

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A supracricoid partial laryngectomy (SCPL) is an organ preserving surgical technique used for the treatment of selected glottic and supraglottic laryngeal cancers (1, 2). The technique consists of resecting the entire thyroid cartilage including the vocal folds, paraglottic, spaces and the preepiglottic space, while sparing the cricoid cartilage and at least one of the mobile arytenoids (1, 3, 4). The unilateral arytenoid cartilage disarticulation and resection is performed at the time of the SCPL in patients with a lesion occupying the mucosa within the region of the arytenoid cartilage or with a fixed true vocal cord and impaired arytenoid motion (1).
The most common type of tumor recurrence after SCPL procedures involves an eccentric submucosal extension, particularly in the cricoid or cricoarytenoid region (5, 6). A CT scan facilitates the detection of recurring submucosal lesions by the appearance of abnormal thickening in the neoglottic area. The accuracy of the CT scan in the postoperative evaluation of the larynx has been reported, but with limited information on the radiological findings of the arytenoidectomy site following a SCPL (7-11).
We retrospectively analyzed neoarytenoid soft tissue in patients following a SCPL with or without an arytenoidectomy. The thickness of neoarytenoid soft tissue at the arytenoidectomy site was measured, and statistically compared to that of the mucosa covering the spared arytenoid cartilage.
MATERIALS AND METHODS
Thirty-one male patients (age range, 42-74 yrs; median, 62 yrs) were included in this retrospective study. All the patients had a well-differentiated invasive endolaryngeal squamous cell carcinoma that was managed by a SCPL. Resection of the arytenoid cartilage of the tumor bearing side was performed in 14 patients. The findings from the clinical examination performed by nasal fibroscopy, prior to CT imaging, ruled out a local superficial recurrence after surgery. The mean period between the surgical procedure and the CT imaging was 7.8 months (range, 6-12 months).
A postoperative laryngeal CT was performed with a 4 multidetector row CT scanner (Volume Zoom; Siemens, Erlangen, Germany). The scans were taken from the base of skull to the tracheal cartilage using 3-mm-thick contiguous sections after intravenous contrast administration. The patients were put in the supine position with their neck hyperextended and were asked to breathe quietly and avoid swallowing.
The CT appearance of the postoperative neoarytenoid soft tissue was analyzed. On the side of arytenoidectomy, the maximal distance between the superior border of the cricoid cartilage and the mucosal surface of inwardly bulging neoarytenoid soft tissue was measured on an axial image. Similarly, the thickness of the mucosa over the side of the spared arytenoid cartilage was also measured. Lastly, a statistical comparison was drawn between the thickness of neoarytenoid soft tissue and that of mucosa over the spared arytenoid cartilage via the student's t-test with a statistical significance threshold of p < 0.05.
RESULTS
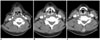
For the 14 sites of arytenoidectomy during the SCPL, the arytenoid cartilage was not observed on postoperative laryngeal CT images. In its place, the arytenoidectomy site appeared as an eccentric thickening of the soft tissue forming neoarytenoid soft tissue (Fig. 1). The thickness of this neoarytenoid soft tissue ranged from 1.4 to 10.3 mm (mean ± standard deviation, 5.66 ± 2.61 mm).
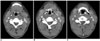
For the 48 preserved arytenoid cartilage sites the arytenoids were identified in at least one sectional image (Figs. 2, 3). Further, the mucosa over the spared arytenoid showed marginal thickening, ranging from 0.6 to 4.1 mm (mean ± standard deviation, 1.90 ± 0.68 mm).
Lastly, the thickness of neoarytenoid soft tissue at the arytenoid cartilage was found to be significantly greater than that of the mucosa covering the spared arytenoid cartilage (p < 0.01).
DISCUSSION
The SCPL technique has been advocated, in selected patients with advanced endolaryngeal cancer, to avoid a total laryngectomy as well as allowing for high rates of local control and survival of selected patients with laryngeal cancer. The SCPL technique is oncologically safe in the setting of glottic and supraglottic cancer without arytenoid fixation (1, 2, 12-16). A unilateral arytenoid cartilage disarticulation and resection is performed at the time of the SCPL procedure in patients with true fixed vocal cords and impaired arytenoid motion (1).
In our series, eccentric neoarytenoid soft tissue prominence was consistently noted on the arytenoidectomy side. Moreover, the thickness of this neoarytenoid soft tissue, measured from the superior surface of the cricoid cartilage, was significantly larger than that of the mucosa covering the spared arytenoid cartilage. If a single arytenoid is resected during the SCPL procedure, the retroarytenoid mucosa should be spared to cover the cricoarytenoid joint area on the cricoid. This spared posterior mucosal flap is elevated and sutured anteriorly and laterally to the transected posterior subglottic mucosa, to create additional mass in the goal of equalizing the heights on both sides. This neoglottic soft tissue promotes neoglottic closure and helps to prevent aspiration during swallowing. However, it can mimic tumor recurrence on the imaging studies as well as on fibroscopy (7).
The CT scan is useful for the detection of submucosal lesions indicated by abnormal thickening. The most common types of tumor recurrence after the SCPL procedure involves an eccentric submucosal extension, which primarily occurs in the cricoid or cricoarytenoid region, and frequently involves masses larger than 10 mm occurring beyond the larynx (10). The thickness of neoarytenoid soft tissue (on the side of arytenoidectomy) in our series did not exceed 11 mm in thickness.
In cases with spared arytenoids, considerable thickening of the mucosa covering the spared arytenoid cartilages have been reported following a horizontal supraglottic or supracricoid partial laryngectomy (7, 10). In addition, hypopharyngeal mucosa, which was sutured to cover the exposed arytenoid cartilage during a partial laryngectomy procedure, may result in excessive soft tissue around the apex of the cartilage. Similarly, scar tissue and healed mucosa over the spared arytenoid may also result in asymmetrical thickening of the mucosal lining of the subglottis (10). In the series reported by Maroldi et al.(10), excessive thickening of the mucosa covering the arytenoid cartilage occurred in 40% of horizontal supraglottic laryngectomy cases and 100% of SCPL cases. In our series, considerable thickening of the mucosa covering the spared arytenoid cartilages were also observed. However, the thickness of mucosa over the spared arytenoid did not exceed 4 mm, which was statistically less than the neoarytenoid soft tissue after an arytenoidectomy. During the SCPL procedure, for cases without an arytenoidectomy, the spared arytenoid is pulled anterolaterally to the posterolateral aspect of the cricoid. This prevents a postoperative backward prolapse of the spared arytenoid. In addition, scar tissue and healed mucosa over the rotated arytenoid cartilage may be seen as eccentric soft tissue prominence on a sectional image. However, there is little chance of mucosal thickening to the extent that a soft tissue mass is formed because the mucosa directly covers the spared arytenoid without forming the posterior mucosal flap, as is the case in neoarytenoid soft tissue after an arytenoidectomy (3, 4).
In conclusion, the neoarytenoid soft tissue can mimic tumor recurrence on the imaging studies as well as on fibroscopy. Consequently, radiologists should be aware of the various surgical techniques for advanced laryngeal cancer as well as the characteristic radiologic findings of the SCPL procedure. Eccentric soft tissue thickening of less than 11 mm in thickness may be noted as neoarytenoid soft tissue on the postoperative CT following an arytenoidectomy during a SCPL. The thickening is consistently larger than the spared mucosa or fibrosis, which is generally less than 4 mm in thickness. These findings should be identified and distinguished from a recurrent tumor on a follow-up CT after a SCPL, with or without an arytenoidectomy.

 XML Download
XML Download