

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It is important for the surgeons to have extensive preoperative knowledge of the renal vascular anatomy for selecting the proper kidney and for the surgical planning when performing laparoscopic donor nephrectomy (1, 2). Depiction of the vascular variants on the preoperative imaging facilitates the dissection of these vessels and it helps avoid vascular injuries. Planning nephron-sparing surgery in a case of a renal neoplasm also requires precise localization of the renal lesion and its relationship to the renal vasculature (3). Multidetector CT (MDCT) angiography is a fast, reliable and non-invasive modality for the comprehensive evaluation of the renal vasculature (4, 5). MDCT angiography is currently the preferred investigation for evaluating prospective renal donors and it has replaced conventional angiography in many institutions. MDCT angiography can accurately depict the renal arterial and venous anatomy, including the smaller tributaries such as gonadal, lumbar and adrenal veins (4, 5).
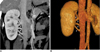
Various three-dimensional postprocessing techniques are employed for obtaining angiographic-quality images from the axial CT data. Of the many available reconstruction algorithms, volume rendering and maximum intensity projection (MIP) are most commonly employed (6, 7). The number, size, course and relationships of the renal vessels can be easily demonstrated by using real-time interactive editing of these reconstructions, and the vascular anatomy can be viewed from different perspectives by rotating these images. Curved planar reconstructions are useful to provide a visual summary of the entire vascular anatomy over a single image. As the MIP images lack depth orientation, the volume-rendered images are better than the MIP images for displaying complex anatomy, and especially when overlapping vessels are present (6). The renal arterial anatomy is evaluated on the arterial phase images (1). The major variations of the renal veins are well depicted on the arterial phase images; however, optimal visualization of the large systemic venous tributaries sometime requires additional evaluation of nephrographic phase images (1, 4). All the cases presented in this article were evaluated on a 64 channel multidetector scanner (Brilliance CT, Philips Medical systems, Cleveland, OH) at our institution. The MIP and volume rendered images were reconstructed on a 3 D work station (Extended Brilliance workspace, Philips Medical systems). The purpose of this pictorial review is to describe the usefulness of MDCT angiography for demonstrating the normal and variant renal vascular anatomy. The venous anomalies are described in detail to familiarize radiologists with the various anomalies of the renal veins.
NORMAL RENAL VASCULAR ANATOMY
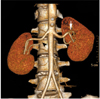
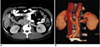
Most individuals have single renal arteries on either side that originate from the abdominal aorta at the level of the L2 vertebra (6) (Fig. 1). The right renal artery has a long downward course due to the inferior position of the right kidney and it lies behind the inferior vena cava (IVC). Classically, each kidney has a single renal vein that usually lies anterior to the renal artery at the renal hilum (Fig. 1). The left renal vein is longer than that of the right renal vein and the left renal vein measures 6-10 cm in length. It normally courses between the superior mesenteric artery and the abdominal aorta and then it joins the medial aspect of the IVC. The right renal vein has a short course, measuring 2 to 4 cm in length, and it joins the lateral aspect of the IVC. Unlike the right renal vein, the left renal vein receives several tributaries, which include an adrenal vein superiorly, a gonadal vein inferiorly and a lumbar vein posteriorly (6) (Fig. 2). Tributaries of the left renal vein, and especially the posterior lumbar branches, are of potential surgical importance if they are noted to be enlarged. The left kidney is preferred for laparoscopic donor nephrectomy due to the longer renal venous pedicle; however, a right nephrectomy may be performed if complex vascular anatomy precludes resection of the donor's left kidney (8).
EMBRYOLOGY OF THE RENAL VEINS
Variations of the renal veins and IVC are related to the developmental processes in the fetus (9, 10). The renal venous collar is made up laterally by the paired dorsal and ventral primitive renal veins on each side, which are linked to the centrally paired ventral subcardinal and dorsal supracardinal veins, and anastomoses of these four craniocaudally oriented subcardinal-supracardinal veins (Fig. 3). Different anatomic presentations of the renal veins are encountered depending on the persistence or regression of different components of this primitive circumaortic venous network.
RENAL ARTERY VARIATIONS
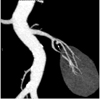
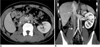
More than one artery supplying a kidney is the most common arterial variation, and this is seen in about 24% of cases (11) (Figs. 4, 5). These arteries are divided into two groups: hilar (accessory) and polar (aberrant) arteries. The accessory arteries enter kidney from the hilum along with the main renal artery, whereas the aberrant arteries enter the kidney directly from the capsule outside the hilum. These accessory/aberrant renal arteries usually originate from the abdominal aorta or iliac arteries; however, they can, on rare occasion, arise from the lower thoracic aorta or from the lumbar or mesenteric arteries (6). Early arterial branching or prehilar branching is diagnosed when the first renal branch arises within 1.5 cm of the renal artery ostium (Figs. 5, 6). Early branching is seen in about 12% of the cases (4). Sometimes an aberrant course of the main renal artery may also be observed (a left renal artery arising from the distal abdominal aorta near the bifurcation or a left renal artery arising above the celiac axis; the right renal artery can have a precaval course) (4).
