

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
High-resolution CT (HRCT) is known to be useful for determining the extent of diffuse interstitial lung disease (DILD), especially idiopathic interstitial pneumonias (1-3). In addition, HRCT is useful for predicting the clinical outcomes of idiopathic pulmonary fibrosis (IPF) as the HRCT scoring of fibrosis correlates well with the mortality rate (4, 5). However, in most cases, the disease extent seen on HRCT has been subjectively and qualitatively evaluated by radiologists who analyze a medical image by searching for specific disease patterns. Typically, a correct global diagnosis of parenchymal lung disease can only be made 40-70% of the time and by two experienced readers on 76-85% of the global diagnoses (2, 6). Such variation has been confirmed in other studies examining lung pattern type, with an interobserver variation of 81% (kappa of 0.48) and a similar intraobserver variation (kappa of 0.37 to 0.78) (7). Other visual scoring system have been suggested by Remy-Jardin et al. (8) or Copley et al. (9). However, in their studies, the reproducibility of the scoring systems was not assessed and their scoring systems were semi-quantitative methods. Therefore, an automated classification system is necessary for objective and reproducible assessment of disease extent.
To objectively evaluate the extent of IPF, several automated classification systems have been developed based on the specific features of texture or shape such as a histogram, gradient, run-length matrix, Top-hat transformation and so on, as seen on HRCT images (10-15). We developed an automated classification and quantification system for chronic obstructive pulmonary disease and DILD using HRCT images (5, 16). We thought that the basic algorithm of these studies can be applied for a quantitative assessment of HRCT in patients with usual interstitial pneumonia (UIP) and nonspecific interstitial pneumonia (NSIP). The purposes of this study are to evaluate the usefulness of quantifying UIP and NSIP in terms of the agreement with the radiologist's interpretation, the contribution of regional patterns to pulmonary function test (PFT) variables, and the ability to discriminate between UIP and NSIP.
MATERIALS AND METHODS
Our study was approved by the Asan Medical Center Institutional Review Board for Human Investigation and informed consent was not required because of the retrospective nature of our study.
Patients
Between May 1998 and August 2007, we reviewed the HRCT images of 834 patients that had interstitial lung diseases as well as 652 patients that had visible UIP or NSIP patterns on images. We assigned an UIP pattern for predominantly basal and peripheral reticular opacities with honeycombing, traction bronchiectasis on HRCT images, and a NSIP pattern for predominantly basal ground-glass opacities rather than reticular opacities. Of the 652 patients with UIP or NSIP patterns on images, 286 underwent surgical lung biopsies including video-assisted thoracoscopic surgery, open lung biopsy, and a lobectomy. Further, 195 patients had UIP or NSIP on HRCT images and pathologic specimens. Of these 195 patients, 83 underwent PFT. Several previous studies noted that texture-based quantification was largely dependent on training data sets (10, 13, 17, 18). Therefore, we decided to include patients with CT images from the same type of CT scanner (i.e., a 16-channel multi-detector CT - Sensation 16, Siemens, Forchheim, Germany). Among the patients who underwent PFT, 54 underwent HRCT scans using the same Siemens CT scanner.
Consequently, a total of 54 patients (M:F = 27:27; mean age, 52 years ± 9.7 standard deviation [SD]) were included in our study. Twenty-six patients (M:F = 18:8; mean age, 55 years ± 9.9 SD) had pathologically proven UIP, and 28 patients (M:F = 9:19; mean age, 53 years ± 9.7 SD) had pathologically proven NSIP. All patients had incremental HRCT scans using 0.75-mm collimation, 1-mm slice thickness, 10-mm intervals and a sharp kernel (B70f) on a 16-channel multi-detector CT (Sensation 16; Siemens, Forchheim, Germany). The matrix size was 512 × 512 and the window settings were center, -750 and width, 1500, respectively.
Automatic Classification System
We developed the automatic classification system using Visual C++ and the Insight ToolKit (ITK). Lung segmentation was performed automatically, and inaccurate segmentation was modified by one resident radiologist. Histogram, gradient features, run-length encoding, Grey Level Co-occurrence Matrix (GLCM), and ITK-GLCM, were used as texture features. For shape analysis, the size and number of low attenuation areas and means with standard deviations of white and black Top-Hat transformations of the original images were used. The detailed information of each feature was reported in previous papers (5, 19, 20).
