

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Voluntary embolization of the renal parenchyma has been used to treat kidney cancer since the 1970s. Many other applications for very different clinical situations have been developed during this period. We review here the various embolization techniques before presenting the indications for such treatments and the obtained results.
Techniques
Preprocedural Imaging
Performing pre-procedural imaging for the embolotherapy candidates is very important, and especially for assessing the tumoral or aneurysmal lesions. The suggested modalities for detecting kidney diseases include Doppler ultrasonography, magnetic resonance angiography and most importantly, computed tomographic (CT) angiography, which is gaining prominence for assessing patients with good renal function. Indeed, the three-dimensional imaging capability of modern day CT scanners has made CT scanners a potent tool for renal imaging. However, Doppler ultrasonography is the simplest investigation and it can provide both structural and functional information. It is highly useful in emergency situations. Arteriography is used less often than it was in the past, but it remains the first step of every endovascular procedure and for the cases of bleeding combined with hemodynamic instability.
Catheter Embolization
Precise mapping of the vascular bed, including the aorta and its branches, and a selective study of the involved kidney must be performed to plan the therapeutic strategy. A catheter sheath introducer is used systematically. In patients with atheroma or tortuous arteries, using a long sheath (35 to 45 cm) with the tip positioned just downstream from the ostium of the renal arteries facilitates iterative catheterization. The use of 4 Fr or 5 Fr conventional catheters and hydrophilic guidewires facilitates superselective catheterization and these devices make it possible to use microcatheters that are inserted co-axially into the approach catheter.
Adjuvant Medications
Embolization is performed under strict aseptic conditions, as is the case for any endovascular intervention. Depending on the indication and the context, the patient will be premedicated with analgesics, anxiolytics or neuroleptanalgesics. Administering prophylactic antibiotics in the days following the intervention is recommended for permanent embolization of the renal parenchyma.
Embolization Materials
Resorbable materials
These are pieces or particles of sterile synthetic gelatin sponge, and they are available in several commercial forms: Gelfoam® (Pharmacia & Upjohn Company, Pfizer, NY), Curaspon® (Cura Medical BV, Amsterdam, The Netherlands) and Gelitaspon® (Gelita Medical BV, Amsterdam, The Netherlands). This is a biodegradable material that is resorbed within 3 weeks to 3 months; it is well tolerated and easy to use. It can be in the form of particles that are 1 to 3 mm in diameter or in the form of sheets that need to be cut up. It is deformable, which makes it easy to insert into the catheter, but the final volume and the distribution are difficult to predict and they may change with time. The foam is prepared in a 10-ml syringe and a contrast agent is added to control the injection (1).
Non-Resorbable Materials
Agents for Distal Embolization
* Inert Particles
There are several different types of inert particles on the market: polyvinyl foam or polyvinyl alcohol (Ivalon®, Unipoint Lab., High Point, NC), acrylic polymer microspheres impregnated with gelatin (Embosphere Microspheres®, Biosphere Medical, Rockland, MA) and polyvinyl alcohol microspheres (Beadblock®, Terumo, Leuven, Belgium). These particles are calibrated in different sizes from 100 to 1,000 µ. They can be dry or diluted in an aqueous solution. It is useful to add a contrast agent to control the injection, which should always be done slowly with making sure that there is no reflux. The risk of reflux increases at the end of the embolization when the blood flow has been reduced. Deformable particles do not aggregate in the catheter and so they do not block it. Inert particles allow more precise embolization and the embolization is more durable than that with using resorbable materials. This type of material is ideal to exclude a small area of renal parenchyma such as a benign tumor or a lesion of the renal cortex.
* Liquids
There are various products on the market (1).
1) Alcohol solutions of polypeptides associated with a radiopaque agent (Ethibloc®, Ethnor Laboratories, Ethicon, Noderstedt, Germany). This is an occlusive gel that polymerizes in water in 1 to 2 minutes. This allows high-quality distal diffusion and therefore excellent peripheral occlusion of the parenchyma.
