FLAIR Imaging
T2-weighted anatomical images of the whole brain were recorded by means of a FLAIR (fluid attenuated inversion recovery)-sequence. The slab was oriented in the axial standard orientation along the crus anterior and posterior of the corpus callosum.
FAIR True-FISP Imaging
The amygdala was located in the FLAIR images and the selected slice for ASL imaging was oriented in the same way. So, the amygdala and rhinonasal cortex, as well as parts of the brain stem (pons), were covered by one image.
The FAIR-TrueFISP method has been previously described (11); in the FAIR preparation scheme, an adiabatic RF FOCI (frequency offset corrected inversion) pulse was used for slice selective inversion. A inversion time (TI) of 1.2 sec after the inversion pulse was chosen prior to each acquisition, and four FAIR preparation prescans were applied before data acquisition. Imaging slice thickness was 5 mm and inversion slab thickness for slice selective inversion was 12.5 mm. Image matrix size for perfusion images and T1 maps was 64 × 64 with a field of view of 256 × 256 mm, resulting in a spatial resolution of 4 × 4 × 5 mm. To reduce Gibbs ringing, a Hamming k-space filter was applied. For optimal perfusion contrast, a centric-reordered k-space acquisition scheme was used.
Each FAIR preparation was followed by a data recording of one slice. Repetition time was 4.8 ms, echo time was 2.4 ms, and acquisition bandwidth of the TrueFISP sequence was 651 Hz/pixel. Acquisition time for 50 sets of FAIR images was 6:56 min. Fat-saturation preparation and an excitation angle of 70° was applied. After FAIR-TrueFISP perfusion imaging, tissue equilibrium magnetization was measured by the acquisition of a conventional TrueFISP image using the mentioned parameters (without inversion pulse).
Image Processing and Data Analysis
Magnitude images with slice selective and global inversion were collected in two sets. Magnitude images of each set were averaged and the final images were subtracted on a standalone PC using a home-made Matlab (The Mathworks, Inc., Natick, MA) program. The quantitative perfusion maps were computed on a pixel-by-pixel basis from the analysis of the magnetization difference, ΔM, using Eq. [1] (6):

where M0 represents the tissue equilibrium magnetization per unit mass of the tissue, T1 is the longitudinal relaxation time of tissue, f is the perfusion rate (usually in mL/100 g/minute), and λ is the blood-tissue water partition coefficient, which is assumed to have a constant value of 90 mL/100 g/minute (12). The T1 value for the amygdala and arterial blood was set to 1.2 s. All pixels with perfusion values greater than 150 mL/100 g/minute were encoded to 0 mL/100 g/minute, since they represent vascular flow rather than tissue perfusion.
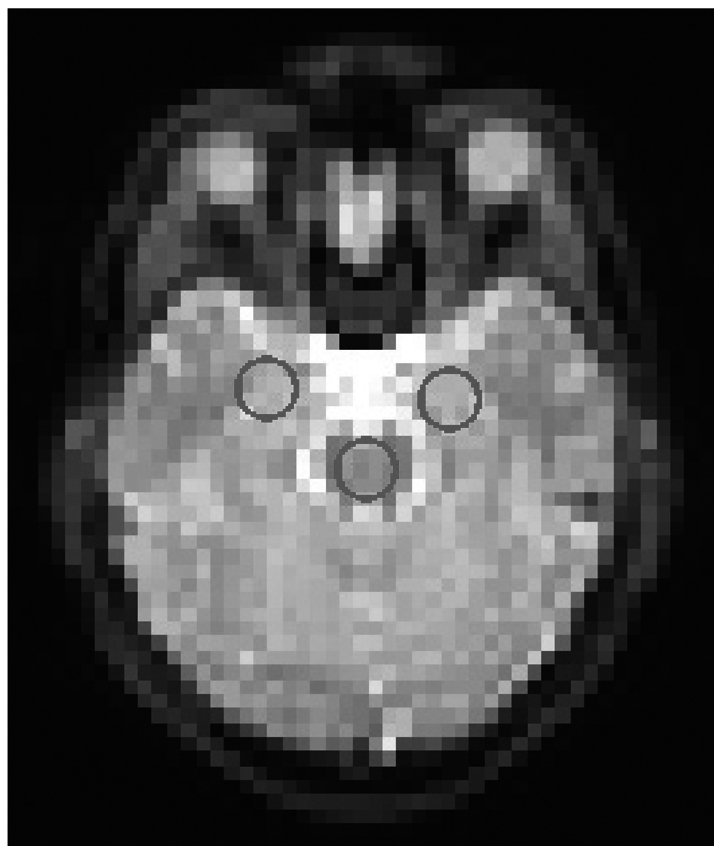
Three regions of interest (ROI) were defined: one in the pons, one in the left and one in the right amygdala. Figure 1 illustrates the localizations in a FLAIR image. Data were furthermore processed an analysed using OpenOffice (Calculator).
