

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Transjugular intrahepatic portosystemic shunt (TIPS) placement is a relatively non-invasive procedure used to relieve portal hypertension and treat variceal bleeding in patients with advanced cirrhosis (1-4). However, TIPS placement is associated with high early mortality when used to control acute variceal hemorrhage, with early mortality rates reported to range from 28% to 36% (5-8).
Existing methods to grade liver function have been developed in non-Asian patients with cirrhosis (8-12), and it is not known to what extent the existing methods can predict mortality in Asian patients with cirrhosis. Three methods commonly used to predict mortality in cirrhosis patients are the acute physiology and chronic health evaluation (APACHE II) (10), Child-Pugh (13) and model for end-stage liver disease (MELD) (14, 15) models. These methods have been developed by the determination of independent risk factors for mortality with large, heterogeneous groups of patients with the development of predictive algorithms based on these risk factors and by testing the algorithms prospectively on other groups of patients. The aim of the current study was to evaluate the prognostic ability of the APACHE II, Child-Pugh and MELD models for short-term (30-day and 60-day) and long-term (360-day) mortality in Taiwanese patients who underwent an emergent TIPS procedure due to uncontrolled variceal bleeding.
MATERIALS AND METHODS
Patient Population
From August 1995 to December 2006, 107 consecutive patients (74 males, 33 females; mean age, 56 years), who underwent an emergent TIPS procedure for uncontrolled variceal hemorrhage were enrolled in the study. Emergency indications for the TIPS procedure were defined as a patient requiring blood products within 24 hours of TIPS creation, hemodynamic instability, balloon tamponade or obvious continued bleeding (16). In general, patients underwent an emergency TIPS procedure at our institution after the failure of other available therapies (e.g. blood transfusion, pharmacological management, balloon tamponade and endoscopic treatment). All cases were evaluated and were initially treated endoscopically. If available treatments were unsuccessful, the clinical condition of patients was stabilized with blood transfusion, pharmacological therapy and/or balloon tamponade, and a TIPS procedure was performed immediately after obtaining patient informed consent. Antibiotics were administered when there were signs or evidence of infection such as fever or leukocytosis, suspicion of aspiration pneumonia or evidence of other infectious conditions such as spontaneous bacterial peritonitis (SBP). This study was approved by our Institutional Review Board.
Data Collection
Clinical and laboratory data were collected retrospectively from the Hospital Information System database and through a review of medical records. Data abstracted included the presence of ascites, encephalopathy, SBP, bacteremia, hepatorenal syndrome and other disease or infection. The need for mechanical ventilation or inotropic support was noted, as was the number of units of blood transfused before the TIPS procedure. Portal and central venous pressure levels and the portal-systemic pressure gradient (PSG) were also recorded. Laboratory values analyzed included hemoglobin level, hematocrit, white blood cell (WBC) count, platelet count, prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (APTT), serum creatinine level, blood urea nitrogen (BUN), serum albumin level, total bilirubin level, glutamic-oxaloacetic transaminase level, glutamic-pyruvic transaminase level and levels of serum sodium, potassium and chloride. APACHE II (10), Child-Pugh (13) and MELD (14, 15) scores were calculated for all patients.
The criteria used to grade hepatic encephalopathy were based on the West Haven classification scale. Diagnosis of hepatorenal syndrome was based on a finding of a reduced glomerular filtration rate in the absence of other causes of renal failure in patients with chronic liver disease. SBP was defined as an absolute neutrophil count in the ascitic fluid of ≥ 250/mm3 in the absence of a surgically treatable, intra-abdominal source of infection. Ascites was graded as: 1) none: no ascites; 2) mild: ascites detected only on ultrasound; 3) moderate: shifting dullness; 4) severe: tense abdomen.
Transjugular Intrahepatic Portosystemic Shunt Procedure
Transjugular intrahepatic portosystemic shunt procedures were performed using techniques described elsewhere (3) and summarized here. Under local anesthesia, the right (or left) hepatic vein was selectively catheterized with a 40 cm-long 9 Fr sheath using a right internal jugular venous approach. A parenchymal tract between the hepatic and portal veins was created with a 16-gauge Colapinto needle (Cook, Bloomington, IN) under fluoroscopic guidance. After entry into the portal vein, a guide wire, followed by a 4 Fr angiocatheter, was advanced through the parenchymal tract into the portal venous system. Splenic (or superior mesenteric) venography was performed. Portal venous pressure was measured through the angiocatheter and central venous pressure was measured from the side-arm of the 9 Fr introducer sheath. The parenchymal tract between the hepatic and portal veins was dilated with an 8 mm diameter angioplastic balloon catheter. A 10 mm in diameter Wallstent endoprosthesis (Schneider, Minneapolis, MN) was deployed in the tract to support the parenchymal channel. This stent can be opened from 8 mm to 12 mm; the size is decided by the largest balloon that is used. In order to achieve an ideal PSG lower than 15 mmHg, it is sometimes necessary to dilate the tract of the TIPS to 12 mm. A higher gradient was used as the therapeutic target as all cases were medical emergencies and the use of a lower gradient might have increased the risk of liver failure. Transcatheteral embolization was performed to fill the residual varices with metallic coils or tissue adhesive (Histoacryl; B. Braun, Melsungen, Germany). All patients were transferred to the intensive care unit (ICU) for monitoring. Before patient discharge, Doppler ultrasonography was performed to confirm shunt patency. If portal vein thrombosis was present, the portal vein was recanalized.