2) N-butyl 2-cyanoacrylate-type biological glue (Histoacryl®, B/Braun, Tuttlingen, Germany, or Glubran 2®, GEM SRL, Viareggio, Italy): this product polymerizes upon contact with an ionic medium, and particularly when contacting blood. The peripheral dissolution and the speed of polymerization depend on the degree of dilution in an oily contrast agent (Lipiodol®, Therapex, E-Z-EM, Montreal, Canada). Dilution is usually 1 to 4 (glue to contrast, respectively). It is essential to use a co-axial catheter. Once in place, the catheter is first filled with Glucose 5% D/W (G5%) rather than Lipiodol® to prevent the glue from polymerizing in the catheter. The Lipiodol®-cyanoacrylate mixture is then slowly injected until the blood flow has been slowed. A few drops of pure Lipiodol® or G5% are then slowly injected to clean the catheter, which is then systematically withdrawn. Control is ensured via the guide catheter. The use of G5% rather than Lipiodol® is preferable to rinse the catheter before and after injection of the Lipiodol®-glue mixture because of the radioparency of G5%. This property allows more accurate detection of the presence or the absence of the Lipiodol®-glue mixture at the tip of the catheter thanks to the radioopacity of Lipiodol®, which leads to a safer embolization procedure. Complete mastery of this technique is essential because of the risk of serious complications. However, this technique allows rapid distal occlusion of a voluminous vascular bed. It is particularly appropriate for preoperative renal devascularization and for the management of hemorrhage and arteriovenous malformations.
3) High concentrations of ethanol (between 95 and 99%) cause total tissue necrosis with permanent glomerular occlusion. The disadvantage of this material is that it is not radiopaque, which is why certain authors suggest adding 20% of Lipiodol® to it (2). Another drawback is the potential pulmonary toxicity (pulmonary edema, increased pulmonary arterial pressure), and this has been recently reported on by some authors (3, 4). It is also very fluid and it tends to quickly dilute in the blood and cause hemolysis. Injection under the control of a balloon catheter can provide more selective, safe and rapid embolization. The injection is often painful and the patients require analgesics. This material is often used to destroy kidney function. It is also used for renal tumor ablation.
Agents for Proximal Embolization
These are appropriate for the occlusion of a large lumen without distal migration.
* Metallic Coils
A piece of textile is fixed to the metallic coil to facilitate formation of the thrombus. The coils can be inserted via catheters or microcatheters, but the caliber of the coil must be suitable for the bore of the catheter. The sizes and shapes of the metallic coils vary according to the size of the vessel to be occluded. Microcoils are appropriate for the occlusion of false aneurysms or arteriovenous fistulas because they make it possible to exclude the diseased area while preserving irrigation of the downstream vascular bed. They also provide satisfactory proximal occlusion as a complement to distal occlusion.
* Occluders
Occluders, and notably the Amplatzer® Vascular Plug (AGA Medical Corporation, Plymouth, MN) system, are comprised of a nitinol cage filled with thrombogenic polyester filaments. Although they are expensive, they provide very rapid occlusion of the vessel lumen and full cross-sectional vessel coverage. The devices are ideal for high flow situations such as arteriovenous malformations, and they allow blocking a vessel that would have required many coils. They have the ability to be recaptured and repositioned, if necessary.
* Detachable Balloons
They are less frequently used today because they are difficult to insert and they are likely to be altered over time. However, they do have the advantage of providing a large volume of occlusion with great precision. They may be useful in certain aneurysms, in particular in pedicular aneurysms.
Summary
The choice of the embolization strategy (the technique, material and site) depends on the indication. Embolic materials for proximal occlusion can be used for occlusion of the renal artery. If the aim of the intervention is to destroy all or part of the parenchyma, then the intraparenchymal branches must also be occluded and possibly with complementary proximal occlusion. The first two or three centimeters of the trunk must be left intact to permit surgical ligature of the artery in the case of secondary nephrectomy.