Go to :
RESULTS
Reproducibility
One volunteer was investigated three times in one session with repositioning between the different experiments. After anatomical FLAIR Imaging the ASL experiments were planned in plane with the FLAIR images. Reliability measures were performed defining the above mentioned ROIs in the amygdala left and right and in the pons. The data revealed a standard deviation of 12% of mean in the pons and 5% and 8% in the right and left amygdala. Data are given in Table 1.

Perfusion Data
Following perfusion values were derived: amygdala right 65.2 (± 18.2) mL/100 g/minute, amygdala left 64.6 (± 21.0) mL/100 g/minute, pons 74.4 (± 19.3) mL/100 g/minute.
Table 2 illustrates the results of our study and compares them with selected former published data in the literature. Compared with PET measurements the values are a little higher but comparable. Other ASL experiments using continuous ASL with EPI acquisition revealed much lower values. Standard deviations are relatively high, but this has also been reported from PET measurements (13, 14).
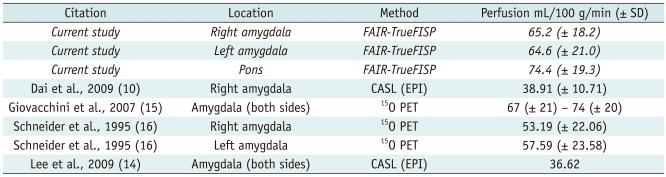
Table 2
Published Perfusion Data in the Literature
Note.- Data from previously published literature with absolute perfusion data at skull base, especially in amygdala and brain stem. 15O PET = oxygen-15 positron emission tomography, CASL = continuous arterial spin labeling, EPI = echo planar imaging, FAIR-TrueFISP = flow-sensitive alternating inversion recovery-true fast imaging in steady precession
![]()
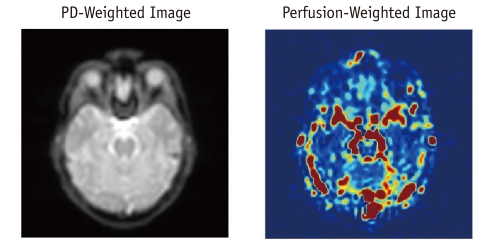
Figure 2 shows a proton density weighted TrueFISP image and a perfusion weighted image of one individual for illustration.
Go to :
DISCUSSION
In this study we applied the FAIR-True FISP technique in order to determine perfusion data in the amygdala with a completely non-invasive MRI technique. Most common approaches use EPI data acquisition to measure perfusion in the brain. This technique is much more sensitive to susceptibility artifacts than the True-FISP technique. Boss et al. (9) have shown that FAIR-TrueFISP is applicable at the skull base. The FAIR-TrueFISP imaging technique uses endogenous water as a tracer. Therefore it is a completely non-invasive method.
Scent impairment is one of the early symptoms in mild cognitive impairment (MCI), which is the early stage of dementia (13). Therefore structures of the rhino-nasal cortex and the amygdala seem to be strongly involved in the development of dementia. Hence, functional investigation of these structures is of great concern in the diagnosis of dementia, especially in early stages. In this study we employed this method to determine perfusion values in the amygdala in mentally healthy people. The acquired values were compared with published values from the literature.
Compared with Dai et al. (10) and Lee et al. (14) (Tables 1, 2) who used continuous ASL for measuring perfusion, our values are much higher. But compared to PET-measures, which use radioactive labeled water (15O) (15, 16), our values are very similar to the literature. However, the standard deviation of individual data is pronounced.
Thus, FAIR-True FISP has some advantages but also disadvantages. Compared to EPI, it is feasible to investigate brain structures in the vicinity to the skull base, because it is less sensitive to susceptibility changes. Second, it is feasible in the clinical routine as one doesn't need any additional technical equipment like continuous arterial spin labeling (CASL). Third, it is non invasive because it uses endogenous water as tracer, and one doesn't need any contrast agent. However, there are some disadvantages to be discussed. FAIR TrueFISP is very sensitive to water inflow effects. Therefore small vessels in the voxel of interest contribute to the perfusion signal and may therefore increase the CBF values artificially. This effect was already discussed by Boss et al. (9). And in our study, this feature may be of special importance due to many also small vessels at the skull base. This effect explains the higher values compared to the other CASL studies. On the other hand, the present values are comparable with the PET data from literature. PET is still meant to be the gold standard in perfusion measures. So our measures are probably nearer to reality than the published CASL measures. Both, the present data, and also the formerly published data concerning the amygdale, showed very high amounts of variance. Standard deviations are very high in all cases (Table 2). Thus FAIR-TrueFISP is not worse than other more elaborated methods.
Another shortcoming of the present study is a wide range of age in the study samples. Due to a small sample size, we did not correct the data for age. But in elderly people lower perfusion values would be expected than in younger persons, independent from dementia (17). Therefore, to consolidate the results, and to analyse correlations with age, further studies will be necessary.
Further studies will also be necessary to investigate the clinical value of FAIR-True-FISP in functional perfusion studies. But it seems to be a dedicated method for the use at the skull base.
Go to :
 XML Download
XML Download