If hemostasis was achieved after the TIPS procedure, a baseline Doppler ultrasound study was performed before the patient was discharged. A follow-up ultrasound examination was performed at three-month intervals during the first year and every six months thereafter. If there were ultrasound signs of shunt obstruction, follow-up portography via the shunt was performed. Dilatation of the shunt or placement of an additional metallic stent was performed during the follow-up intervention. If portal vein thrombosis was identified on an ultrasound or CT scan before the TIPS procedure, the patent or partially patent portion of the intrahepatic portal vein was punctured from the hepatic vein and then catheterized through the thrombosed area of the portal vein to the splenic vein or superior mesenteric vein under fluoroscopic guidance. After dilatation of the tract of the TIPS and thrombosed portal vein, the metallic stent was placed continuously from the hepatic vein through the TIPS tract to the main portal vein or sometimes to the splenic vein or superior mesentery vein to produce a patent TIPS tract.
Statistical Analysis
Survival analyses were performed to evaluate the ability of APACHE II, Child-Pugh and MELD scores to predict 30-day, 60-day and 360-day mortality. The survival period was defined as the duration between TIPS placement and death, or TIPS placement and the last follow-up contact. Kaplan-Meier analysis with the use of the log-rank test was performed to assess the ability of stratified APACHE II, Child-Pugh and MELD scores to predict survival. Scores were evenly divided into first, second or third tertiles. Tertiles were utilized in the analyses to avoid assumptions regarding linearity and to maximize statistical power.
A Cox proportional hazard model was applied for both univariate and multivariate analyses. Univariate Cox regressions were used to evaluate the crude effect of each demographic characteristic, laboratory examination and clinical feature for 30-day, 60-day and 360-day mortality. Based on a literature review, well-known risk factors for the prediction of mortality among patients with acute variceal bleeding who underwent the TIPS procedure were added to the multivariate models. Other variables found to be significant by univariate analysis were considered as candidate confounding factors for constructing multivariate models. The three prognostic scores (APACHE II, Child-Pugh and MELD) were evaluated as ways to predict mortality. Hazard ratios with 95% confidence intervals (CI) were estimated for each prognostic scoring system. Statistical analyses were performed with SPSS 15.0 for Windows (SPSS, Chicago, IL), with the significance level set at 0.05.
Multiple receiver operator characteristic (ROC) curves for each scoring system were estimated and C-statistics (equivalent to the area under ROC curve) with 95% CI were calculated to compare the validity of the three indices. For pairwise comparison of ROC curves, MedCalc for Windows, version 9.38 (MedCalc Software, Mariakerke, Belgium) was used.
RESULTS
Patient Demographics
A total of 107 patients were enrolled in this study. The period between acute variceal hemorrhage and TIPS placement varied greatly (mean, 19.2 ± 68.9 hours), but this time period was not used in later calculations as there was uncertainty in some cases.
Baseline characteristics of the participants are shown in Table 1. The majority of patients had viral hepatitis (n = 73, 68%). After TIPS placement, the average portal venous pressure decreased from 32.84 to 21.12 mmHg (p < 0.001) and the PSG decreased from 26.96 to 11.27 mmHg (p < 0.001).
For 38 patients who were subjected to follow-up for more than six months, shunt dysfunction was identified in 12 patients and 16 sessions of re-intervention with placement of additional stents were performed.
Survival Analysis
No patient died during the TIPS procedure, but 82 (77%) patients died during the follow-up period. Thirty (28%) patients died within 30 days, 37 (35%) patients died within 60 days and 53 (50%) patients died within 360 days. Causes of death included hypovolemic shock (nine patients), hepatic failure (31 patients), septic shock (29 patients), respiratory failure (eight patients), renal failure (one patient) and other causes (four patients).
As shown in Table 2, univariate analysis demonstrated that mortality after 30, 60 and 360 days increased significantly with increasing laboratory values for the creatinine level, PT, INR, APTT, BUN, WBC count and pre-TIPS placement and post-TIPS placement portal and central venous pressure levels (p < 0.05). Decreasing levels of albumin and hemoglobin and a decreased hematocrit were also associated with increased 30-day mortality (p < 0.05). Patients with encephalopathy or hepatorenal syndrome, or who received mechanical ventilation or inotropic agents had a worse prognosis (p < 0.05).