Complications
Pain
Depending on the volume of the involved parenchyma, the pain usually starts during the embolization and it may last 1 to 5 days. There is very little pain when treating arteriovenous fistulas, but patients may experience intense pain during the first 24 to 48 hours following ablation of renal parenchyma with using ethanol. Patients must receive appropriate treatment with analgesics before, during and after the procedure.
Kidney Failure
Performing many examinations with agents that contain iodine, and particularly when treating tumoral diseases, may cause deterioration of the renal function. The patient must be appropriately hydrated before any embolization. In the case of palliative embolization, it is essential to preserve enough renal parenchyma to preclude the need for dialysis.
Post-Embolization Syndrome
This syndrome is almost inevitable in cases of destroying tissue and this syndrome includes nausea, vomiting, fever and abdominal pain. As a rule, the severity depends on the volume of the infarcted tissue. Paralytic ileus is often associated with the syndrome. Biological examinations will show hyperleukocytosis and an increased level of plasmatic lactate dehydrogenase. The syndrome generally resolves with symptomatic treatment in a few days.
Hematuria
Moderate hematuria may occur following embolization. This is related to hemorrhagic infarction and it generally resolves within 24 to 48 hours.
Infections
There is a risk that latent infections may flare up, which means doctors need to be familiar with the patient's medical record (a history of lithiasis or infection). Cytobacteriological examination of the patient's urine must be systematically performed before the intervention: a current urinary infection that is not controlled by appropriate treatment is a contra-indication for transcatheter arterial embolization. Small air bubbles have been found on the post-intervention CT images of patients with infection. They occur between the third and sixteenth day after the renal embolization. These air bubbles do not necessarily indicate an abscess, but they may correspond to normal aseptic infarction (7).
Accidental Embolization
This is always possible whatever the material used. There is a notable risk of pulmonary embolization due to coils, permanent inert particles or glue. A microcoil can be recovered using a lasso snare or by surgery. When alcohol or particles are injected, care must be taken to prevent the reflux of the material into non-targeted arteries, and particularly the digestive, gonadal and adrenal arteries, as this may cause serious complications. Indeed, some authors have reported pulmonary circulation toxicity with the use of ethanol (3, 4).
The Risks Associated with Any Type of Catheterization and the Injection of Contrast Agents
As with any endovascular procedure, embolization carries a risk of hematoma at the entry point, arterial dissection, thrombosis, distal embolism, anaphylactic reactions, shock, volume overload and kidney failure.
Practical Considerations
Before the Examination
The urine must be checked to make sure it is sterile. It is essential to make sure that the patient is comfortable as the intervention will cause pain; appropriate analgesics must be on hand. It is advisable to monitor the patient (ECG, blood pressure) throughout the procedure and during the following 24 hours.
During the Pre-Intervention Check-Up
It is necessary to look for possible early venous return and arteriovenous shunts. For tumoral lesions, the possibility of collateral extrarenal blood flow must be taken into account. For those patients with conservative indications, the adrenal, gonadal and ureteral vascularization must be preserved as much as possible, along with that of the healthy renal parenchyma.
During the Procedure
It is essential to take steps to prevent accidental embolization by ensuring the stability of the catheterization before the embolization. Imaging must be used to monitor the distribution of the occlusive agent and the residual blood flow in the embolized territory. The quantity of agent being injected should decrease in parallel with the progressive reduction in blood flow to the downstream vascular bed. The effect of the intervention must be evaluated morphologically at the end of the procedure. The control contrast agent must be injected far enough from the embolized territory, using a perfectly clean catheter, to avoid reflux accidents or accidental injections of the occlusive agent.
Go to : 
Indications
First of all, the contra-indications such as the presence of serious coagulation disorders or an infectious syndrome must be ruled out. Therapeutic embolization is not free of risks: such procedures have an 8% rate of morbidity and a 2.5% rate of overall mortality (8). Any procedure should only be performed once the benefits and risks to the patient have been carefully evaluated: rigorous analysis of the medical record and the indications is essential. The preintervention check-up must answer two questions: is embolization the most appropriate technique, and if so, what is the best embolization strategy (9)?
