

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In terms of the diagnostic evaluation of neonates with an imperforate anus (IA), the primary goal is the differentiation of IA type, as this information is required to determine the correct type of surgery. The position of the distal rectal pouch with respect to the puborectalis sling of the levator ani muscle is a critical factor when considering whether an IA is of the high-type, intermediate-type or low type, i.e., above the sling (high or supralevator), at the sling (intermediate), and through the sling (low or infralevater). High and intermediate IA types are treated using a two-stage surgical approach, with an early diverting colostomy followed by a "pull-through operation," whereas low type IAs are treated by perineal anaplasty shortly after birth.
Of the various preoperative modalities, transperineal ultrasonography (US) has been used to determine the IA type and to search for an associated internal fistula (1-4). Previously, the differentiation of a low-type from a high-type IA had been performed indirectly by measuring the distance from the distal rectal pouch to the perineum (1, 4). However, recent improvement in US resolution has facilitated the identification and determination of location of internal fistulas with the use of transperineal US (3).
The purpose of this study was to assess the usefulness of transperineal US to determine the IA type.
MATERIALS AND METHODS
We reviewed medical records at Seoul National University Children's Hospital from January 2000 to December 2004 and identified 193 infants with a diagnosis of IA that underwent surgical treatment. Of these infants, 46 infants that underwent transperineal US prior to corrective surgery were included in the study population. The mean patient age at the time of diagnosis was 3.5 months (age range, 1 day to 12 months). The study population consisted of 30 males and 16 females. The Institutional Review Board of Seoul National University Children's Hospital approved this retrospective study and waived the requirement for informed consent.
Transperineal US was performed by one of four board certified diagnostic radiologists using a 5-15 MHz linear transducer with the patient in a modified lithotomy position. A thick layer of gel was applied over the perineum to prevent artifacts due to the presence of intervening air. An US transducer was placed in the midsagittal plane through the perineum. In this plane, the pubic synchondrosis, posterior urethra, anterior rectal wall and the bladder base, and in girls, the vaginal region between the urethra and rectum could be appreciated (Fig. 1). In all of the 46 infants, interpretable midsagittal scans were obtained.
Two radiologists with 20 and four years of clinical experience, respectively, retrospectively reviewed the US images by consensus on a 2000 × 2000 Picture Archiving and Communication Systems monitor (PACS; Marotech, Seoul, Korea). During the review process, the observers were unaware of the surgical, physical and other imaging findings.
First, internal fistula types were determined. On transperineal US images, an internal fistula was defined as a hypoechoic linear tract, sometimes possessing an internal echogenic line due to the presence of intervening air within the fistula. These hypoechoic tracts course anteriorly, interrupting the echogenic fat plane between the rectum and urethra (vagina or bladder) (Fig. 1).
Second, the shortest distance between the distal rectal pouch and the perineum was measured in each infant. A scatterplot of "pouch to perineum (P-P)" distances was constructed versus surgically proven IA types. The mean P-P distance and range were calculated and optimal threshold P-P distances to discriminate between a high-type IA and a low-type IA were determined using a scatterplot.
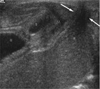
Third, the IA type was determined by considering the fistula type and P-P distance. The International Classification of 1970 was used to match IA type and fistula (5). In male infants, an IA with 1) a recto-vesical fistula or 2) a recto-prostatic urethral fistula was classified as the high-type. An IA with a recto-bulbar urethral fistula was classified as an intermediate-type. An IA with an anocutaneous fistula was classified as a low-type. In female infants, an IA with a recto-upper vaginal fistula was classified as a high-type. An IA with 1) a recto-vestibular fistula (where the fistula opened at the vestibule of the vagina and the narrow fistular tract coursed cephalad up to the level of the levator) or 2) a recto-lower vaginal fistula was classified as intermediate-type. An IA with 1) an anovestibular fistula (a fistular opening that presented in the vestibule and where the fistula connected with the vestibule and the distal rectal pouch, located below the level of the levator) or 2) an anocutaneous fistula was classified as a low-type. Anal stenosis and a thickened skin-covered anus were classified as low-type IAs (Fig. 2). In cases of an IA with an indeterminate internal fistula, the P-P distance was taken into consideration. Threshold P-P distances previously determined were used to discriminate between high-type and low-type IAs.
