

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Gadobenate dimeglumine (gadolinium-benzyloxypropionictetraacetate [BOPTA], MultiHance; Bracco Imaging, Milan, Italy) can be used not only as a non-specific extracellular contrast agent for dynamic imaging of the liver, but also as a liver-specific agent for the acquisition of hepatobiliary-phase images (1-4). Therefore, gadobenate dimeglumine-enhanced magnetic resonance (MR) imaging simultaneously provides both morphological and functional information.
In general, lesions that contain functioning hepatocytes where hepatobiliary metabolism is mostly unaltered may be expected to uptake gadobenate dimeglumine in the same manner as normal hepatocytes and the lesions may be expected to excrete the compound into the bile. Such lesions are typically benign and usually appear isointense or hyperintense as compared to the normal liver parenchyma as depicted on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging. In contrast, lesions that do not contain functioning hepatocytes where hepatobiliary metabolism is blocked or inhibited are generally not able to uptake and excrete gadobenate dimeglumine into the bile. Such lesions are typically malignant and usually appear hypointense as compared to the normal liver parenchyma as depicted on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging (4-11). However, some benign lesions may be hypointense as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging and may be mistaken for hepatic malignancies, resulting in unnecessary performance of an interventional procedure such as a biopsy or surgery (4-13).
In this pictorial essay, we describe the mechanism of enhancement of gadobenate dimeglumine in the liver as seen on hepatobiliary-phase MR imaging. In addition, we will present various pathologically proven benign and malignant hypointense hepatic lesions as depicted on gadobenate dimeglumine-enhanced three-hour delayed hepatobiliary-phase MR imaging, with an emphasis on the differential diagnosis between benignancy and malignancy.
Mechanism of Hepatic Uptake and Biliary Excretion of Gadobenate Dimeglumine
Gadobenate dimeglumine is a gadolinium-based contrast agent, which possesses a two-fold greater T1 relaxivity as compared to conventional gadolinium-based agents in human plasma, due to a weak and transient interaction with serum albumin (1, 2). Gadobenate dimeglumine undergoes elimination from the body through both a renal (95-97% of the injected dose) and hepatobiliary pathway (2, 3). Approximately 3-5% of the injected dose is taken up into the functioning hepatocytes through the action of organic anion transporting peptide 1 and the compound is eliminated into the bile by the adenosine triphosphate (ATP)-dependent canalicular multispecific organic anion transporter peptide (cMOAT), multidrug resistance-associated protein 2 (Mrp2) that transports bilirubin (Fig. 1) (14-18).
Hepatobiliary-Phase MR Imaging of Gadobenate Dimeglumine
It is known that as seen on gadopentetate dimeglumine (Gd-DTPA)-enhanced 1-hour to 4-hour delayed MR imaging, the area with delayed enhancement corresponds pathologically to abundant fibrosis, the hypointense rim corresponds to rich tumoral cellularity and the hypointense center corresponds to coagulative necrosis (19). The enhancement of focal hepatic lesions as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging is affected by the internal component of the lesions such as the sinusoid-like vascular space or fibrosis, which is similar to the enhancement mechanism of Gd-DTPA. The enhancement of focal hepatic lesions is also affected by the retained hepatocyte activity of the lesion, which is unique as compared with the effect of Gd-DTPA (6, 19, 20). Appropriate gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging can be performed from 40 minutes after the injection of the contrast agent and the strong enhancement of normal liver parenchyma is maintained for a period of 120 minutes or longer (2, 18). In our institute, hepatobiliary-phase MR imaging has been obtained three hours after the injection of gadobenate dimeglumine for the minimization of the extracellular effects of the contrast agent.
Benign Hypointense Hepatic Lesions
A variety of benign hepatic lesions can appear hypointense as depicted on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging due to the following causes. (a) No functioning hepatocytes are present in the lesion, (b) damage to the functioning hepatocytes has occurred due to infection or inflammation and (c) impairment of biliary function in the lesion has occurred (4-13).
No Functioning Hepatocytes
Cysts and Hemangiomas
Cysts (Fig. 2) and hemangiomas (Fig. 3) are the most common benign lesions in the liver that lack functioning hepatocytes (5, 6). The differentiation of these lesions from other malignant hypointense hepatic lesions is possible with the use of unenhanced and gadobenate dimeglumine-enhanced dynamic MR imaging.
Mesenchymal Tumors
A variety of mesenchymal tumors of the liver with no functioning hepatocytes including angiomyolipomas and solitary fibrous tumors can appear as hypointense as depicted on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging; the appearance of these lesions may mimic a malignant tumor. We have experienced a rare mesenchymal tumor (21, 22), a hypointense solitary fibrous tumor with a clear margin (Fig. 4) as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging, which mimicked a malignant tumor.
Miscellaneous
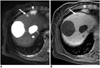
We have experienced a reactive lymphoid hyperplasia (Fig. 5) in the liver that is a rare benign nodular lesion characterized by marked proliferation of non-neoplastic, polyclonal lymphocytes that form follicles with an active germinal center (23, 24). This nodule appeared hypointense with a clear margin as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging and mimicked a malignant tumor.