Malignant Tumors: Adenocarcinoma
Embolization can be considered in three types of situations (10).
Pre-Operative Embolization
Performing embolization in patients who are suitable for radical surgery (stages I to III) is controversial. It can be useful to reduce blood loss (11, 12) and to facilitate cleavage of the tumor, thanks to the reaction edema in the embolized territory. It seems advisable to limit this technique to large (> 9 cm), extensively vascularized tumors. By collapsing the perihilar vascular network, embolization may facilitate the approach to the pedicle in stage III tumors that show involvement of the renal vein. In cases where the renal capsule is involved, embolization may provide a better cleavage plane (13). In this case, embolization must be completed with distal occlusion of the vessels so as to more effectively devascularize the area to be excised (Fig. 1). Ethanol with or without Lipiodol® can be used, although cyanoacrylate or microparticles are more frequently employed for this; resorbable materials are rarely used. When microcoils are used for distal embolization, they must be positioned far enough from the ostium of the renal artery so as not to hinder the surgeon during ligature of the pedicle.
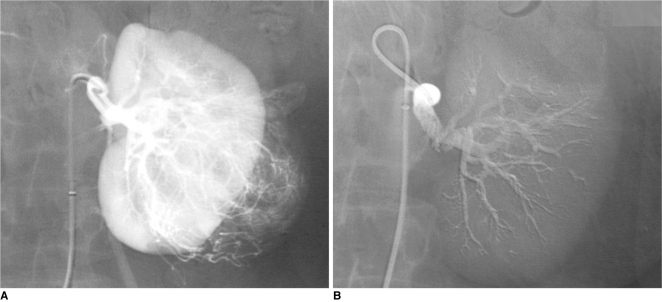 | Fig. 1Preoperative glue embolization of renal cell carcinoma before nephrectomy in 69-year-old man.
A. Selective renal arteriogram: large vascular tumor in lower-pole of left kidney.
B. Control angiogram after embolization of entire renal artery using radiopaque cyanoacrylate/Lipiodol mixture (1:3): complete occlusion of renal artery allows minimal intraoperative blood loss and easier nephrectomy.
|
Palliative Embolization
There is no controversy concerning embolization in patients with end-stage renal disease (13-17). It is performed for relieving symptoms to improve the quality of life and to treat certain complications: persistent macroscopic hematuria with anemia, treatment-resistant low back pain, heart failure due to arteriovenous shunt and excessive blood flow, arterial hypertension, hypercalcemia and polycythemia. In this context, complete embolization is not always necessary, and interventions must be limited to relieving the symptoms. The drawbacks of embolization, and notably deterioration of renal function, infections and post-embolization syndrome, can thus be reduced. Partial embolization is far less aggressive than surgery. Some authors have reported that embolization in patients with end-stage renal disease can increase survival by several months (14).
Pre-Operative Embolization in Patients with Metastases
When the metastases are limited to the lungs, nephrectomy has been shown to lead to spontaneous regression. In this context, certain medical teams have performed embolization together with nephrectomy and systemic chemotherapy. These authors have reported an improvement in survival (14). These results have been widely contested by other teams, who report similar results whether or not nephrectomy or embolization is performed (18).
Benign Tumors: Angiomyolipoma
In the vast majority of cases, there is only one small sporadic hamartoma that does not require any particular treatment. Yet in some cases, the lesion is hypervascularized and the lesion contains a large number of vessels with walls that are deficient in elastic fibers and so the vessels are susceptible to the formation of aneurysms. Rupture of such aneurysms is responsible for hematoma in the perirenal space with pain in the side, and in one third of cases, hemorrhagic shock. They may be complicated by persistent hematuria due to a fistula in the urinary system. Hemorrhagic complications especially occur in tumors greater than 4 cm in diameter (19, 20) and in the context of Bourneville's tuberous sclerosis, for which 80% of the patients have multiple lesions (20) (Fig. 2). The diagnosis of aneurysm is made using ultrasonography, CT or MRI, and all these modalities clearly reveal the vascular behavior of these lesions.
