

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fecal tagging is labeling of fecal residue in the colon by oral ingestion of a small amount of positive contrast material as part of the preparation prior to CT colonography (CTC) (1). The use of fecal tagging improves the differentiation of residual feces from polyps and thereby false-positives can be avoided. Fecal tagging also offers the opportunity to reduce the extent of cathartic cleansing for CTC and therefore can improve patient compliance (2). Reduction of the discomfort of purgative bowel cleansing before CTC is a substantial advantage for patients as studies have shown that bowel cleansing represented the most unpleasant part of colonic examinations (3, 4). Given the importance, fecal tagging is becoming widely accepted as a standard procedure for CTC.
Different tagging methods, including various densities of barium, water-soluble iodinated contrast agents and combinations have been previously evaluated (2, 5-14). Of these methods, barium-based fecal tagging (2) has been particularly widely adopted due to cost-effectiveness, safety and commercial availability. Most studies regarding the effectiveness of fecal tagging and optimal tagging methods have been performed in Western populations with Western diets. However, the effectiveness of fecal tagging and optimal tagging methods may possibly vary according to the dietary habits of different ethnic groups. To the best of our knowledge, there have been no published studies about the efficacy of fecal tagging or optimal fecal tagging methods in a population from South Korea, even though commercial fecal tagging agents are already available in South Korea. There have been a few clinical studies with CTC conducted in Korean patients where fecal tagging was used in a subgroup of the patients; however, the efficacy of fecal tagging was not specifically addressed in the studies (15, 16).
The purpose of this preliminary study was to determine and to compare the efficacy of two commercially available barium-based fecal tagging agents for CTC (high-density [40% w/v] and low-density [4.6% w/v] barium suspensions) in a population from Korea by using the rate of complete fecal tagging as the primary outcome measure.
MATERIALS AND METHODS
The institutional review board approved this study and informed consent was obtained from all of the participants.
Study Patients
From March 2006 to July 2006, 30 asymptomatic adults with an average-risk for colorectal cancer were recruited for this study. The participants were selected from subjects who were scheduled for colorectal screening at our institution. Subjects were excluded who had undergone colorectal imaging (including sigmoidoscopy, colonoscopy, CTC or a barium enema) within the prior five years, subjects with a history of colorectal disease or surgery, subjects with symptoms of lower gastrointestinal tract disease and subjects with a first-degree relative that was diagnosed with colorectal cancer. The first set of 15 patients (group I) were assigned to undergo fecal tagging with use of a 40% w/v barium suspension (Tagitol V; E-Z-EM, Westbury, NY). The second set of 15 patients (group II) were assigned were assigned to undergo fecal tagging with use of a 4.6% w/v barium suspension (Easy CT 4.6; Taejoon Pharmaceuticals, Seoul, Korea).
Bowel Preparation and Fecal Tagging
Bowel preparation for CTC started two days before the examination. The patients were requested to refrain from foods that were rich in fiber (such as pickled or fermented cabbage or radishes, e.g. kimchi (17), bean sprouts, lettuce or garlic), seeded fruits (such as grapes, watermelon or other types of melon) and seaweed. The day before the CTC examination, the patients were instructed to eat rice porridge at breakfast, lunch, and dinner, with the ingestion of the barium suspensions at the end of each meal. For the group I patients, three doses (each dose at the end of each meal) of 20 mL 40% w/v barium suspension were administered. For the group II patients, three doses of 200 mL 4.6% w/v barium suspension were administered. Each tagging protocol resulted in a total barium load of 24 g and 27.6 g in group I and group II patients, respectively. Colonic purgation was performed using the same protocol in both group I and group II patients in the evening prior to the CTC examination by the administration of 19.2 g magnesium citrate in the form of a 250 mL solution (Magcorol Solution; Taejoon Pharmaceuticals) and 20 mg of bisacodyl (Dulcolax; Boehringer Ingelheim, Seoul, Korea).
