

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Coronary artery disease (CAD) is one of the leading causes of death in developed countries despite that there has been a significant reduction of the mortality rates during past decades (1, 2). CAD predominantly manifests in older individuals, and the incidence of symptomatic CAD in young adults is low; most studies have shown that only about 3% of all CAD cases and 2% to 6% of all infarctions involve individuals under the age of 45 (3).
Although young patients with myocardial infarction exhibit fewer comorbidities, lower rates of in-hospital mortality and more favorable outcomes on short-term follow-up than do the older patients (4), their long-term prognosis is often rather poor, with an overall 15-year mortality rate of 30% (5). Therefore, the early detection and treatment of subclinical CAD and the prevention of developing acute coronary events should be emphasized in young adults.
Because young, asymptomatic patients typically do not undergo medical evaluations for CAD, not much data exists regarding the prevalence and characteristics of CAD in young asymptomatic individuals. In the current study, we used coronary CT angiography (CCTA) to evaluate the prevalence and CT characteristics of subclinical coronary atherosclerosis in asymptomatic Korean individuals who were under 40 years of age and who exhibited coronary risk factors.
MATERIALS AND METHODS
Study Population
We retrospectively evaluated 128 consecutive young adults who were under 40 years of age and who had undergone a CCTA evaluation with 64-slice multidetector CT (MDCT) as a screening test for detecting CAD during a general health evaluation from January 2006 to May 2008. We excluded 16 subjects who had chest pain or discomfort (n = 15) and those with a history of acute coronary syndrome (n = 1). None of the subjects were excluded due to nondiagnostic CCTA image quality. As a result, 112 asymptomatic young adults (90 men and 22 women) were finally enrolled. The mean age of the study population was 35.6 ± 3.7 years (range: 28-40 years). All the subjects had conventional coronary risk factors such as diabetes mellitus (n = 8), cigarette smoking (n = 54), hypertension (n = 36) or obesity (n = 62). There were 77 subjects with a low CAD risk, 27 with a moderate risk and eight with a high risk. Our Institutional Review Board approved this retrospective study and patient informed consent was waived.
Data Acquisition
A single oral dose of 20 mg of a β-blocker (propranolol [Pranol; Daewoong, Korea]) was administered one hour before MDCT for the patients with a heart rate of > 65 beats per minute (bpm). For those with a heart rate that was still greater than 65 bpm, an additional 20 mg of oral propranolol was administered one hour after the administration of the first dose of oral β-blocker. CCTA was not performed for patients with heart rates more than 70 bpm after repeated drug administration or for those with an intermittent arrhythmia. Coronary vasodilatation was achieved by administering 0.6 mg nitroglycerin (Myung Moon, Seoul, Korea) sublingually before the CCTA to obtain the maximum coronary artery opacification.
All the examinations were performed using a 64-slice MDCT (SOMATOM Sensation 64, Siemens Medical Solutions, Germany) and the following scan parameters were used: tube voltage 120 kVp, tube current 750 effective mAs, detector collimation 64 × 0.6 mm, gantry rotation 370 msec and pitch 0.24. Retrospective electrocardiogram (ECG) gating and ECG-gated dose modulation were used. A bolus of 70 ml iopamidol (370 mg of iodine per milliliter; Iopamiro 370; Bracco, Milan, Italy) was injected intravenously into an antecubital vein at a flow rate of 4 ml/sec, and this was followed by a 40-50 ml saline chaser using the bolus tracking technique. The images were initially reconstructed at the mid-diastolic phase (60-70% of the RR interval) of the cardiac cycle, and they were then transferred to a computed workstation (Leonardo, Siemens Medical Solutions, Germany).
Image Analysis
All the scans were retrospectively analyzed on a three-dimensional workstation by two radiologists (14 and 7 years of experience in chest CT, respectively), using the multiplanar reformation technique, the maximum intensity projection technique and the volume-rendering technique with a short-axis and the two-chamber and four-chamber views. The coronary artery tree was segmented according to the modified American Heart Association classification (15 segments), and these segments were subsequently investigated for the presence and characteristics of coronary plaques (6).
The degree of stenosis was classified as significant if the patient had more than a 75% area stenosis on the cross-sectional images or more than a 50% diameter stenosis on the longitudinal images.
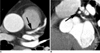
Coronary plaques were classified as non-calcified (plaques without visible calcification), mixed (plaques with non-calcified and calcified components) or calcified plaques (completely calcified plaques), according to the calcified component of the plaques seen on CCTA. Plaque densities of more than 130 HU (Hounsfield unit) on the native scans were classified as calcified (Fig. 1).
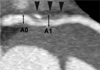
Changes in the coronary artery diameter were measured to determine the remodeling index (RI). The maximum outer diameter at the lesion and at the proximal reference site was measured to calculate the RI (i.e., RI = [maximum outer diameter at the plaque site - maximum outer diameter at the reference vessel] / maximum outer diameter at the reference vessel). Positive remodeling was defined as an RI > 0 and negative remodeling as an RI < 0. The degree of remodeling was calculated by percentage (i.e., mean values ± standard deviations). Measurements of the vascular diameter were obtained from the manually traced maximal diameters taken from the longitudinal source images (Fig. 2).