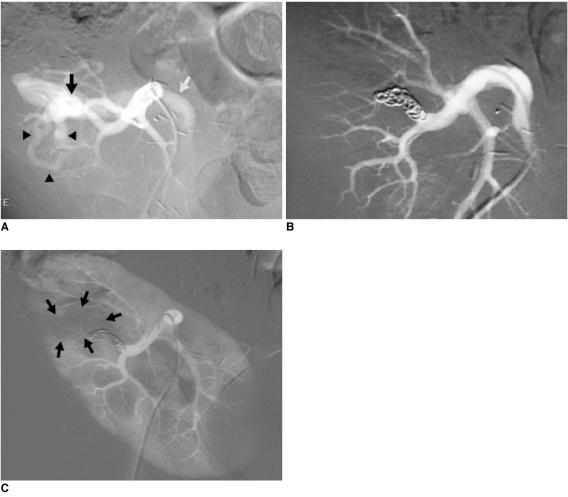
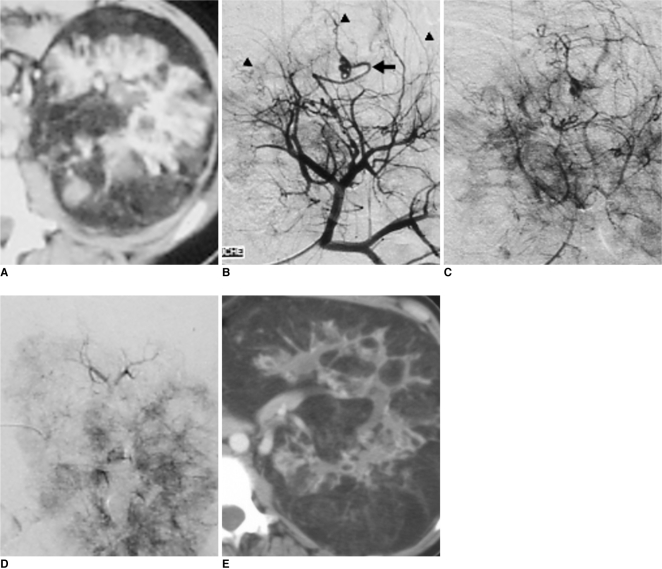 | Fig. 2Recent lumbar pain in 19-year-old patient with Bourneville's tuberous sclerosis.
A-C. CT scan (A) and arteriography (B, C) confirm modifications of renal vascular architecture, as related to fat infiltration and making upper-pole mass opaque (arrowheads) and mass corresponds to hemorrhagic angiomyolipoma. Vascularization of angiomyolipoma is ensured by atypical artery (arrow).
D. Results after superselective embolization with 300-500 µm calibrated microspheres using 3 Fr microcatheter: angiomyolipoma is completely devascularized without infarction of renal parenchyma.
E. CT scan at one year shows evolution of disease with predominant fat infiltration, but no hypervascularization.
|
Embolization is justified in patients with hemorrhagic syndrome as it stops the bleeding, and in many cases, it completely devascularizes the angiomyolipoma (Fig. 3). Therefore, surgery is not always necessary (19). The risk of hemorrhage cannot be neglected: for angiomyolipomas measuring more than 4 cm in diameter, it is of the order of 20% per year (19). For certain embolization teams, this is justification for preventive selective embolization of the tumor. Complete mastery of the technique is essential in such cases. For cases of diffuse lesions, in particularly when the masses are large and bilateral (20), embolization should also be considered, and when it is performed, as much of the renal parenchyma as possible should be preserved, while precluding the risk of hemorrhage. Unlike the procedure in malignant lesions, embolization must only target the territory of the tumor. The most frequently used agents are ethanol, with or without Lipiodol®, and inert particles (21, 22). Cyanoacrylate can be used in certain cases. Resorbable materials should be avoided as they only provide temporary occlusion. The occlusion provided by microcoils is too proximal and it carries a substantial risk of revascularization.
 | Fig. 3Preventive embolization of large renal angiomyolipoma in 63-year-old woman.