CT Colonography Scanning
A small catheter with a retention cuff (PROTOCO2L administration set; E-Z-EM) was placed in the rectum with the patient in the left lateral decubitus position by a dedicated CT technologist. After inflation of the retention cuff, the cuff it was gently pulled back until its proximal end rested on the anal sphincter. Colonic insufflation was performed using carbon dioxide and an automated insufflator (PROTOCO2L colon insufflator; E-Z-EM) under the supervision of a radiologist. A supine scout view was taken after the following suggestive signs of a fully distended colon: intolerance of the patient, initial insufflation of approximately 2 to 2.5 L or a consistent rectal pressure over 25 mmHg. Further insufflation was performed when collapsed bowel segments were identified. After completion of the supine scan, the patient was turned prone with a cushion placed under the lower chest of the patient to decrease the compression of the abdomen. A prone scout image was obtained. Further insufflation was performed if the distention was deemed suboptimal. CT scans were obtained using a 16-detector row scanner (Somatom Sensation 16; Siemens, Erlangen, Germany) without intravenous contrast enhancement and with the following parameter settings. The parameters were beam collimation, 16 × 0.75 mm; reconstruction slice thickness, 1 mm; reconstruction interval, 0.7 mm; beam pitch, 1; gantry rotation time, 0.5 seconds; table speed, 24 mm/sec; field of view: to fit; 120 kV; 30 mAs.
Image Analysis
CTC images were reviewed by consensus of two experienced radiologists (with an experience of more than 500 CTC cases and with an experience of approximately 50 CTC cases). Image review and analysis were performed with the use of a commercial CTC system (Lucion; Infinitt, Seoul, Korea).
Images were analyzed to evaluate the similarity of the scanned datasets between group I and group II patients. First, the entire colonic length was measured in each patient. The colonic length was defined as the distance from the anorectal junction to the cecal tip as measured on the software-derived centerline of the colon. The centerline distance was obtained both from the supine and the prone datasets and then the two measurements were averaged for each patient. Second, the degree of colonic distention was assessed on a segmental basis (i.e. six colonic segments of the rectum, sigmoid, descending, transverse, ascending, and cecum (18)) according to the use of a 4-point scale that Taylor et al. had previously used (19): grade 1 (worst) to grade 4 (best). The definitions of each grade have been described elsewhere (19).
Using both three-dimensional (3D) endoluminal fly-through and two-dimensional (2D) review, every luminal protrusion that was 6 mm or larger in its greatest linear dimension was marked. Size measurement of the luminal protrusions were performed on a 3D endoluminal view (20). Images from both the supine and prone positions were compared and luminal protrusions that showed an apparent positional change between the two positions were regarded to represent feces. Internal attenuation of the luminal protrusions was examined both visually and by the use of a region-of-interest (ROI) measurement. ROI measurement was performed on 2D images at a window width and level of 400 HU and 20 HU, respectively, to avoid erroneous inclusion of colonic air within the ROI due to the partial volume averaging effect (21). Luminal protrusions that showed internal air-density or had attenuation values higher than 200 HU were considered to represent feces. Any luminal protrusions other than protrusions that met the aforementioned criteria for feces were considered as polyp candidates, regardless of the morphology. Those patients who were determined to have such polyp candidates were referred for colonoscopy.
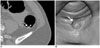
Evaluation of the degree of fecal tagging - The stool pieces were visually categorized into completely tagged (Fig. 1), incompletely tagged (Fig. 2), and untagged (Fig. 3) according to the appearances at a window width and level of 1,500 HU and -200 HU (the colon window setting), respectively. Complete tagging (Fig. 1) was defined as homogeneous high attenuation of the luminal protrusion that appeared homogeneously "white" on the colon window setting. Untagged feces (Fig. 3) represented stool pieces that appeared "gray" and might be confused with soft-tissue polyps in terms of attenuation at visual inspection. Incomplete tagging (Fig. 2) referred to the presence of both "white" and "gray" portions within the stool pieces. Attenuation values of the tagged feces were measured using an ROI. For an incompletely tagged stool piece, the ROI measurement was performed only in the tagged portion and was performed only when the tagged portion was at least a few millimeters in size to avoid erroneous measurement due to the partial volume effect. An ROI was drawn manually to encompass as much of each tagged stool as possible. ROI measurements were performed on 2D images at a window width and level of 400 HU and 20 HU, respectively (21).