RENAL VEIN ANOMALIES
Raman et al. (1, 2) have classified renal vein anomalies into the major or minor subtypes. Major renal vein anomalies are those that result in altered surgical management, including creation of the venous anastomosis in the recipient. The major renal vein anomalies include supernumerary veins and the presence of a late venous confluence. On the left side, the major anomalies also include circumaortic or retroaortic renal veins and a left-sided IVC or a duplicated IVC. The minor venous anomalies bilaterally are those that influence the planning of donor laparoscopic dissection, but they did not alter the venous anastomosis procedure in the recipient and these include anomalies associated with the lumbar, gonadal, adrenal and/or retroperitoneal veins, including the large gonadal and lumbar veins (> 5 mm) and their associated confluence with the main or branch renal veins.
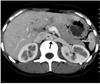
The most commonly encountered venous anomalies are multiple renal veins, which are seen in approximately 15-30% of patients (5, 6). Multiple renal veins are more common on the right side and these occur in up to 30% of individuals (Figs. 8, 9). The other uncommon variants described on the right side include a late venous confluence and minor variants like drainage of a large gonadal vein into the right renal vein. On the right side, a late venous confluence is diagnosed when the renal vein branches coalesce within 1.5 cm of the anastomosis with the IVC (Fig. 10). In one series, late confluence of the venous trunk was reported in about 10% of the right kidneys (2). However, the presence of a late venous confluence on the right side has not been described by other studies as the authors observed that the right renal vein is short, and in almost all cases the confluence occurs within 1.5 cm from the IVC (5). Multiple right renal veins are a contraindication for donor nephrectomy because this variant is associated with a higher incidence of thrombosis of the graft renal vein (4).
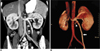
The most common anomaly of the left renal venous system is the circumaortic renal vein, and this is seen in 4.4-17% of patients (6, 12). In this variant, the left renal vein bifurcates into the ventral and dorsal limbs that encircle the abdominal aorta (Fig. 11). The appearance of a circumaortic left renal vein depends on the size of the retroaortic venous component, which is variable. Often the retroaortic component joins the IVC at a caudal level (Fig. 12). Sometimes a very small posterior branch from the left renal vein courses posterior to the aorta and the branch drains into the IVC. This posterior branch of the left renal vein is often difficult to differentiate from a lumbar vein or an ascending lumbar vein and in the usual clinical setting, such a small posterior branch is not called a 'circumaortic renal vein' (13).
Other main variants of the left renal vein include a retroaortic left renal vein, double IVC and late confluence of the renal venous trunk. A single retroaortic renal vein is a less common venous anomaly, and this is seen in 1.8-3% of patients (4, 12). A retroaortic left renal vein forms if the dorsal part of the supra-subcardinal vein anastomosis and the intersupracardinal anastomosis persist, whereas the ventral part of the supra-subcardinal anastomosis and the intersubcardinal anastomosis regress. Here, a single left renal vein courses posterior to the aorta and it drains into the lower lumbar portion of the IVC (Fig. 13). Sometimes, the retroaortic renal vein drains into the iliac vein (6). Double IVC is a relatively uncommon condition with a reported incidence of 0.2-3% (9, 14). It results from failure of regression of the embryonic left supracardinal vein. The duplicated left IVC usually drains into the left renal vein, and the left renal vein then crosses anterior to the aorta and joins the right IVC in a normal fashion (Fig. 14). A late venous confluence of the left renal vein is seen in 7-17% of cases (2, 4). On the left side, a late venous confluence is diagnosed when the renal vein branches coalesce within 1.5 cm from the left lateral margin of the aorta (Fig. 15). Preoperative knowledge of the late left venous confluence helps laparoscopic surgeons to anticipate two venous transections if they cannot gain control around the short main renal vein segment. Usually a 5-mm-or-larger gonadal or lumbar vein is present in patients with late venous confluence and it generally it drains into a branch of the main renal vein rather than into the main renal vein itself.
The left renal vein often communicates with the retroperitoneal veins, including the adrenal, lumbar, gonadal and hemiazygous veins. Knowledge of these venous tributaries is relevant and especially the ones that are connected on the posterior aspect of the left renal vein, where the laparoscopic visualization is limited (15, 16). A 5-mm-or-larger gonadal or lumbar vein is seen to drain into the main renal vein in about 40% of cases for the left kidneys or a 5-mm-or-larger gonadal or lumbar vein is seen to drain into a branch renal vein in 14% of the cases for the left kidneys (2) (Figs. 16, 17). In many cases, the gonadal vein is joined by a lumbar branch before eventual insertion into the left renal vein (Fig. 16B). Sometimes an accessory renal vein may drain into the lumbar-gonadal complex (1). Multiple left adrenal veins are seen in 2% of patients and multiple left gonadal veins are seen in 7% of patients (13). Other uncommonly reported venous abnormalities are spontaneous spleno-renal shunts, an isolated renal varix, renal arteriovenous malformations and fistulas (6).
SUMMARY
Pre-operative depiction of the complete vascular anatomy is important for the surgical planning, and especially prior to performing laparoscopic nephrectomy and nephron-sparing surgery. Since laparoscopic nephrectomy is performed with a limited field of view, having knowledge of these vascular anomalies reduces the chance of vascular injury and hemorrhage. MDCT angiography is a reliable, non-invasive investigation for evaluating the renal vascular anatomy. The three dimensional volume rendered and MIP techniques are very helpful for accurately displaying various renal vascular anomalies.










 XML Download
XML Download