In all patients, surgical and radiological examination findings obtained using distal loopography or voiding cystourethrography were viewed as reference standards. The diagnostic accuracies of transperineal US to determine IA type were evaluated by comparing US findings with reference standards.
RESULTS
Surgical Findings
Of the 46 IA cases enrolled this study, 17 cases were confirmed as high-type IAs, three cases were confirmed as intermediate-type IAs and 26 cases were confirmed as low-type IAs. Fourteen of the 17 high-type IA cases had a recto-prostatic urethral fistula and the other three cases had a recto-vesical fistula. Two cases of an intermediate-type IA had a recto-bulbar urethral fistula. One case of an intermediate-type IA had anal agenesis without a fistula. Nineteen cases of a low-type IA had an anovestibular fistula (n = 11) or an anocutaneous fistula (n = 8). Seven cases had no fistula, and were confirmed as having anal stenosis or an anomalous membrane obstruction.
US Identification of Internal Fistulas
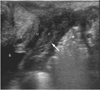
All 14 cases of recto-prostatic urethral fistulas were correctly identified by the use of transperineal US (Fig. 3). However, fistula tracts were not demonstrated in all three recto-vesical fistula cases. Of the 17 high-type fistula cases, 14 cases were correctly demonstrated (14 of 17, sensitivity 82%). For intermediate-type IAs, one of two recto-bulbar urethral fistulas was demonstrated (Fig. 4). Among the 19 cases of a low-type IA with an anovestibular or anocutaneous fistula, 13 cases of an anocutaneous or anovestibular fistula were correctly identified (13 of 19, sensitivity 68%) (Fig. 5). Two cases of anocutaneous fistulas were misdiagnosed as recto-prostatic urethral fistulas due to apparent anterior beaking of the distal rectal pouch. For the other four cases of low-type IAs with fistulas (three anocutaneous fistulas and one anovestibular fistula), no fistula tract was demonstrated by the use of transperineal US.
"Pouch to Perineum" Distances
A scatterplot of P-P distances was constructed versus the IA type (Fig. 6). The mean P-P distances for high, intermediate and low-type IAs were 18.2 mm (range, 6-30 mm), 11 mm (range, 6-16 mm) and 5.3 mm (range, 0-14 mm), respectively. Some overlap in P-P distances was observed among the IA types, but all patients with a P-P distance > 16 mm had a high type IA and all patients with a P-P distance < 5 mm had a low type IA (Fig. 6).
US Determination of Imperforate Anus Type
Among 17 cases of high-type IA, 15 cases were correctly determined as high-type IAs (15 of 17, sensitivity 88%) and 14 cases were diagnosed as high-type IAs due to the identification of a recto-prostatic urethral fistula (Fig. 3). One case of an IA with a recto-vesical fistula, where a fistula tract was not demonstrated was diagnosed as a high-type based on the P-P distance (19 mm). In the other two high-type IAs with a recto-vesical fistula, no fistula tract or distal rectal pouch was demonstrated due to poor transperineal US tissue penetration, and the two cases remained undetermined.
For intermediate-type IAs, only one case was correctly diagnosed as an intermediate-type by demonstrating the presence of a recto-bulbar urethral fistula (Fig. 4). The other two cases remained undetermined due to a non-visualized fistula tract and indeterminate P-P distances (6 mm and 11 mm, respectively).
Of the 26 cases of low-type IAs, 23 cases were correctly diagnosed as low-type IAs (23 of 26, sensitivity 88%). Thirteen cases of low-type IAs were correctly determined by identifying anocutaneous or anovestibular fistulas (Fig. 5) and the other 10 cases were correctly diagnosed as low-type IAs due to a short P-P distance (< 5 mm), even though the fistula tract was not demonstrated on US. Two cases of low-type IAs with an anocutaneous fistula were misdiagnosed as high-type IAs with a recto-prostatic urethral fistula. Only one low-type IA was undetermined due to an invisible fistula tract and an indeterminate P-P distance (7 mm).