Evaluation of the degree of fluid tagging - The amount of residual fluid in each colonic segment (the six colonic segments) (18) were scored in the supine position according to the ratio of the depth of the largest fluid pocket to the anteroposterior (AP) luminal diameter in each colonic segment (22). The scores were 1, no fluid; 2, < 25% AP diameter; 3, 25 to 50% AP diameter; 4, > 50% AP diameter. If fluid was present, the degree of fluid tagging was scored as follows (13, 22): 1, untagged; 2, layered tagging; and 3, homogeneously tagged. Layered tagging indicates a mix of tagging densities with a denser dependent layer and visibly less dense non-dependent layer. The attenuation value of the tagged fluid was measured by taking the average of three ROI measurements (22). In case of layered tagging, the denser dependent layer was measured.
Data and Statistical Analysis
The entire colonic length was compared between group I and group II patients by use of the Student's t-test. The degree of colonic distention was compared between group I and group II patients for each colonic segment in each position by using the Wilcoxon rank sum test.
Efficacy of fecal tagging - The efficacy of fecal tagging was analyzed on a per-lesion (per polypoid stool) basis and a per-segment basis (per colonic segment according to the six colonic segments (18)). For the per-lesion analysis, the rates of complete tagging, all degrees of tagging and untagging, defined as the numbers of completely-tagged, tagged either completely or incompletely, and untagged stool pieces 6 mm or larger, respectively, divided by the total number of stool pieces 6 mm or larger were calculated along with 95% confidence intervals (CIs). For the per-segment analysis, the rates of complete tagging, all degrees of tagging and untagging, defined as the numbers of colonic segments with all stool pieces 6 mm or larger that were completely tagged, with all stool pieces 6 mm or larger that were tagged either completely or incompletely, and with at least one stool piece 6 mm or larger that was untagged, respectively, divided by the total number of colonic segments with stool pieces 6 mm or larger, were calculated along with 95% CIs. The rates were compared between group I and group II patients. The attenuation values of tagged stool pieces, including completely tagged feces and the tagged portions of those incompletely tagged feces, were compared between group I and group II patients.
Efficacy of fluid tagging - The fluid amount scores were compared between group I and group II patients. The fluid tagging scores and the attenuation values of the tagged fluid were compared between group I and group II patients with residual fluid.
All statistical comparisons between group I and group II were performed by the use of generalized estimating equations unless specified otherwise in order to account for data clustering. P values less than 0.05 were considered as statistically significant. Statistical analysis was performed with the use SPSS 15.0 software (SPSS, Chicago, IL).
RESULTS
Study Patients and Comparison of the CT colonography Datasets between Group I and Group II
Five patients in group I and one patient in group II failed to attend scheduled CTC appointments and therefore were excluded from the study. The final study population therefore consisted of 24 patients, including ten patients in group I (five men and five women; mean age, 50 ± 8.4 years; age range, 29-58 years) and 14 patients in group II (six men and eight women; mean age, 60.4 ± 15 years; age range, 30-87 years).
The entire colonic length ranged from 126.8 mm to 202.4 mm (165.8 ± 23.2 mm) in group I and from 132.8 to 229.1 mm (172.3 ± 26.5 mm) in group II, with no demonstrable statistical significant difference (p = 0.551) between the two groups.
The degree of distention in each colonic segment in each position and comparisons between group I and group II patients are summarized in Table 1. Overall, the colon was well distended in both positions in all patients and there was no significant difference between group I and group II patients.