A. Aortography showing round, well-defined intraparenchymatous mass 4 cm in diameter in upper pole of right kidney (arrowheads).
B, C. Selective renal angiogram confirms hypervascularized character of angiomyolipoma.
D, E. Final angiography after using 300-500 µm microspheres to superselectively embolize two main arterial branches with using 3 Fr microcatheter: devascularization of entire angiomyolipoma (arrowheads) with respect to rest of renal parenchyma.
|
Traumatic or Iatrogenic Lesions
Injury to the lower back, and particularly stab wounds and percutaneous biopsies of the kidney, can cause vascular lesions that may give rise to various complications: embolization may be a therapeutic option in such cases (23-25).
In the Acute Phase
In the hours that follow the trauma, it may not be possible to stop the bleeding, which may result in a state of shock (9). Emergency arteriography will very often reveal the injured vessels (23). It is quite simple to occlude the artery that feeds the damaged region using inert particles, resorbable material, glue or microcoils according to the morphology of the lesions (Fig. 4). Hemostasis can generally be achieved (24). The few reported incidences of recurrent bleeding occurred when resorbable material was used. In these cases, the bleeding was stopped by repeat embolization. The renal infarction that can result from such interventions is often invisible or minor, as can be noted on surveillance examinations. This technique is only slightly aggressive and it preserves the renal parenchyma.
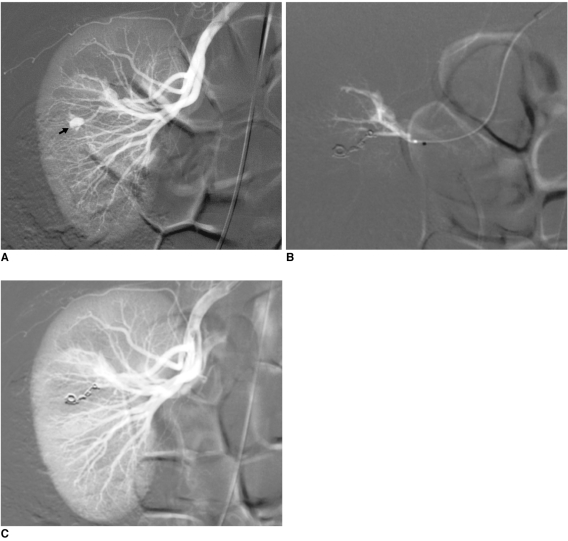 | Fig. 4Emergency embolization for arterial injury after blunt renal trauma in 51-year-old woman.
A. Extravasation of contrast medium (pseudoaneurysm-like lesion) from lower distal-pole branch at selective angiography indicates continuous bleeding (arrow).
B. Selective embolization of feeding artery using detachable microcoils.
C. Control angiogram shows complete and selective occlusion of bleeding branch, with no active bleeding.
|
In the Post-Acute Period
The main problem in the post-acute period is persistent hematuria through the creation of an arteriourinary fistula (25, 26). This very frequently occurs following renal biopsy, and it generally closes spontaneously within a few days. Should it persist for more than a week, it may complicate recovery. Percutaneous treatment consists of occluding the abnormal vessel responsible for the hematuria (Fig. 5). The blood losses are generally small and these generally concern the peripheral arteries. Embolization can be easily done using inert particles or more often one or two microcoils. Bedsores may appear towards the tenth day. The clot that blocks the puncture site may sometimes detach causing sudden severe hemorrhage, which may be particularly serious if the patient is no longer under medical supervision. As is the case in the acute phase, emergency embolization is particularly useful as it stops the bleeding and prevents complications.