Damage of Functioning Hepatocytes
Focal Eosinophilic Liver Disease
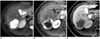
Focal eosinophilic liver lesions including focal eosinophilic infiltration, eosinophilic abscess and granuloma (Fig. 6) are composed of inflammatory cell infiltration with a large proportion of eosinophils with or without coagulation necrosis (25-27). Imaging findings of focal eosinophilic liver disease as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging depend on the degree of inflammation and the destruction of the liver parenchyma. The peripheral portion of an eosinophilic focal lesion may show retention of the contrast agent due to inflammation as compared with the central necrotic portion, which may result in the depiction of a fuzzy margin due to peripheral isointensity or hyperintensity relative to the center (Fig. 6).
Infectious Lesions
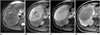
With the use of gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging, imaging findings of inflammatory lesions (Fig. 7) such as hepatic abscesses may vary depending on the difference in the degree of inflammation and destroyed hepatic parenchyma (11, 13). The presence of peripheral isointensity or hyperintensity of an inflammatory lesion may be mainly due to the retention of the contrast agent in fibrous tissues, from an inflammatory change due to extensive fibrosis as relative to the hypointensity (necrosis) of the center, and may suggest that the lesion is not typically malignant in nature.
Impaired Biliary Function
Hepatic Adenomas
Although a hepatic adenoma (Fig. 8) has functioning hepatocytes, it lacks bile ducts (7, 8, 28). Therefore, it is likely that the hepatocellular bilirubin metabolism is blocked in the adenoma, as confirmed by the absence of bile in a resected adenoma (28), which results in the absence of uptake and transport of gadobenate dimeglumine. As seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging, an adenoma appears as a hypointense lesion. Although not always helpful, for the successful differential diagnosis of hepatic adenomas from other malignant hypointense hepatic lesions, especially hepatocellular carcinomas, the use of unenhanced and gadobenate dimeglumine-enhanced dynamic MR imaging may be complementary.
Dysplastic Nodules
Dysplastic nodules usually appear isointense as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging (9, 10). The biliary function of a low-grade dysplastic nodule is usually preserved and bile ducts are present in portal areas. In a high-grade dysplastic nodule, the biliary function may only be partially impaired, in which portal triads may be focally absent in the nodule and thus bile ducts may be missing (4). Although confirmation of the presence of the tumor after performing a needle biopsy is not always sufficient to eliminate the need for a histological examination of the entire tumor after resection (Fig. 9), uptake and transport of gadobenate dimeglumine may be impaired in a dysplastic nodule.
Malignant Hypointense Hepatic Lesions
Malignant lesions such as advanced hepatocellular carcinomas (Fig. 10), cholangiocarcinomas (Fig. 11) and metastases (Fig. 12) do not contain functioning hepatocytes and thus cannot retain gadobenate dimeglumine. These lesions appear hypointense as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging (4-6, 9, 30).
Malignant hepatic lesions tend to outgrow their blood supply, producing central necrosis, hemorrhage and fibrosis, which results in the depiction of various imaging patterns on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging. A target appearance that is defined as peripheral hypointensity relative to the center (6, 20) may appear in a malignant mass with abundant fibrosis such as a cholangiocarcinoma and a metastasis. The pathological features may explain the target appearance, where the majority of stromal fibrosis is in the center of the lesions, resulting in the retention of gadobenate dimeglumine in the center. More abundant tumoral cellularity is observed in the periphery of the lesion, resulting in rim-like hypointensity to the center, which may be similar to the enhancement mechanism of the target appearance by Gd-DTPA (29, 30). The target appearance appears to be more conspicuous on Gd-DTPA-enhanced hepatobiliary-phase images than Gd-DTPA-enhanced delayed images due to the marked and prolonged enhancement of the normal liver parenchyma as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase images.
In conclusion, gadobenate dimeglumine has a property of being a unique liver-specific contrast agent in addition to a property of being an extracellular contrast agent, which results in the marked and prolonged enhancement of the normal liver parenchyma up to three hours after the administration of the contrast agent with intralesional enhancement. Based on these features, three-hour delayed hepatobiliary-phase MR imaging may be helpful in the characterization of focal liver lesions. Both benign and malignant hepatic lesions may appear hypointense as seen on gadobenate dimeglumine-enhanced hepatobiliary-phase MR imaging. Benign hypointense hepatic lesions as seen on hepatobiliary-phase imaging alone may be mistaken for hepatic malignancies, resulting in the performance of an unnecessary biopsy or surgery. As seen on three-hour delayed hepatobiliary-phase imaging, peripheral iso/hyperintensity due to fibrotic tissue compared to the hypointense center with a fuzzy margin may be a clue of the presence of a benign hepatic lesion. In contrast, peripheral hypointensity due to rich tumoral cellularity compared to the center with a clear margin may favor the presence of a malignant hepatic lesion.









 XML Download
XML Download