To train and test the automated system, HRCT images were selected retrospectively from a total of 106 patients, which were included in another previous study group (16), which included 14 healthy subjects, 16 patients with emphysema, 35 patients with cryptogenic organizing pneumonia, 36 patients with usual interstitial pneumonia, four patients with pneumonia, and one patient with acute interstitial pneumonia. A thoracic radiologist with 10 years of clinical experience evaluated a total of 600 typical regions of interest (ROIs) (circular ROIs of 32-pixel diameter) by the naked eye and marked them as normal (NL, n = 100), ground-glass opacity (GGO, n = 100), reticular opacity (RO, n = 100), honeycombing (HC, n = 100), emphysema (EMPH, n = 100) or consolidation (CONS, n = 100). We chose several axial HRCT images from each patient to select typical ROIs. However, in order to minimize any clustering effect, we tried to select only one ROI in each image. If the same disease pattern of ROIs were selected from one patient, the ROIs were chosen from different lung lobes.
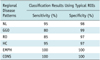
With 600 ROIs selected to represent typical areas of local disease patterns, the system was trained using the Support Vector Machine (SVM) classifier and the image features were subsequently extracted. The classifier performance was tested using a 5-fold cross-validation method. This was achieved by first randomly classifying data into five sets and then using four data sets for model construction and retaining one data sets to test the performance of the model. The performance testing was repeated 20 times, after which the results were averaged to assess the sensitivity and specificity of the system for classifying regional disease patterns.
Automatic Quantification
The trained system was applied to HRCT images of the whole lung in each patient with UIP or NSIP. For quantification of the regional patterns, round ROIs with a 10-pixel diameter were used. Analysis of the lung parenchyma was performed using an automatically moving-ROI function running through the lung field. Even if we marked a ROI of a typical disease pattern with the naked eye, several disease patterns can be exist microscopically. Therefore, instead of each ROI, each pixel was classified into one of six categories. Area and volume fractions of each class were also calculated. Volume was calculated simply by multiplying the area of each class by the slice thickness of the HRCT image.
Comparison with Human Readers
To assess the agreement of these quantification data of the system with those of human readers, we randomly selected 26 HRCT scans (13 HRCT scans from UIP and 13 HRCT scans from NSIP), and two thoracic radiologists with three and 11 years of experience with HRCT interpretation, respectively, were requested to record the extent of pulmonary abnormality. The extent of GGO, RO, HC, EMPH, and CONS was scored to the nearest 5% throughout the entire lung in each patient. The normal lung parenchyma was calculated simply by extracting the abnormality volume from the entire lung volume. All statistical analyses were performed using a statistical package (SPSS 15.0.0; SPSS; Chicago, IL). Results were expressed as mean ± SD. The interclass correlation coefficient (ICC) was used to evaluate the quantification agreement between the system and the readers. The comparison between the system and the readers was performed in terms of the volume fraction of each pattern. Values of the ICC were interpreted as k-statistics: slight (ICC 0-0.20), fair (ICC 0.21-0.40), moderate (ICC 0.41-0.60), substantial (ICC 0.61-0.80), or almost perfect (ICC 0.81-1).
Correlation Study between Pulmonary Function Test and Automated Quantification
Spirometry was performed as recommended by the American Thoracic Society (Vmax 22, SensorMedics, CA; PFDX, MedGraphics, MN) in all 54 patients (21). The following values were evaluated: the forced expiratory volume during one second (FEV1); and the forced vital capacity (FVC). The diffusing capacity (DLco) was measured according to the single-breath carbon monoxide uptake (Vmax 22, SensorMedics, CA; PFDX, MedGraphics, MN) (22). All values were expressed both as a percentage of measured to predicted values and as measured values. A linear regression analysis (LRA) with backward elimination was used to evaluate the contribution of regional patterns (NL, GGO, RO, HC, EMPH, and CONS) to the PFT parameters (FEV1, FVC, and DLco). This analysis was performed using a volume of each pattern and a measured value of the PFT parameter.
Discrimination between Usual Interstitial Pneumonia and Nonspecific Interstitial Pneumonia
The discriminating ability of the automated system between UIP and NSIP was evaluated using a binary (or binomial) logistic regression. The best set of regional patterns for differentiating between UIP and NSIP was found by trial and error. A p-value less than 0.05 was considered to be statistically significant. The analysis was performed according to the volume fraction of each pattern.
To test the performance of the human reader in the same data sets, a thoracic radiologist with 11-years of experience was requested to review the whole 54 HRCT scans and decide the likelihood of diagnosis. The characteristic HRCT findings in UIP are predominantly basal and peripheral reticular opacities with honeycombing and traction bronchiectasis. In NSIP, basal ground-glass opacities tend to predominate over reticular opacities, with traction bronchiectasis present only in advanced disease (23). According to these criteria, the probability of UIP or NSIP in each patient was estimated using a five-point rating scale: 1, definite NSIP; 2, probably NSIP; 3, possible UIP; 4, probable UIP; and 5, definite UIP.
