

 PDF
PDF ePub
ePub Citation
Citation Print
Print


To diagnose occult fractures in skeletally immature children, radiography is often insufficient because a subtle fracture is obscured by overlapping structures and by non-perpendicular X-ray beams to the fracture line. Also, it is difficult to interpret radiographs as to whether a fracture is present or not; especially in the joint regions where growing bones are composed of unmineralized physis and cartilaginous ossification centers (1-4). Fractures account for 71% of the delayed diagnoses in pediatric trauma, with the extremities having the most common involvement (5). In contrast to trauma in adults, the evaluation of a pediatric patient is often confounded by the patient's inability to participate in the history and physical examination (1-3, 5). In these situations, performing ultrasound (US) is helpful for the early diagnosis of both soft tissue and bone injuries, resulting in appropriate and timely management. The high reflectivity of US at the interface between the cortical bone and peri-osseous soft tissues can delineate the bone cortical outline and adjacent soft tissue changes at a fractured site (4, 6). US can be performed in young children without sedation, which is frequently required for MRI to prevent a motion artifact. There are reports about US diagnosis of occult fractures in children. To the best of our knowledge, most case reports in the English literature have a limited number of patients in a localized region of extremities (7-14). Accordingly, the purpose of this study is to describe US findings of occult fractures in growing bones of pediatric-aged children and report its usefulness in diagnosing fractures.
MATERIALS AND METHODS
Patient Selection
The study protocol was approved by the committee of the institutional review board of institutes. For six years (from April 2002 to March 2008), three authors (who had longer than seven years experience of musculoskeletal US) independently performed US in 50 children younger than 15 years who were referred with trauma-related local pain and swelling of the extremities. Among the 50 children, 11 did not have available clinical follow-up medical records and were excluded from the study. Another 14 children were excluded because they were not diagnosed as having a fracture (soft tissue contusion, seven cases; osteomyelitis, three cases; joint effusion, two cases; and foreign body, two cases).
The final enrollment of our study consisted of 25 fractures in 25 children (M:F = 20:5; age range: five months to 15 years; average age: 7.7 years) with a confirmed occult fracture by an initial and follow-up radiography, additional imaging studies, and clinical observation longer than three weeks. Of the 25 confirmed cases, additional MRIs (n = 11) and a radionuclide scan (n = 1) were performed on either the same day or within two days from the US examination (2 to 40 hours; mean: 26 hours). The symptom duration at US examination and time interval between the initial radiograph and US ranged from 30 minutes to two weeks (average: 7 days) (Table 1).
Ultrasound Machines and Scanning Methods
US was carried out with 5-10 MHz (HDI 3000, Advanced Technology Laboratories, Bothell, WA) and 7-12 MHz (HDI 5000, and iU22, Philips, Bothell, WA) broad-band linear array transducers. As a routine US examination, soft tissue, bones, and adjacent joints were examined in the long-axis (aligned of bone) and short-axis (transverse) directions in the area of discomfort. In addition, the opposite area asymptomatic contralateral extremity was examined for comparison.
Treatment Methods
Of the 25 confirmed occult fracture cases, five were treated by surgical intervention (one by open surgery, and four by percutaneous pinning), 14 were treated by casting immobilization, and the remaining six cases, by conservation. Conservative treatment was selected for the four ischial tuberosity fractures (case no. 11-14) and the two infant cases of femoral pathologic fractures (case no. 15, 16).
Review of Radiographs and Medical Records, and Classification of US Findings of Fractures
One author, who did not perform any US examination and was blinded to the final diagnoses, retrospectively reviewed all the radiograms, which were randomly numbered. He also analyzed carbon-copied medical records (clinical history, treatment methods, US findings with impression on US reports) which were also randomly numbered. Next, all the data was pigeonholed into editing tables (Tables 1, 2) according to the fracture sites (from the shoulder to the ankle) and age of the children.
RESULTS
Location of Fractures
The most common occult fracture sites were the elbow (n = 9, 36%), followed by the knee (n = 7, 28%), ischium (n = 4, 16%), distal fibula (n = 3, 12%), proximal femur (n = 1, 4%), and humeral shaft (n = 1, 4%). For the elbow (n = 9), fractures were found in the growth plate (n = 4), metaphysis (n = 2), medial epicondyle of the distal humerus (n = 2), as well as the olecranon tip of the ulna (n = 1) (Fig. 1). For the knee, fractures were found in the proximal tibia (n = 3), distal femur (n = 2), and patella (n = 2) (Table 1).