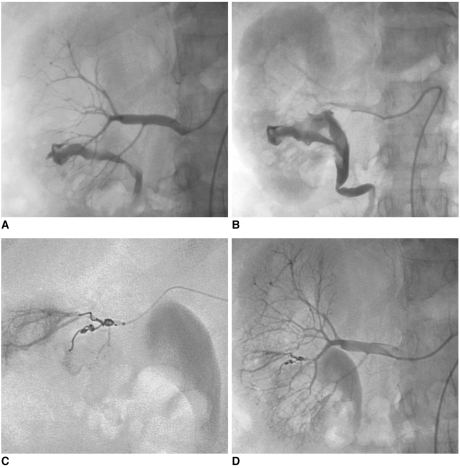 | Fig. 5Massive hematuria with hypovolemic shock two hours after performing percutaneous renal biopsy in 56-year-old woman.
A, B. Presence of high-flow arteriocaliceal fistula on emergency renal angiography with rapid opacification of urinary cavities.
C. Microcoil embolization of two abnormal vessels that were responsible for hematuria.
D. Complete occlusion of fistula and cessation of bleeding are seen on post-embolization angiogram.
|
Delayed Complications
Arteriovenous fistulas and false aneurysms are quite common, and their incidence increases with the number of percutaneous interventions and renal biopsies. Arteriovenous fistulas occur following almost 15% of renal biopsies, but only 4% persist after several months (23). The vast majority heal spontaneously. Arteriovenous fistulas may also occur following nephrectomy if the entire vascular pedicle is ligated en bloc. Fistulas are very rarely due to malformations, but the treatment is the same as that for acquired fistulas. The decision whether or not to repair this type of lesion depends on the blood flow through the fistula (heart failure, arterial hypertension), the risk of rupture in the case of large false aneurysms, and recurrent hematuria. In certain cases, fistulas are repaired to allow new renal biopsies to be performed (such as for a kidney transplant).
The morphology of the fistula must be carefully studied before embolization. The communication between the artery and the vein, or the false aneurysm when present should be the main target of the occlusion procedure (23). The principal technique is the deployment of metal coils (23, 27) or detachable balloons (28). An occlusion plug can sometimes be delivered into the feeding artery. Non-communicating false aneurysms are usually occluded using coils. In most cases, it is possible to preserve the downstream vascular bed and almost all of the renal parenchyma. Embolization is currently the treatment of choice for such fistulas (Fig. 6). There is no doubt that the results of embolization are far superior to those obtained with surgery. The incidence of complications is low for experienced teams.
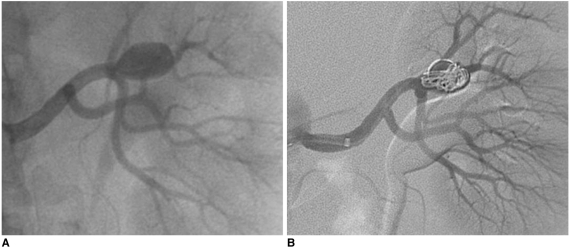
 | Fig. 6Progressive arterial hypertension in 43-year-old patient one year after percutaneous renal allograft biopsy.
A. Selective arterial angiogram: there is large arteriovenous fistula in upper-pole segmental branch of transplanted renal artery and pseudoaneurysm (black arrow) with marked arteriovenous shunting (arrowheads) and early venous filling (white arrow). Note absence of nephrogram.
B. Control angiogram after selective embolization of afferent artery with 0.035" coils: complete occlusion of pedicular aneurysm and fistula, and improvement in nephrogram.
C. Post-embolization angiogram (parenchymal phase): renal infarction is seen in less than 10% of renal parenchyma (arrows).
|
Pedicular Aneurysms
They may be congenital and they are often associated with a disease of elastic tissue (Ehler Danlos syndrome or Recklinghausen disease). Other causes include inflammation or infection (29). Traumatic pedicular aneurysms can be due to a direct wound or to dissection of the media due to deceleration in a car accident. Finally, atheromatous aneurysms are often associated with stenosing lesions. The risk of complications is difficult to assess. Rupture seems to be less frequent in pedicular aneurysm than that in digestive aneurysms and this depends on the size of the aneurysmal sac. Most authors consider that the risk of rupture is substantial for aneurysms greater than 2 cm in diameter. The risk of rupture also depends on the etiology, the symptomatology and whether or not the aneurysm is calcified. The risk of peripheral embolism is linked to the turbulence within the sac and the sac's shape (saccular or fusiform).