Coronary Artery Disease Risk Assessment and the Clinical Outcomes
All the study related data, including the demographics, symptoms, medical histories and laboratory results, was systemically acquired from the hospital database and a chart review. The conventional coronary risk factors such as obesity, cigarette smoking, hypertension, hypercholesterolemia and diabetes mellitus were assessed, and the serum biomarkers such as homocysteine, C-reactive protein and triglyceride were measured. The Framingham risk scores, as used by the National Cholesterol Education Program (NCEP) guidelines, were also calculated (7). All the subjects were assigned to one of three different risk groups according to the revised NCEP guidelines: the high-risk group (CAD risk equivalents or a 10-year risk > 20%), the moderate-risk group (more than two risk factors and a 10-year risk ≤ 20%) and the low-risk group (0-1 risk factors).
Of the 112 subjects, 109 underwent abdominal ultrasonography as part of a general health evaluation within one week of CCTA, and the presence or absence of a fatty liver was determined. The degree of fatty liver on ultrasonography was classified as follows: 1) a mild, minimal diffuse increase of the hepatic echogenicity with normal visualization of the diaphragm and intrahepatic vessel borders; 2) a moderate, moderate diffuse increase of the hepatic echogenicity with slightly impaired visualization of the intrahepatic vessels and diaphragm; 3) a severe, marked increase of the echogenicity with poor visualization or nonvisualization of the hepatic vessels and diaphragm. We also compared the patients with CAD to the normal subjects with respect to the coronary risk factors and a fatty liver.
The clinical follow-up data (range: 10-39 months) was obtained from the patients who exhibited CAD on CCTA, based on the cardiac events, the treatment and the laboratory findings.
Statistical Analysis
All the statistical analyses were performed using SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL). The differences between categorical variables were analyzed using Chi-square or Fisher's exact tests, and the differences between continuous variables were analyzed using the unpaired Student's t-test or Mann-Whitney test, as appropriate. A p < 0.05 was considered significant.
RESULTS
Atheromatous plaques were noted in 15 segments in 12 of 112 subjects (11%). Nine patients had single-vessel disease, and three had two-vessel disease. There were 11 men and one woman with an age range from 31 to 40 years (mean age: 36.8 ± 2.6 years) with atheromatous plaques. The patient population included four of 77 subjects (5%) with a low CAD risk, six of 27 (22%) with a moderate risk and two of eight (25%) with a high CAD risk. The prevalence of CAD was significantly higher in the moderate CAD risk group than that in the low risk group (p = 0.018); however, there was no significant difference between the moderate and high risk groups (p = 0.604) (Fig. 3).
The presence of obesity, hypertension, hypercholesterolemia, high triglycerides and fatty liver was significantly higher in the patients with CAD than that in the normal individuals. There also tended to be a higher incidence of cigarette smoking, high LDL (low-density lipoprotein) cholesterol, low HDL (high-density lipoprotein) cholesterol, diabetes mellitus and high C-reactive protein in the patients with CAD; however, any statistical significance was not identified (Table 1).
The location and degree of stenosis as well as the type of plaque are shown in Table 2. The coronary plaques were located in the left anterior descending (LAD) (n = 11, 73%) and the left main (LM) (n = 4, 27%) arteries, with the most common location being the proximal LAD (n = 9, 60%) (Fig. 4). All the coronary segments with plaque exhibited non-significant stenosis. The types of plaque included non-calcified (n = 4, 27%), mixed (n = 7, 47%) and calcified (n = 4, 27%).
The changes in the vascular diameter at the CAD site were measured in four coronary segments with noncalcified plaque and in seven with mixed plaques. This measure was not evaluated in segments with calcified plaques because the exact measurement of the vascular diameter was unavailable due to beam-hardening and blooming artifacts. Positive remodeling was identified in all the segments with noncalcified or mixed plaques, and the degree of positive remodeling tended to be higher in the patients with noncalcified plaques than in those with mixed plaques (Table 3); however, there was no statistically significant difference between the two groups (p = 0.471).
Twelve patients with CAD have been free of cardiac events 10-39 months after CCTA. Four of the five patients with hypercholesterolemia started antihypercholesterolemic medication, based on the results of the CCTA, and they showed improvement of their hypercholesterolemia on the follow-up tests.
DISCUSSION
Early detection of CAD provides the opportunity to initiate interventions that will stabilize existing lesions, including LDL-lowering drug therapy (statins), smoking cessation intervention for cigarette smokers, blood pressure lowering for persons with hypertension, and lifestyle intervention for the physically inactive and obese. Such interventions can reduce the risk of developing acute coronary syndromes later in life.