Clinical and Radiographic Findings
History of trauma was unclear in six cases, and most of these cases were of very young children. The provided clinical information prior to US, indicated that infection was observed in four cases (case no. 5, 7, 21, and 25 in Table 1). Following US, two cases were confirmed to be infections and the other two were found to bew fractures (Table 2). Three cases (case no. 12-14) referred with bone or soft tissue tumor before US indicated a 'fracture or infection' by the impression on the US reports. These included three pathologic fractures: (case no. 1, simple bone cyst of the humerus; and case no. 15 and 16, fractures around the knee in infants with prematurity history) (Tables 1, 2) (Fig. 2).
Thirteen out of the 25 cases showed no bone abnormalities except for various soft tissue swelling. In three of the 13 cases (case no. 9, 17, and 19), a tiny bone fragment of fracture was detected in an additional view obtained at a different axis (Fig. 3). In three children (case no. 1, 18, and 22), the radiography performed after the suggestion of a fracture by US results showed abnormal bone findings (Table 2). On the retrograde review of the radiographs for the 22 children that underwent a radiography prior to US, three fractures which were missed on the initial image readings were detected.
Ultrasound Findings
1. Bone surface abnormality
Discontinuity (direct sign of a fracture) of the crisp hyperechoic cortex was clearly visualized in most cases (n = 23/25, 92%). A questionable cortical discontinuity was positive in two cases (8%): one (case no. 12) showed diffuse irregularity of the bone surface; and the other (case no. 22), showed localized thinning and a wide area of muscle edema as auxiliary findings (Fig. 4).
2. Auxiliary US findings
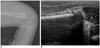
Auxiliary US findings (indirect signs of a fracture) include a definite step-off deformity in seven cases, a tiny bone fragment (i.e., avulsion) in five cases (Fig. 5), a double-line appearance of cortical margin in five cases (Fig. 6), diffuse irregularity of bone surface in five cases, and disruption of normal bone alignment in one case (Fig. 7) (double counted).
The various US findings for the various fractures were summarized as a diagram by authors (Fig. 8).
3. Impressions on US reports
The primary and secondary impressions on the US reports indicates that infection (septic arthritis or osteomyelitis) was suggested in seven cases, but a tumor was not suspected in any of the cases (Table 2).
DISCUSSION
The term 'occult fracture' is used for a fracture that is either radiographically undetectable or demonstrating subtle abnormalities that were missed on the initial prospective interpretation, even if the fracture is visualized retrospectively or confirmed by other imaging tests (15, 16). Contrary to adults, there are several obstacles in the diagnosis of fractures in children: minor trauma that may not be merited consideration by parents, poor localization of pain by young children, communication obstacle, unexplained trauma history, and physician oversight (1, 17). In our study, most of the cases with an unclear history of trauma (n = 6/25, 24%) were very young children. US is a helpful tool in diagnosing occult fractures when trauma history is unclear or a fracture is not suspected clinically. For some cases, fractures in children may not be initially suspected by the referred physicians. In the current study, three children (n = 3/25, 12%) did not undergo a routine radiography prior to US examination. Failure to recognize a subtle fracture on radiography is caused by overlapping structures, under-mineralized ossification centers, a non-perpendicular X-ray beam to the fracture line, poor image quality, and insufficient clinical information.
The incidence of pediatric cases of occult fractures occurs in about 2-18% of reviewed cases (1, 18). On the retrograde review of the initial routine A-P and lateral radiograms in our series, 13 out of the 25 cases showed no bone abnormalities except for soft tissue swelling. This demonstrates how subtle the radiographic signs of occult fractures may be and a negative radiographic result may provide a false sense of assurance. The absence of early management in these children may increase the complication rate (13). Thus, immobilization is critical for improving healing time, preventing potential growth arrest, fracture deformity, and to avoid discomfort (13, 19). However, the major limitation of this strategy is the undesirable over-treatment, resulting in unnecessary limitation of extremity motion, and a 1-2 week follow-up that is imposed on children without a fracture, as well as unnecessary visits for parents or guardians. As a result, about half of the children without fractures can be overtreated, and nearly one-third of children with a fracture can be under-treated (19).