Overall, the IA type was correctly diagnosed by the use of transperineal US in 39 of the 46 study subjects (85%).
DISCUSSION
An IA is a relatively common anomaly, which occurs in approximately one of 500 live births, with a slight predilection for male infants (5). An IA is classified according to the International Classification of 1970 and the proposed "Wingspread" modification of 1986 as a high-type, intermediate-type and low-type (5, 6). These classifications are based on the level of the distal rectal pouch relative to the puborectalis sling of the levator ani muscle. The differentiation of IA types is critical to determine surgical treatment and to predict continence. Various radiological modalities have been used to determine the level of the distal pouch in infants with IA. The modalities include inverted lateral radiography (invertography), distal colostography (loopography), US, CT and MRI (1, 4, 7-11). The role of the use of a preoperative radiological modality for IA is to determine the level of the distal rectal pouch, to identify the presence and location of internal fistulas and to diagnose any associated anomalies.
Conventional transperineal US is both rapid and straight-forward to perform and US is not associated with any radiation hazard. Previously, differentiation of low-type and high-type IAs with the use of US had been indirectly performed by measurement of the distance between the distal rectal pouch and the perineum (1, 4). However, the use of this method has been limited by measurement overlaps between high and low-type IAs and with variable cut-off points among studies. Donaldson et al. (1) have reported that a P-P distance of 1.0 cm or less is suggestive of a low-type IA and a P-P distance of 1.5 cm or greater is suggestive of a high-type IA. Oppenheimer et al. (4) have stated that a P-P distance of less than 1.5 cm is consistent with a low-type IA. In our study, different cut-off values were obtained and some overlap in P-P distances was observed among IA types. Such discrepancies in P-P distance measurement might be caused by varying degrees of pouch distension, pressure on the perineum by the probe and may be related to the age of the infant at the time that the examination is performed.
Accurate preoperative identification of an internal fistula between the distal pouch and the urogenital tract is very important for optimal surgical management and prevention of a potential injury to the genitourinary tract. In addition, the IA type can be determined based on the internal fistular type. With recent improvements in US resolution, transperineal US has become an excellent diagnostic modality to define the type of the internal fistula for an IA (3). Our study results have also demonstrated good performance for the use of transperineal US. Of the 38 cases with fistulas, 28 fistulas were correctly identified by the use of transperineal US. Only three recto-vesical fistulas and one recto-bulbar urethral fistula with a very high location could not be demonstrated due to poor sonic penetration. But, of 19 anovestibular or anocutaneous fistulas of the low-type, only 13 cases were visualized by transperineal US, because the low-type fistula tracts were shallow and short. However, as low-type fistulas such as anocutaneous or anovestibular fistulas can be easily determined on a clinical examination, this low detection rate of US for low-type fistulas is not of clinical concern.
Lastly, we considered two sonographic findings in combination (the fistula type and P-P distance) and we attempted to use these findings to determine the IA type. The IA type was correctly diagnosed by the use of transperineal US alone in 39 of the 46 patients (85%). If physical examination findings had been taken into consideration, the diagnostic accuracy of transperineal US would have increased. Considering the easy accessibility, good performance and the lack of any radiation hazard, transperineal US can be performed as an initial modality to determine the type of IA and to determine the type of early surgical management.
In the present study, a female cloacal anomaly was not included as this anomaly can be determined by inspection of the perineum alone. Females with only a single opening on the perineum and no visible hymen must have a cloacal anomaly, which is indicative of a high-type anomaly, which obviates the need for a US examination to determine type.
In conclusion, our study results show that transperineal US is a good modality to define the internal fistula type and to predict the IA type based on consideration of the fistula type and P-P distance.




 XML Download
XML Download