

 PDF
PDF ePub
ePub Citation
Citation Print
Print


An adenomyoepithelioma of the breast is a rare tumor, characterized by the biphasic proliferation of epithelial and myoepithelial cells (1, 2). Most cases of the tumors are of benign origin; however, malignant degeneration may also occur in rare cases (2-4). The imaging findings have reported a range of benign to malignant features (5-9). To the best of our knowledge, no previous studies have reported the radiologic findings of benign adenomyoepitheliomas according to Breast Imaging Reporting and Data System (BI-RADS). The purpose of this study was to investigate the ultrasonographic features of benign adenomyoepitheliomas and to correlate them with histopathologic findings.
MATERIALS AND METHODS
From 2005 to 2009, benign adenomyoepitheliomas were confirmed in five patients by ultrasonography-guided core needle biopsy. All patients were women and had a mean age of 50 years (range 31-72 years). Three patients underwent surgical excision, whereas one patient underwent a mass removal using a vacuum-assisted device. One patient was lost to a follow-up after the core biopsy. Medical records and pathology results were reviewed for the evaluation of clinical features and histology.
In all patients, a breast ultrasonography was performed. Mammograms were available for four patients. Breast magnetic resonance imaging (MRI) and positron emission tomography with computed tomography (PET/CT) were performed for cancer staging in one patient with concurrent breast cancer and for further evaluation in one patient who had image and pathology discordance, as well as a high suspicion of breast cancer.
The ultrasound images were acquired using a 7-15 MHz linear probe (HDI 5000, Advanced Technology Laboratories; Bothell, WA/iU22 Ultrasound System, Philips Ultrasound; Bothell, WA) and a 6-14 MHz linear probe (EUB-8500 scanner, Hitachi Medical, Tokyo, Japan). Two radiologists retrospectively analyzed the imaging findings for factors such as size, shape, margin, and internal echogenicity, as well as associated findings including ductal changes on ultrasonography, shape, margin, density, and the presence of calcifications on mammography, and the shape, margin, and internal enhancement on MRI. All lesions were described according to BI-RADS. The presence of fluorodeoxyglucose (18F-FDG) uptake and the maximal standardized uptake value (SUVmax) on PET/CT were reviewed.
RESULTS
The clinical characteristics of the patients are summarized in Table 1. Three patients presented with palpable breast masses, and two patients were asymptomatic and were referred for further investigation with a screen-detected abnormality. The size of the adenomyoepithelioma varied from 0.5 cm to 3.4 cm (mean, 1.5 cm). Four patients had a solitary breast mass, whereas one patient (Patient 1) had two masses of adenomyoepithelioma and ductal carcinoma in situ. After mass excision, the final pathology revealed benign adenomyoepithelioma in all patients, except for one patient who was lost to follow-up without surgery. One of the patients (Patient 5) showed a small area of atypia.
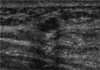
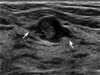
The ultrasonographic findings are summarized in Table 2. The shapes of the masses were oval (n = 3) (Figs. 1, 2) and irregular (n = 2), and the margins were angular (n = 3) (Fig. 3A), microlobulated (n = 1) (Fig. 1), and relatively well-circumscribed (n = 1) (Fig. 2). The internal echogenicities were hypoechoic (n = 3) (Fig. 3A) and complex echoic with a cystic component (n = 2) (Fig. 4). The posterior acoustic features were enhancement (n = 4) and a combined pattern (n = 1). The mass with combined posterior acoustic features had calcifications within the mass (Fig. 4A). Three patients showed focal ductal dilatation adjacent to the mass (Figs. 2, 3). Ultrasonographic assessments were classified as BI-RADS category 4A, with low suspicion of malignancy in two cases, and as category 4B, with intermediate suspicion of malignancy in three cases.
Mammograms were available for four patients. In two patients (Patients 1 and 2), lesions were not discriminated due to the high density of the breast. In two patients, the lesions appeared as an oval, obscured, isodense mass (Patient 3) (Fig. 3B) and as an irregular, indistinct, hyperdense mass with linear microcalcifications (Patient 5) (Fig. 4B).
MRI and PET/CT were performed in two patients. Patient 1 showed an oval, smooth mass with homogeneous enhancement and a delayed persistent pattern on the kinetic curve. No FDG uptake was noted on PET/CT. Patient 5 demonstrated an irregular, spiculated mass with heterogeneous enhancement (Fig. 4C, D) and a delayed washout pattern on the kinetic curve. Moreover, FDG uptake was observed along with a SUVmax of 4.9 (Fig. 4E).