Parents are commonly anxious of their children's condition and prefer a definite diagnosis with appropriate treatment rather than an empirical treatment with a splint or casting immobilization for a 1-3 week follow-up period. In these clinical contexts, a comparative radiography with the contralateral extremity may be helpful for a prospective suggestion of the diagnosis, although there is no total agreement as to whether one should obtain comparative views in all, or all potentially subtle cases (3). Unfortunately, radiography is not as sensitive in diagnosing soft tissue abnormalities compared to MRI and US. MRI is an excellent adjunct to a comparative radiography in the depiction of bone abnormalities, including intraosseous change as well as joint and soft tissue structures since it provides a global view of a region. However, MRI is expensive and frequently requires sedation. The other adjunct procedure to radiography, US, is useful in evaluating both soft tissue and bone surface abnormalities, however US cannot visualize intra-osseous abnormalities. Moreover, US is much better at depicting soft tissue compared to radiography with no radiation. In addition US is faster, cheaper, and more comfortable than MRI, without the need for sedation, especially in young children.
An abrupt cortical discontinuity (as the direct US sign of a fracture) and trauma history are the most important determining factors to correctly diagnose a fracture. However, there are pitfalls in interpreting cortical discontinuities. Anatomically, the growth plate in immature bones, accessory ossicles, secondary ossification centers, and canals or grooves for nutrient vessels, are delineated as a discontinuity of the bone surface and can mimic a fracture (6) (Fig. 7). In an experimental setting with cadaveric bones in a degassed water bath, fractures cannot be detected on US when a transducer is placed parallel to the course of the fracture line (20). Therefore, the transducer should be oriented orthogonally (i.e., at an angle of 90°) to the fracture line with an appropriate focus at the region of interest, and with the aid of the gain scale from the US machine to obtain the best depiction of the characteristic cortical disruption of a fracture.
When cortical discontinuity is not definite, auxiliary findings such as bone surface irregularity, soft tissue abnormality, history of trauma, and symptoms are very important for the correct diagnosis of a fracture. We surmise that a diffuse cortical irregularity with soft tissue edema at the fracture site, in our cases, may represent a bone contusion by blunt trauma with inflammatory change. In these cases, whether there is a history of trauma or not, we need to differentiate a fracture from an infection, a tumor, or even a metabolic disease because any pathology of bone or periosseous soft tissue may have similar US findings (6). The presence of a cortical irregularity by erosion is commonly present in acute osteomyelitis cases of children who have symptoms for more than one week (21). In addition, certain children with osteomyelitis may have a history of trauma (22). In our study, there were four cases referred with infection as the clinical information given prior to US and three cases referred with bone or soft tissue tumor as given clinical information. Of the seven cases, the US reports impressions included 'infection (n = 2)', 'fracture (n = 2)', and a 'fracture or infection (n = 3)'. In addition, two out of the three cases of osteomyelitis (which were excluded from the final enrollment in our study) were 'infection or trauma' by impression on US reports.
The limitations of this study are that the classification of fracture type was not performed and the trauma mechanism was not evaluated because we were concerned about whether an occult fracture was present or absent. Second, MRI, as a gold standard, was not performed in all the cases. However, clinical data, a follow-up radiography, and the treatment methods supported the final diagnosis. Third, the number of materials was not abundant. We need more wide study. Lastly, we did not include infection cases, which may have similar US findings (21, 22). Thus, a further study comparing the US findings of fractures and infections may confirm the value of US as an additional diagnostic tool in the early detection of occult or missed fractures.
In conclusion, US for soft tissue and bone surface in children with pain and swelling (with or without trauma history) is very important for the early detection of occult or missed fractures of immature bones in pediatric-aged children. US is a useful adjunct if MRI is not available. Understanding of the US findings of occult fractures will heighten the perception of subtle radiographic abnormalities which may be present, resulting in better patient evaluation with appropriate management.









 XML Download
XML Download