Efficacy of Fecal Tagging
In total, 79 luminal polypoid protrusions 6 mm or larger were found on CTC, including 42 and 37 luminal protrusions in group I and group II, respectively. Two of the luminal protrusions in two patients, both located in the transverse colon, were considered as true polyps as seen on CTC, whereas the other 77 luminal protrusions were confirmed as stool pieces based on the movability on positional change, presence of internal air and/or barium tagging. The two patients subsequently underwent a colonoscopy. The colonoscopy examination revealed no lesion in one patient, confirming that the luminal protrusion was an adherent untagged stool piece. In the other patient in group II, a 6 mm tubular adenoma was found after the colonoscopy. Another patient underwent a colonoscopy as per a request by the patient despite the CTC negative result and was shown not to have any colonic lesions. We excluded the 6 mm tubular adenoma, and 42 and 36 polypoid stool pieces 6 mm or larger in group I and group II, respectively, were finally included in the analysis.
The results of the per-lesion and per-segment analyses of fecal tagging efficacy are summarized in Table 2. For group I, 22 of 42 (52.4%; 95% CI, 37.7-66.6%), 11 of 42 (26.2%; 95% CI, 15.2-41.2%) and nine of 42 (21.4%; 95% CI, 11.5-36.2%) stool pieces were completely tagged, incompletely tagged, and untagged, respectively. For group II, 28 of 36 (77.8%; 95% CI, 61.7-88.5%), six of 36 (16.7%; 95% CI, 7.5-32.3%) and two of 36 (5.6%; 95% CI, 0.6-19.1%) stool pieces were completely tagged, incompletely tagged, and untagged, respectively. The per-lesion rates of complete tagging (p = 0.285) and all degrees of tagging (p = 0.227) were not significantly different between group I and group II.
Eighteen colonic segments in group I and 15 colonic segments in group II had stool pieces 6 mm or larger, whereas the other segments either had stool pieces 5 mm or smaller or did not have residual stool. Per segment analysis included the 18 and 15 colonic segments. The per-segment rates of complete tagging (p = 0.171) and all degrees of tagging (p = 0.219) were not significantly different between group I and group II.
The mean HU of the tagged stool pieces was 817 ± 293 HU (n = 30; range, 233-1,394 HU) for group I and 812 ± 325 HU (n = 33; range, 330-1,521 HU) for group II, with no demonstrable statistical significant difference (p = 0.938).
Efficacy of Fluid Tagging
The number of colonic segments with each fluid score was 48, 11, 1, and 0 for scores 1, 2, 3, and 4, respectively, in group I and 56, 22, 4, and 2, respectively, in group II. The vast majority of colonic segments (98.3% [59 of 60] in group I and 92.9% [78 of 84] in group II) either did not have luminal fluid or had only small amount of fluid (fluid scores 1 or 2). There was no statistically significant difference in the fluid amount between group I and group II (p = 0.156). The analysis of the degree of fluid tagging included the 12 segments and 28 segments with residual fluid in group I and group II, respectively.
For group I, 8 of 12 (66.7%; 95% CI, 38.8-86.5%), one of 12 (8.3%; 95% CI, less than 0.01-37.5%) and three of 12 (25%; 95% CI, 8.3-53.9%) colonic segments showed untagged fluid (score 1), layered tagging (score 2) and homogeneously tagged fluid (score 3), respectively. For group II, 14 of 28 (50%; 95% CI, 32.6-67.4%), one of 28 (3.6%; 95% CI, less than 0.01-19.2%) and 13 of 28 (46.4%; 95% CI, 29.5-64.2%) colonic segments showed untagged fluid (score 1), layered tagging (score 2) and homogeneously tagged fluid (score 3), respectively. The average fluid tagging score was 1.6 ± 0.9 in group I and 2.0 ± 1.0 in group II; the difference was not statistically significant (p = 0.387). The mean attenuation of tagged fluid was 647 ± 307 HU (range, 267-913 HU) and 547 ± 139 HU (range, 360-856 HU) for group I and group II, respectively, indicating no statistically significant difference (p = 0.547).