RESULTS
Texture- and shape-based quantification was successfully performed on all images, and the quantification results were displayed using color-coded overlays of the original DICOM images (Figs. 1, 2, 3).
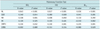
For an abnormal lung volume fraction (GGO, RO, HC, EMPH, and CONS), the overall ICC value showed almost perfect agreement (0.895) among the quantification results of the automated system and the two radiologists (Table 2) and, considering only the volume fraction of fibrosis (RO and HC), the overall ICC value also showed substantial agreement (0.706) among the automated system and the two radiologists. The overall ICC values for each regional pattern were almost in perfect agreement (0.895) for NL, substantial agreement (0.625) for GGO, substantial agreement (0.626) for RO, almost perfect agreement (0.893) for HC, substantial agreement (0.800) for EMPH, and moderate agreement (0.430) for CONS. The agreement between the two readers was almost perfect except for CONS in which there was substantial agreement. The agreement between the system and readers 1 or 2 was lower than that between the two readers, particularly for GGO, RO, and CONS.
In LRA (Table 3), the volumes of NL, GGO, RO, and EMPH significantly contributed to FEV1 (r = 0.72, β values, 0.84, 0.34, 0.34 and 0.24, respectively) and FVC (r = 0.76, β values, 0.82, 0.28, 0.21 and 0.34, respectively). And although the volume of NL contributed positively to the DLco, the volume of HC contributed negatively (r = 0.65, β values, 0.64, -0.21, respectively).
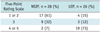
In 26 patients with UIPs, the reader gave a five-point rating scale as 1 or 2 in four patients (15%), 3 in three patients (12%), and 4 or 5 in 19 patients (73%) (Table 4). In 28 patients with NSIPs, the reader gave a five-point rating scale as 1 or 2 in 17 patients (61%), 3 in nine patients (32%), and 4 or 5 in two patients (7%) (Table 4). Among the 12 patients with a five-point rating scale of 3, there were three UIPs and nine NSIPs. Excluding scale 3, the diagnostic accuracy of the human reader for discriminating between UIP and NSIP was 67%.
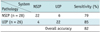
By either binomial or binary logistic regression, our system showed a discrimination power of 82% between UIP and NSIP (Table 5). This discriminative accuracy was much higher than that of the human reader. And when the human reader had difficulty arriving at the diagnosis between UIP and NSIP, as in the 12 patients with a five-point rating scale of 3, the system correctly classified nine patients (75% accuracy). The logistic prediction equation was:
ln(prob(event)/[1-prob(event)]) = 0.404 HC + 0.178 GGO + 0.181 RO - 0.010 HC × RO - 0.006 GGO × RO - 0.064 CONS × GGO - 4.347
where, prob(event) < 0.50 was NSIP and prob(event) ≥ 0.50 was UIP.
DISCUSSION
Our results showed that the automated system had reliable agreement with the radiologist's interpretation and that several regional patterns contributed to the PFT parameters. Unlike the previous quantification system of UIP using only the density and texture features (10, 11, 13-15, 24), we used shape features as well as the density and texture features to perform objective quantification of UIP and NSIP. The SVM classifier afforded highly sensitive and specific discrimination of the six typical, radiologic tissue types (Table 1). The results of this study are similar to or better than those of previous studies (7, 9). Even more importantly, our system can discriminate between UIP and NSIP with an 82% accuracy, which was superior to that of the human reader. To the best of our knowledge, there has been no previous report pertaining to the automated discrimination between UIP and NSIP.
There are several studies existing, which highlight the density histograms for the quantification of UIP (10, 11, 15, 24). And Do et al. (24) reported that a density histogram may be helpful for differentiating NSIP from UIP, without the definite presence of HC. Therefore, the system based on histograms had been used more extensively than the multiple feature method for the quantification of UIP. However, Uppaluri et al. (17) showed that the overall accuracy of the adaptive multiple feature method (AMFM) as 81%, which was 25% more successful than the histogram analysis. Uppaluri et al. (17) also showed that the samples comparing NL and the IPF samples had a discriminatory accuracy of 86% using the AMFM. Delorme et al. (13) developed a texture-based pattern recognition and segmentation for the quantification of HRCT findings in UIP. The overall accuracy of their study was 71%; however, they did not include HC, which is an important component of UIP. Rodriguez et al. (14) also showed that the automatic discrimination and quantification of IPF from normal lung parenchyma was possible using generalized fractal dimensions on HRCT images. However, they did not attempt to differentiate between UIP and NSIP, which is important for the treatment option and the patient prognosis. We demonstrated that our system had good agreement for determining the fibrosis extent between the system and the human reader, as well as a discriminating power of 82% between UIP and NSIP. Furthermore, when the human reader had difficulty distinguishing between UIP and NSIP, the system classified it correctly with an accuracy of 75%. In the logistic prediction equation of our system, HC was the largest component for discriminating between UIP and NSIP. GGO and RO also contributed to the power of discrimination.
