

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abbreviations
ALSA
aberrant left subclavian artery
ARSA
aberrant right subclavian artery
CAA
cervical aortic arch
IAA
interrupted aortic arch
LAA
left aortic arch
LSA
left subclavian artery
MDCT
multidetector computed tomography
MinIP
minimum intensity projection
MIP
maximum intensity projection
MPR
multiplanar reformatting
RAA
right aortic arch
VR
volume rendering
Congenital anomalies of the aortic arch are uncommon and may be associated with other congenital cardiovascular diseases. A congenital anomaly of the aortic arch is usually an incidental radiological finding in asymptomatic patients, except when the anomaly constitutes a vascular ring that is formed when the abnormally patterned arch vessels completely encircle the trachea and esophagus (1). Multidetector computed tomography (MDCT) angiography has recently become a principal diagnostic method for the assessment of thoracic aortic abnormalities. The advantage of the use of MDCT angiography is that the modality is a noninvasive technique that enables evaluation of vascular anomalies and the status of tracheal or esophageal compression in the same study (2, 3). Disadvantages of the use of MDCT angiography, especially in pediatric patients, are the necessity to use iodinated contrast medium as well as an increase in patient radiation exposure. Magnetic resonance (MR) angiography is an alternative non-invasive tool without the need for contrast material or radiation exposure. However, the method is time-consuming and may require the need for prolonged sedation in pediatric patients. Although MR angiography may show vascular anomalies, the technique does not provide sufficient information regarding the esophagus and trachea.
Multidetector CT Scanning Technique
Multidetector CT angiography examinations were performed with a 16-row MDCT (LightSpeed Ultra, GE Healthcare, Milwaukee, WI). Patients were examined while in the supine position and all images were acquired during a single breath hold, extending from the base of the neck to the diaphragm. In adult patients, automatic tube current dose modulation was used. Imaging parameters were as follows: tube voltage, 100-120 kV; tube current, 140-300 mA, collimation, 16 × 1.25 mm; slice thickness, 1.25 mm; increment 0.6 mm; table feed, 27.5 mm/sec; rotation time, 0.5 sec. In pediatric patients, a body weight-based low-dose protocol (80-100 kV, 25-120 mA) was used to further reduce radiation exposure. A tube voltage of 80 kV was used for patients weighing less than 50 kg and 100 kV was used for patients weighing more than 50 kg. A tube current of 25 mAs was used for patients weighing less than 15 kg. A tube current of 30 mAs was used for patients weighing between 15 and 24 kg. A tube current of 45 mAs was used for patients weighing between 25 and 34 kg. A tube current of 75 mAs was used for patients weighing between 35 and 44 kg. A tube current of 100 mAs was used for patients weighing between 45 and 54 kg and a tube current of 120 mAs was used for patients weighing more than 54 kg. Imaging data was acquired after an intravenous injection of 1.5-2 ml/kg iodinated contrast agent (Iodixanol, 320 mgI/ml Visipaque, GE Healthcare) at a rate of 3-4 ml/sec. The scanning delay was determined with the use of a bolus tracking technique. The examination was initiated 4 seconds after the attenuation of a region of interest positioned in the ascending aorta reached 150 Hounsfield units (HU). For three-dimensional image reconstruction, the raw MDCT data was processed on a separate workstation (Advanced Workstation 4.2, GE Healthcare) with multiplanar reformatting (MPR), maximum intensity projection (MIP), minimum intensity projection (MinIP) and volume rendering (VR). MIP and VR techniques were used mainly for evaluation of cardiovascular structures, the MinIP technique was used to evaluate the tracheobronchial air column and the MPR technique was used to evaluate both cardiovascular structures and the status of tracheal or esophageal compression.
Embryology
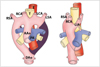
According to Edward's hypothetical double aortic arch system in which there is an aortic arch and a ductus arteriosus on each side, the right carotid and subclavian arteries arise from the right arch and the left carotid, and subclavian arteries originate from the left arch. The descending aorta is in the midline (Fig. 1A). Interruption of this arch system at different locations can explain the various aortic arch anomalies. The normal arch system results from interruption of the dorsal segment of the right arch between the right subclavian artery and descending aorta, with regression of the right ductus arteriosus (4) (Fig. 1B).
Congenital anomalies of the aortic arch include the following. The left aortic arch (LAA) with an aberrant right subclavian artery (ARSA), the right aortic arch (RAA) with an aberrant left subclavian artery (ALSA), the RAA with mirror image branching, the RAA with isolation of the left subclavian artery (LSA), the double aortic arch, the cervical aortic arch (CAA) and the interrupted aortic arch (IAA).
Left Aortic Arch with an Aberrant Right Subclavian Artery
An ARSA originating from normal left sided aortic arch is the most common aortic arch anomaly, with an incidence of 0.5-2% (5). This anomaly results from interruption of the dorsal segment of the right arch between the right carotid artery and right subclavian artery with regression of the right ductus arteriosus in the developing double aortic arch (4) (Fig. 2). In this anomaly, the right carotid artery arises as the first branch directly from the aortic arch, which is followed by the left carotid artery, left subclavian arteries and ARSA (Fig. 3). The ARSA arises from the descending aorta as a last branch and crosses the mediastinum from left to right, passing behind the esophagus and trachea (Figs. 3, 4). An aortic diverticulum, also known as Kommerell's diverticulum, may be present at the origin of this vessel and has been reported in up to 60% of cases, representing the remnant of the distal RAA (6) (Fig. 3). An ARSA is generally asymptomatic and has been diagnosed incidentally, but about 10% of adults with this anomaly have symptoms of dysphagia due to extrinsic compression of the esophagus due to its retroesophageal course (Fig. 5). Rarely, with failure regression of the right ductus, a loose vascular ring may be formed by the LAA with an ARSA, right pulmonary artery and right ductus arteriosus (1). Aneurysmal dilatation of the proximal portion of an ARSA is uncommon. Such an aneurysm may or may not be associated with Kommerell's diverticulum, and is believed to be the result of atherosclerotic disease (6) (Fig. 3). Generally, this anomaly is isolated, but may be associated with other cardiovascular anomalies, principally with coarctation of the aorta (Fig. 6), a patent ductus arteriosus, intracardiac defects, anomalous pulmonary artery circulation and carotid or vertebral artery anomalies (5, 7) (Fig. 7).