DISCUSSION
We evaluated the efficacy of barium-based fecal tagging for CTC and compared the tagging efficacy between the use of high-density (40% w/v) and low-density (4.6% w/v) barium suspensions in a population from Korea. Our study showed that the tagging efficacy of both the 40% w/v and the 4.6% w/v barium suspensions were moderate, showing 52% (22 of 42) and 78% (28 of 36) rates of complete tagging, respectively, in terms of per-lesion analysis.
One previous study performed in a Western population that used the same 40% w/v barium-based tagging suspension reported a 76% (154 of 203) rate of complete tagging in terms of per-segment analysis (13). Compared to the previous study (13), the per-segment rates of complete fecal tagging in our study, 33% (6 of 18) and 60% (9 of 15) with the 40% w/v and 4.6% w/v bariums suspensions, respectively, appears to be lower and may suggest a lower efficacy of barium-based fecal tagging in Korean patients. The different results between the previous study (13) and the present study may be due to a multitude of factors including the difference in the diet consumed the day before the CTC; i.e. a structured low-residue diet was used in the previous study (13) versus rice porridge in the present study. Unfortunately, due to some differences in the study methods, it is difficult to estimate clearly and to understand the difference in tagging efficacy between the two studies. The results of per-segment analysis should be interpreted carefully as a low rate in the per-segment analysis may not necessarily mean a low tagging efficacy. In the per-segment analysis, when multiple stool pieces are present in each colonic segment, the tagging efficacy is calculated as very low as long as at least one of the multiple stool pieces is poorly tagged, regardless of the number of well-tagged stool pieces. Therefore, the tagging efficacy can be underestimated. Moreover, interpretation of CTC is not performed on a segmental basis but the interpretation consists of the characterization of each and of every luminal protrusion into a true polyp or residual feces; thus, a per-lesion analysis would be more clinically relevant than a per-segment analysis. This was the reason why we analyzed the data both on a per-lesion and on a per-segment basis. Therefore, it is difficult to compare clearly the present results with the findings of the previous study (13). It is even more difficult to know the difference between our results and those of some other previous studies (2, 8) as those studies analyzed the tagging efficacy mostly on a per-segment basis and did not provide the exact rates of untagged stool (2, 8).
Regardless of whether or not barium-based fecal tagging is less effective in a population of Korean patients as compared to Western patients, what is clear from our study is that barium-based tagging with both the use of the 40% w/v and 4.6% w/v preparations requires further improvement. Although barium-based fecal tagging has been widely accepted for CTC, the finding that the method is not always ideal for fecal tagging has been consistently observed in previously studies (2, 6-8, 10-13) as well as in the present study. Imperfect fecal tagging with the remaining untagged stool pieces does not always pose a substantial diagnostic problem as untagged stool pieces can be clearly differentiated from true polyps by mobility, presence of internal air and morphology in many cases, as demonstrated in our study and also in previous studies (2, 8, 13). Nevertheless, there is no doubt that better quality of fecal tagging will further improve the interpretation of CTC. First, false-positive diagnoses can be reduced with a better degree of fecal tagging as demonstrated by the occurrence of one false-positive diagnosis in our study. Second, visualization of polyps covered with residual feces will be improved, resulting in better detection of such lesions. Third, straightforward differentiation of true polyps from tagged stools will be possible based on attenuation alone, which will substantially reduce the tedious and time-consuming matching of polyp candidates between the supine and prone positions in order to confirm mobility on the positional change. Fourth, it has become easier and more effective to incorporate advanced interpretive software tools such as electronic cleansing, volume rendering with attenuation-dependent discriminative color-coding of tagged stool or computer-aided detection in the interpretation of CTC as these software tools are not effective with incompletely or inhomogeneously tagged feces (23-26).