Many of these aneurysms require surgery, which is very effective. It is generally accepted that an asymptomatic saccular aneurysm of the renal artery of less than a 15 mm diameter should not be treated. Exceptions include women with normal genital function who wish to conceive, any aneurysm that engenders renal ischemia and arterial hypertension, any aneurysm associated with significant stenosis of the renal artery, any dissecting aneurysm, any aneurysm with distal embolization or any aneurysm that shows an increase in size on successive images. Embolization can be considered in frail patients with aneurysms that have a narrow neck or a favorable anatomical configuration (Fig. 7). In such cases the downstream bed and the arterial lumen must be preserved (30, 31). The aneurysm is generally occluded by inserting metallic coils into the sac. If the neck is wide, then a fenestrated endoprosthesis can be initially used to cover the aneurysm, after which the coils can be inserted via the windows in the prosthesis (32). The use of a recently developed small covered endoprostheses can sometimes simplify the procedure.
 | Fig. 767-year-old man with asymptomatic renal artery aneurysm that was incidentally discovered on CT scan of abdomen.
A. Selective arteriogram demonstrating filling of saccular renal aneurysm arising from hilar branch.
B. Control angiography after embolization of aneurysmal sac across neck with detachable fibered microcoils and using packing technique: there is near complete occlusion of aneurysm and preservation of main renal artery.
|
Functional Exclusions
In patients with end-stage kidney failure and arterial hypertension (33, 34) that does not respond well to medical treatment, or in those patients with severe proteinuria that is responsible for nephrotic syndrome (35), exclusion of the cause, i.e., the renal parenchyma, can be considered. This treatment can also be done in particular cases such as in patients who present with a chronic urinary fistula or hydronephrosis that cannot be treated with the usual therapies. In other cases, this treatment can be done for urinary ascites or urinary urgency in a secondary bladder. In end-stage kidney failure, the kidneys continue to perform three important physiological functions: vitamin D metabolism, erythropoiesis and sometimes the elimination of a certain quantity of water (from 200 to 2,000 ml). The loss of these functions must be weighed against the expected benefits of functional exclusion. Surgery in these weakened patients is associated with substantial morbidity (20%) and up to a 5% rate of death.
In most cases, uni- or bilateral renal embolization gives the desired results with reduced complications. The aim is to obtain total infarction of the kidney via the complete and irreversible destruction of the vascular system: there must be no viable parenchyma as it would compromise the result, and particularly with regard to arterial hypertension. For these reasons, the most frequently employed occluding agent is pure ethanol. It is injected under the protection of a balloon to prevent reflux into the other abdominal arteries. Other authors prefer to inject a mixture of alcohol with 25% of Lipiodol® to make the liquid radiopaque. As microparticles and glues are often more difficult to use, they have been less frequently evaluated for this indication.
Go to :
CONCLUSION
Therapeutic embolization to treat renal disease is indicated in very different disorders, such as cancer, trauma, iatrogenic complications, arterial hypertension and end-stage kidney failure. Any vascular radiology department may be called upon to perform such treatments and sometimes in an emergency setting. Embolization for the usual indications does not carry any major risks provided the indications are clearly established, and the techniques of arterial catheterization and endovascular embolization are completely mastered. As with any act of interventional radiology, the medical record must be carefully analyzed before the procedure, and the patient must be managed by the radiology team before, during and after the procedure. Special care must be taken that the patient's pain is adequately treated and that the follow-up continues once the patient has left the angiography room.
Go to :
 XML Download
XML Download