Right Aortic Arch
The RAA is a relatively common anomaly, occurring in approximately 0.05% of the population (5). RAAs have been classified into three types according to the branching pattern of the arch vessels: an RAA with an ALSA, an RAA with mirror image branching and an RAA with isolation of the LSA.
An RAA with an ALSA is the most common type (5). This anomaly results from interruption of the dorsal segment of the left arch between the left common carotid and left subclavian arteries with regression of the right ductus arteriosus in the hypothetical double aortic arch (4) (Fig. 8). In this anomaly, the first branch arising from the aortic arch is the left carotid artery, which is followed by the right carotid artery, right subclavian arteries and ALSA in order (Fig. 9). The descending aorta is usually on the right side or near the midline. An ALSA may arise from a remnant of the left dorsal aortic root (Kommerell's diverticulum) (4) (Figs. 9, 10). This anomaly rarely produces symptoms and is usually an incidental radiological finding. Rarely, a right arch with an ALSA forms a complete vascular ring, left pulmonary artery and left ductus arteriosus. Symptoms of esophageal compression may develop in older individuals with ectasia, tortuosity or an aneurysm of the ALSA (1) (Figs. 10, 11). Respiratory symptoms due to tracheal compression may be present in pediatric patients (8). This anomaly is rarely associated with other cardiovascular abnormalities (5).
An RAA with mirror image branching is uncommon, but not rare (5). This anomaly results from interruption of the dorsal segment of the left arch between the LSA and the descending aorta, with regression of the right ductus arteriosus in the hypothetical double aortic arch (Fig. 12). The left innominate artery is the first branch arising from the arch, which is followed by the right carotid artery and right subclavian arteries (Fig. 13). This anomaly is usually associated with cyanotic congenital heart disease, especially tetralogy of Fallot and truncus arteriosus (9).
An RAA with isolation of the LSA is the rarest type (5). This anomaly results from interruption of the left arch at two levels, with one level between the left common carotid and left subclavian arteries and the other level distal to the attachment of the left ductus (Fig. 14). The left carotid artery arises as the first branch of the right arch, followed by the right carotid artery and right subclavian arteries. The LSA does not have a connection with the aorta, but is connected to the pulmonary artery by a left ductus arteriosus. This rare anomaly may cause congenital subclavian steal syndrome and vertebrobasilar insufficiency. Rarely, the anomaly is associated with congenital heart disease, especially tetralogy of Fallot (10).
Double Aortic Arch
In a double aortic arch, the ascending aorta divides into two separate arches. The left or anterior arch has a course similar to that of the normal LAA, and the right or posterior arch has a course to the left behind the esophagus and joins the left arch. The descending aorta is usually on the left side. The subclavian and carotid arteries arise from their respective arches. The right and left arches may be symmetric, but usually the right arch is larger, extends more cephalad and is more posterior than the left arch (Fig. 15). This anomaly is most common cause of a complete vascular ring (5). Clinically, the onset and severity of symptoms of esophageal and tracheal obstruction are variable and depend on the tightness of the ring. Most patients present with stridor, recurrent respiratory infections or dysphagia within the first six months of life. Occasionally, the ring is so loose that is discovered incidentally in asymptomatic adults (1, 8). It is rarely associated with congenital heart disease (5).
Cervical Aortic Arch
A CAA is an uncommon congenital anomaly with a prevalence of less than 0.01%, in which the aortic arch is situated cervically above the clavicle (Fig. 16). Though this condition is often an isolated anomaly, in some cases it may be associated with other cardiac and aortic abnormalities. A CAA is associated with an aneurysm, more often left sided, in 20% of cases (11).
Interrupted Aortic Arch
An IAA is rare congenital anomaly and is characterized by the separation between the ascending and descending aorta, and is differentiated from severe coarctation and aortic atresia by the absence of any structural connection between the ascending and descending aorta. An IAA is classified based on the site of interruption relative to the brachiocephalic arteries: type A occurs distal to the LSA, type B occurs between the LSA and the left carotid artery and type C occurs between the left carotid artery and the innominate artery. Each of these three types is further subdivided as follows: subtype 1, a normal subclavian artery; subtype 2, an aberrant subclavian artery; subtype 3, an isolated subclavian artery that arises from the ipsilateral pulmonary artery by way of the ductus arteriosus. An IAA is associated with additional cardiovascular anatomic defects in up to 98% of cases (12, 13).
In conclusion, aortic arch anomalies may be associated with other developmental cardiovascular defects and may cause symptomatic esophageal or tracheal compression. MDCT is able to display the detailed anatomy of the vascular structures and their spatial relationships to adjacent organs. This ability, combined with the availability of various post-processing options such as VR, MIP and MPR that are applicable to all structures in the scanned volume, give MDCT a significant advantage in comparison to the use of other imaging modalities in the evaluation of aortic arch anomalies.















 XML Download
XML Download