DISCUSSION
Adenomyoepithelioma was first described by Hamperl in 1970 (1). Adenomyoepithelioma arises from myoepithelial and epithelial cells in the normal breast lobules and ducts. Most cases of the tumors are of benign origin, and characterized by the biphasic proliferation of epithelial and myoepithelial elements (2, 4). Adenomyoepitheliomas involving one or, more rarely, both cellular elements may also be malignant (2, 10). If a benign adenomyoepithelioma is diagnosed after a fine needle aspiration cytology or a core biopsy, then the total excision of the lesion with a margin of uninvolved breast tissue is recommended (11). A benign or malignant adenomyoepithelioma may recur locally, even several years after an initial surgical excision (3).
The clinical characteristics of adenomyoepithelioma have been rarely reported. In the current study, the mean patient age was 50 years old, but the range was variable (31 to 72 years). Adenomyoepithelioma has been found to develop more frequently in elderly women (2, 4). In most cases the chief complaint was found to be a palpable mass (2, 4). If rapid enlargement is present, the malignant change can also be considered (5). All of the three symptomatic patients in our study complained of nontender palpable masses.
The imaging features of adenomyoepithelioma are nonspecific and have not been well described. On ultrasonography, benign lesions commonly manifest as relatively circumscribed hypoechoic masses and may have posterior enhancement, while malignant tumors may show poorly defined margins and posterior shadowing (5).
The benign cases of adenomyoepithelioma included in the this study were comprised of two cases with a BI-RADS category 4A and three cases with a BI-RADS category 4B, which were in need of a tissue biopsy. In cases classified as BI-RADS category 4B, in which a tissue biopsy showed benign results, a correlation with histopathologic findings was mandatory. In Patient 5, a non-circumscribed mass with suspicious malignant calcification was present on ultrasonography and mammography, as well as a wash out pattern of enhancement on MRI. These imply that there is a high possibility that all of the radiologic findings are of malignant characteristics. However, the histopathology results suggested a benign adenomyoepithelioma accompanying the small area of atypia.
On mammograms, benign lesions commonly manifest as relatively circumscribed masses, and malignant tumors may show poorly-defined margins and architectural distortions (5). Combined calcifications are rare on mammography (8, 9). The malignancy-mimicking lesion, identified in our study was a suspicious malignant calcification.
Nonspecific MRI findings cases of a benign adenomyoepithelioma that mimicked malignancy are extremely rare (9, 12). To the best of our knowledge, no reports about PET/CT findings for the adenomyoepithelioma have been documented. In the current study, there were cases in which no FDG uptake was found, and those in which the hot uptake which occurred had a SUVmax of 4.9. The PET/CT findings warrant further study.
There are some reports in which most cases of adenomyoepithelioma are variants of the intraductal papillary tumor, with most cases having gross findings of a solid tumor rather than a cystic mass (2). Although rare, cystic changes have been reported in patients with adenomyoepithelioma (2, 4). Papaevangelou et al. (13) and Noel et al. (14) reported cases of adenomyoepithelioma of the cystic papillary type. In the current study, three cases were solid masses and two cases were complex echoic masses with the concurrent presence of a cystic portion. One case had an intracystic solid mass, while the other case had a cystic portion around the solid mass. Three cases with solid masses (60%) showed duct dilatation around the mass. This finding might be caused by the neoplastic proliferation of the adenomyoepithelioma compressed or obstructed in the adjacent duct space (12).
The limitation of this study is that a retrospective review of benign adenomyoepithelioma, which had suspicious malignant features, was biopsied and thus, the ultrasonographic features were too difficult to generalize as the usual benign adenomyoepithelioma.
In conclusion, adenomyoepithelioma is a rare breast tumor. However, adenomyoepithelioma should be considered by making a differential diagnosis of a mass that is accompanied by the complex echoic mass or ductal dilatation. Benign cases of adenomyoepithelioma may show suspicious malignant ultrasonographic features, which cannot be easily differentiated from malignant adenomyoepithelioma changes that are concurrently present in rare cases. The use of tissue biopsy and surgical excision should therefore be essential.




 XML Download
XML Download