Delorme et al. (13) showed that the identification of small anatomic structures such as vessels and bronchi was difficult and, our system similarly misclassified some normal vessels and bronchi as reticular opacity, ground-glass opacity, or honeycombing. The basic logic used to differentiate disease patterns may differ between the system and human readers. The system was trained using ROIs representing typical disease patterns. In addition, the best combination of features and parameter settings was selected by the classifier to most effectively discriminate typical areas. However, on clinical HRCT images of DILD, many lung areas do not have such typical compositions as there are always transitional zones between disease patterns, where an area can develop from one class to another as the disease progresses. Therefore, there is no clear method to discriminate among such borderline patterns. This fundamental problem may be overcome or minimized by adjusting the system using ROIs of normal vessels and relatively atypical or borderline patterns. Therefore, the quantification result of our system will be further improved if we include normal bronchovascular bundles and borderline patterns in our training data sets.
Our study showed that the volumes of the NL, GGO, RO, and EMPH contributed to FEV1 (r = 0.72, β values, 0.84, 0.34, 0.34 and 0.24, respectively) and FVC (r = 0.76, β values, 0.82, 0.28, 0.21 and 0.34, respectively). For DLco, the volumes of the NL and HC were independent contributors in opposite directions (r = 0.65, β values, 0.64, -0.21, respectively). This result indicated that the functional components of the lung, such as NL, had the greatest influence on FEV1 and FVC. HC corresponds to end-stage lung disease, and GGO reflects disease activity (25, 26). RO represents the disease spectrum between GGO and HC. In this context, our results showed that GGO and RO had a greater influence on FEV1 and FVC than did HC. On DLco, normal lung parenchyma was positively influenced, although the influence of HC was negative. These study results were well correlated with our previous knowledge.
Idiopathic pulmonary fibrosis is the most common idiopathic interstitial pneumonias (IIPs). With a median survival period ranging from two to four years, IPF has a substantially poorer prognosis than other IIPs (27, 28). NSIP is less common than UIP, but is still one of the most common histologic findings in patients with IIPs (29). As NSIP is associated with a variety of imaging and histologic findings, the diagnostic approach is highly challenging. However, the distinction between NSIP and UIP is more than academic, given the greater response to corticosteroids seen in a subgroup of patients with NSIP (30, 31). Especially, UIP with HC have a worse prognosis than NSIP or UIP without HC (26). Therefore, it is important to differentiate between NSIP and UIP for the purpose of determining both the treatment and the prognosis. Our system had good agreement in determining the fibrosis extent between the system and the human reader and a discriminating power of 82% between UIP and NSIP. Furthermore, when the human reader had difficulty determining the diagnosis between UIP and NSIP, the system classified it correctly with an accuracy of 75%. As we used only clinic-radiologic-pathologically proven cases, the results of the human reader might be lower than those of a clinician. Despite these factors, the system showed very good discriminating ability between UIP and NSIP, by combining the quantification results of several regional patterns. If we added additional information such as the distribution of the regional patterns throughout the entire lung, it may be possible to provide a second opinion provided by the system, for differentiating UIP from NSIP.
There are several limitations to this study. First, we included only pathologically proven UIPs and NSIPs. As a general rule, a pathologic specimen is obtained when there is difficulty differentiating between UIP and NSIP on HRCT images. Therefore, it was possible that we included many atypical cases in our study. In this case, our correlation results between PFT parameters and regional patterns may differ from those of typical UIP and NSIP cases. There is also a limitation derived from the nature of the automatic classification system. Texture-based quantification is largely dependent on the training data sets (10, 13, 17, 18). To simplify our task, we used CT images from a single machine (a Siemens scanner). However, applying this system to images from other CT scanners may yield unreliable results as the texture and shape features may be sensitive to the noise patterns and machine resolution of each individual scanner. Therefore, further system development which is less influenced by machines or noise patterns created by testing as well as comparison of various scanners will be necessary. Third, we used a sample of typical ROIs selected among images from the population of patients included into the study. This may induce a selection bias. Finally, agreement between the system and the two readers was evaluated in only 26 randomly selected cases. Therefore, this aspect will require further study, including more cases.
In conclusion, the quantification results of the automated system on HRCT images of UIP and NSIP, showed good agreement with those of the radiologist's interpretation, and several regional disease patterns contributed to the PFT variables. The system was able to successfully discriminate UIP from NSIP. Therefore, it may be used for the objective and reproducible assessment of regional disease severity in cases of UIP and NSIP.




 XML Download
XML Download