The current approach for managing the asymptomatic individuals who are at risk for CAD is based on traditional clinical risk assessments such as the Framingham risk score or the NCEP guidelines (7). However, there is growing evidence that these traditional risk assessment tools, which are based on risk factor analysis, have substantial limitations when they are used to guide individual therapy (8, 9). In a recently published study by Choi et al. (10) in which CAD was evaluated using CCTA in 1,000 middle-aged asymptomatic adults (mean age: 50 years), CAD was noted in 215 subjects (22%). This rate is higher than that observed in earlier studies (3-5%), and the results were confirmed by coronary angiography in the asymptomatic individuals (11-13).
To date, there is a paucity of data regarding the prevalence of atherosclerotic plaques as detected on CCTA in asymptomatic young adults, and this is largely because these asymptomatic young adults typically do not undergo medical evaluations for CAD. In this study that enrolled asymptomatic young adults (i.e., < 40 years of age) who were at risk for CAD, coronary plaques were demonstrated in 11% of the subjects, and the prevalence of CAD was significantly higher in the subjects with moderate (22%) or high (25%) risk than in those subjects with low risk (5%).
Positive remodeling was noted in all the coronary segments that exhibited noncalcified or mixed plaques with non-significant stenosis. This finding may indicate an important cause for underestimating CAD on coronary angiography and it may explain the acute coronary syndrome of young patients with angiographically normal coronary arteries (14-16). Positive remodeling occurs in the early stages of coronary plaque development, and it is well known that positive remodeling is related to plaque instability, suggesting it is more prone to rupture and erosion with subsequent coronary events (17-19). Nakamura et al. (19) reported that positive remodeling was observed more frequently in patients with acute coronary syndrome (78-82%) than in patients with stable CAD (33-40%), and a significantly higher degree of positive remodeling was noted in patients with acute myocardial infarction (remodeling index, 1.26 ± 0.15) than in elderly patients with unstable angina pectoris (1.11 ± 0.10) or stable angina pectoris (0.94 ± 0.11) (mean age, 63 ± 10 years). Tanaka et al. (18) demonstrated that all lipid core plaques showed positive vascular remodeling, which is in contrast to the severely calcified plaques that did not show positive remodeling. Furthermore, it is well known from angiographic studies that most myocardial infarctions occur at sites that previously caused only mild to moderate luminal stenosis (20, 21). Taken together, these studies demonstrate the clinical significance and importance of early plaques with mild stenosis.
This study found the highest frequency of coronary plaques in the proximal LAD. Choi et al. (10) also reported that 85% of CAD presented at the LAD. In our study, plaques were not observed in the left circumflex artery, the peripheral branches of the coronary arteries or the diagonal branches. This may have resulted from the limited temporal resolution of CCTA, which would underestimate the small branches of the coronary arteries, or it may also result from a lower prevalence of plaques in those segments in patients with early-stage CAD.
The coronary calcium score is intimately associated with the total plaque burden (22) and it is a strong predictor of coronary events, and the coronary calcium score is independent of the traditional coronary risk factors or risk-factor scores (23). However, it sometimes fails to predict acute coronary events or significant stenosis because a significant numbers of vulnerable plaques tend to be predominantly noncalcified and nonstenotic lesions (20). The absence of coronary calcification has been described in 1% of the male patients with significant coronary stenosis (24) and in 4% of the patients suffering from an unheralded myocardial infarction (25). In our study, 27% of the patients with CAD had only noncalcified plaques, which is slightly higher than the 19% reported by Choi et al. (10). This may be linked to the observation that the plaques in young patients are probably in the early stages, so they have less calcification than those of older individuals. Therefore, the coronary calcium score may underestimate CAD in young adults to a greater degree than that in older individuals.
Obesity, smoking, hypertension and hypercholesterolemia are well known risk factors for CAD, and their incidences were significantly higher in the patients with CAD than that in the normal subjects of our study. In a recent report, fatty liver was demonstrated to be associated with the risk of CAD and early atherosclerosis in middle-aged individuals (26). In the current study, we were able to evaluate the incidence of fatty liver because almost all the subjects underwent abdominal ultrasonography and CCTA as a part of a general health evaluation. As such, we also found that a fatty liver was significantly more prevalent in the patients with CAD (83%) than that in the normal individuals (39%).
Our study had some limitations. The study population was small, it included only Koreans living in urban areas and all the subjects were self-referred. Therefore, the actual prevalence of CAD in the young asymptomatic subjects in various ethnic groups and geographic regions may differ from our results, although this was evaluated in relation to the NCEP CAD risk categories.
In conclusion, the prevalence of occult CAD was not negligible in asymptomatic young adults, and the prevalence of CAD was significantly higher in those subjects with moderate to high risks than in those with low risk. Additionally, most of the patients had single-vessel disease, plaques of various composition, non-significant stenosis and positive vascular remodeling and one fourth of the patients had non-calcified plaques. Finally, the most common location for plaques was the proximal LAD. This study suggests the importance of management and risk factor modification for the asymptomatic young adults who have a moderate or high risk for CAD.





 XML Download
XML Download