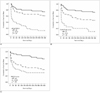
For 30-day survival, patients in the first (< 13) and second (13-17) APACHE II tertiles had similar survival rates, but patients in the third tertile (> 17) had poor survival (log-rank test, p < 0.001). The three Child-Pugh tertiles (< 9, 9-11 and > 11) showed a significant difference in survival (log-rank test, p < 0.001). Patients in the first (< 15) and second (15-20) MELD tertiles had similar survival rates, but overall survival was worse in the third (> 20) tertile (log-rank test, p < 0.001). For 60-day and 360-day survival, the survival rate differed among tertiles for APACHE II (Fig. 1A), Child-Pugh (Fig. 1B) and MELD (Fig. 1C) scores, with all differences significant (log-rank test, all p < 0.001).
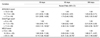
The hazard ratios for survival using the three scoring systems are shown in Table 3. Patients with APACHE II scores > 17 had a three-fold higher risk of mortality at 360 days as compared to patients with APACHE II scores < 17 (p < 0.05). Patients with Child-Pugh scores > 11 had an approximately four-fold to six-fold higher risk of mortality at all time points as compared to patients with Child-Pugh scores < 9 (p < 0.05). Patients with MELD scores > 20 had an approximately four-fold to eight-fold higher risk of mortality at all time points as compared to patients with MELD scores < 15 (p < 0.05).
DISCUSSION
Existing scoring systems that are used to predict patient mortality after TIPS placement, including the APACHE II, Child-Pugh and MELD, were derived largely in non-Asian patient populations. Our results suggest that when these models are used for Taiwanese patients, the prediction of mortality is less than optimal. All of the scoring systems were able to predict mortality to some extent, but the APACHE II score was only useful to predict mortality at 360 days. Both the Child-Pugh and the MELD scores could predict mortality at 30 days, 60 days and 360 days, with the MELD score performing marginally better as compared to the Child-Pugh score, based on the hazard ratio of patients in the highest risk tertile. However, all of the current grading schemes leave room for improvement as demonstrated in this population of Taiwanese patients.
Univariate analysis of 15 different factors was performed and found all factors to be related to 30-day mortality. Other studies of 30-day mortality after emergency TIPS placement have also shown many risk factors determined by the use of univariate analysis (10-12, 16). The most consistently reported risk factors are the bilirubin level, PT (or some other measure of bleeding time) and the need for ventilator support. Our results largely concur with these findings. The study (16), in which population was most similar to ours (30-day mortality after TIPS placement for acute bleeding varices in patients with virally-caused cirrhosis) showed agreement with our findings for three risk factors: creatinine level, albumin level and PT. Final univariate analyses indicated that hepatorenal syndrome, use of inotropic agents and mechanical ventilation were associated with elevated 30-day mortality (all p < 0.05).
Prediction of mortality was roughly equivalent for the three scoring systems according to the C-statistic analysis of predictive power. The C-statistic for the three scoring systems to predict 30-day, 60-day and 360-day mortality were 0.81, 0.75 and 0.78 for the APACHE II scores, 0.74, 0.71 and 0.73 for the Child-Pugh scores and 0.78, 0.78 and 0.74 for the MELD scores, respectively. In general, a C-statistic of 0.8 to 0.9 indicates excellent predictive accuracy while a C-statistic of 0.7 to 0.8 is acceptable. By the use of these criteria, our results suggest that the APACHE II and MELD systems may be somewhat better than the Child-Pugh classification for our patients. However, there were no significant differences between the scoring systems for pair-wise comparisons. Three other studies, all of elective patients that had undergone the TIPS procedure, have compared the predictive power between the use of MELD and Child-Pugh scores (14-17). In one study, which did not use C-statistics, the MELD but not the Child-Pugh score was significantly better to predict survival and three-month mortality (14). In a second study, C-statistics showed that MELD (0.71) and Child-Pugh (0.72) scores had similar predictive power for three-month mortality (15). A third study reported similar C-statistics for MELD (0.73) and Child-Pugh (0.78) scores for 30-day mortality (17).
Differences in the predictive ability between the scoring systems could arise for a number of reasons. The APACHE II system emphasizes general physical health; it was standardized for ICU patients and was intended to predict early mortality risk for ICU patients. Only one item is specific to liver disease and liver disease severity is recorded indirectly, as it affects physiological measurements. The MELD model uses three laboratory test values and an empirically developed algorithm derived from these values. The goal of the MELD model is to avoid subjective judgment and to give greater weight to extremely abnormal laboratory values. The Child-Pugh model includes two measurements of the impact of liver function on other systems, namely ascites and encephalopathy, in addition to three laboratory values of liver function. In addition, the Child-Pugh model is considered easy to use as the model uses a point system for scoring.
A limitation of this study is that it was retrospective, with the risk of data misinterpretation. Another limitation is that we were unable to determine which patients received beta-blocker therapy, an intervention that could have affected the portovenous gradient.
In summary, our results show that a Child-Pugh score > 11 or an MELD score > 20 are predictive of 30-day, 60-day and 360-day mortality in Asian patients with refractory variceal hemorrhage treated with the TIPS procedure. The APACHE II score is not predictive of early mortality in this patient population.




 XML Download
XML Download