Our study showed a tendency towards better tagging with the use of the 4.6% w/v barium suspension than with the 40% w/v barium suspension; therefore, a study of a larger sample size might be able to confirm the superior efficacy of one tagging agent to the other, although this is conjecture. The findings of the present study cannot provide clear information regarding this issue, which is a limitation. However, we believe that it would be more important to understand the limitations of the use of both barium-based tagging agents in a population of Korean patients, which our study has clearly shown, and to contrive ways to improve the tagging efficacy rather than merely to determine which agent yields better fecal tagging.
As one way to improve fecal tagging efficacy, a combination of a barium suspension with a water-soluble iodinated agent such as gastrografin may be worthy of further investigation. Barium-based tagging methods are also generally ineffective for fluid tagging as demonstrated in the present study; the majority of colonic segments with residual colonic fluid (75% [9 of 12] and 53.6% [15/28] in group I and group II, respectively) showed either untagged fluid or layered tagging. Therefore, the use of gastrografin will improve fluid tagging as well. As gastrografin has a mildly cathartic effect (27), a smaller amount of fecal residue is also expected with the use of gastrografin. Given that a large amount of residual tagged fecal matter, even though well-tagged, may sometimes ironically make the interpretation of CTC more difficult (7, 16), some reduction in the amount of residual feces with the use of gastrografin could be an additional advantage. A limitation of the use of gastrografin is that it may potentially decrease patient compliance due to a bitter taste. As the ultimate goal of fecal tagging is not only to improve the diagnostic accuracy and the reading efficiency but also to improve patient compliance to participate in the examination, further studies are required to determine when to use and how to use gastrografin in conjunction with barium-based tagging agents.
Attenuation of the tagged fecal matter is another factor that determines the effectiveness of fecal tagging as weakly tagged feces may have a potential to mimic contrast-enhanced polyps or vice versa (16). Fortunately, this potential pitfall is most likely a very rare phenomenon for several reasons. Firstly, CTC for colorectal cancer screening, which is the foremost indication for the application of CTC, is typically performed without the requirement for intravenous contrast injection. Second, even with the use of intravenous contrast enhancement, as patients are scanned twice in the supine and prone positions, one scan can be obtained without intravenous contrast that allows for the opportunity to confirm the presence of contrast-enhanced lesions. Third, contrast-enhanced colorectal polyps are generally seen with a much lower attenuation than barium-tagged fecal matter (21). Our study results also showed that the attenuation of tagged stool with both the use of 40% w/v and 4.6% w/v barium suspensions was much higher than the attenuation values of contrast-enhanced polyps as previously reported in the clinical literature (21). Nevertheless, the lowest attenuation value of tagged feces was as low as 233 HU in our study (with the use of the 40% w/v barium suspension), alerting the necessity of some improvement for consistent achievement of high attenuation. Combined use of barium and an iodinated agent may be useful in this regard as well.
This study has limitations. First, the study was a preliminary study with a small sample size and without randomization of patients. Therefore, the comparison between the two tagging methods was not conclusive. Randomization was not used as it was considered most likely ineffective or meaningless for a small number of patients where a multitude of potential factors may affect bowel habit and the amount of residual feces. Second, colonoscopy was performed only in a subset of the patients. Even though endoscopic confirmation was not available in many patients, we believe that our specified radiographic criteria allowed for unequivocal identification of residual feces and our method was sound in terms of investigating the efficacy of fecal tagging. Third, we used one method of purgative bowel cleaning. The tagging efficacy may vary with the use of different bowel cleansing methods. Moreover, as one of the major advantages of fecal tagging is the reduced need for purgative bowel cleansing, investigation of the tagging efficacy in a reduced-cathartic or cathartic-free environment may be worthy of further investigation.
In conclusion, barium-based fecal tagging using both the 40% w/v and the 4.6% w/v barium suspensions showed moderate tagging efficacy. The preliminary comparison did not demonstrate a statistically significant difference in the tagging efficacy between the two tagging agents despite the tendency toward better tagging with the use of the 4.6% w/v barium suspension.




 XML Download
XML Download