

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hypereosinophilic syndrome, first described by Hardy and Anderson (1), is a spectrum of diseases characterized by severe peripheral eosinophilic leukocytosis and eosinophilic infiltration of organs such as the heart, nervous system, skin and mucous membranes, the hematopoietic system, liver, spleen, gastrointestinal tract, lung and urinary system. Clinical manifestation depends upon the organ involved and the severity of infiltration, as well as upon thromboembolic phenomena (2); symptoms and signs are, therefore, rather nonspecific. Diagnosis is usually based on persistent peripheral eosinophilia of 1500 eosinophils/mm3 for more than six months, the absence of parasitic, allergic, or other causes of eosinophilia, and evidence of organ involvement (3).
Several reports have described the sonographic, CT, and scintigraphic findings of the liver in patients with hepatic involvement (4-10), though such studies have focused only upon small, focal hepatic lesions. Over the last five years, several cases have come to light in which CT has revealed hepatic involvement over a wider area: subsegmental, segmental or lobar, for example. To our knowledge, no report has described hepatic lobar and segmental involvement in patients with hypereosinophilic syndrome. In this paper, we describe the CT findings of hypereosinophilic syndrome with hepatic lobar, segmental, or subsegmental involvement. In order to demonstrate the correlation between the CT and histopathologic findings, these latter are also reviewed.
MATERIALS AND METHODS
Medical record searches at three institutions over the last five years (1995-1999) disclosed seven patients with hypereosinophilic syndrome with hepatic lobar, segmental or subsegmental involvement, as seen on CT scans. Six were male and one was female, and their ages ranged from 17 to 50 (mean, 32) years. All patients were referred for abdominal CT scanning because of abdominal pain, fever, swelling of the upper and lower extremities, and abnormal liver function tests. In all patients, the history of any allergic disease was obtained, and stool and skin tests for parasites were performed. All results were negative. The Elisa test was not performed. In all patients, diagnosis was based on findings of hypereosinophilia in peripheral blood (eosinophil count of 3410-42, 390/mm3; 28-94%) in conjunction with biopsy, and on the response to corticosteroid therapy. Biopsy was performed under ultrasonographic guidance using a 19.5-gauge automated biopsy gun (Angiomed; Aktiengeselshaft, Karlsruhe, Germany). Three patients underwent triphasic dynamic helical CT scanning (HiSpeed Advantage; General Electric Medical Systems, MilwanRee, WI) with a bolus injection of 120 ml of nonionic contrast media (Iopamiro 300; Bracco, Milano, Italy) via the anticubital vein at a rate of 3 mL/sec by power injector, with images obtained 30, 60, and 180 sec after the start of contrast injection during the hepatic arterial, portal venous, and equilibrium phase, respectively. The scans were obtained through the liver in a craniocaudal direction with 7 mm collimation, 7-mm/sec table speed (pitch, 1.0) during a single breath-hold helical acquisition of 25-30 sec, and 7-mm reconstruction interval. The other four patients underwent conventional CT scanning (Hilight; GE, Mil-waukee, Wis., U.S.A., and Somatom DR, Siemens, Erlagen, Germany) with bolus injection of 100~120 mL ionic or nonionic contrast medium. Scans of 1.0-cm thickness were obtained during the portal and delayed phases. In one patient, follow-up helical CT scanning was performed one month after the resolution of clinical findings and laboratory abnormalities following corticosteroid treatment.
All CT images were reviewed retrospectively by three experienced abdominal radiologists with regard to the shape and distribution of hepatic abnormalities. Biopsy specimens were reviewed by one hepatobiliary pathologist at each hospital, with special reference to portal and periportal abnormalities.
RESULTS
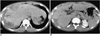
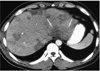
There were two cases of hepatic lobar involvement, three of segmental involvement, and two of subsegmental involvement. The clinical, pathologic and CT findings in seven patients are summarized in Table 1. In two patients, CT scans involving the right lobe of the liver (cases 1 and 2), revealed moderate hepatomegaly and low-attenuated lobar lesions involving the right hepatic lobe. In one patient (case 1), helical dynamic CT revealed heterogeneous low attenuation with a straight border limited to the right hepatic lobe (Fig. 1). There was a small, subsegmental low-attenuated lesion in the medial segment of the left lobe, but the remainder of the left lobe was normal. These findings were prominent during the portal venous phase of CT scanning, while scans taken during the hepatic arterial and equilibrium phases showed only a small, faint, subsegmental lesion. The posterior branch of the right portal vein was considerably narrowed, the diameter being 50% or less of normal. A follow-up CT scan one month after corticosteroid therapy revealed a small peripheral wedge-shaped attenuated lesion only during the portal venous phase of CT scanning. The posterior branch of the right portal vein returned to normal. In the other patient with lobar involvement (case 2), CT scans demonstrated irregular, confluent, low-attenuated lesions around the periphery of the right hepatic lobe; these findings suggest the confluence of multiple subsegmental lesions (Fig. 2).
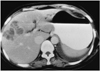
Five patients with segmental and/or subsegmental involvement (case 3-7) were found to have a few or multiple, medium-sized or small, oval or wedge-shaped low-attenuated lesions, varying in size from 1 to 4 cm, in both lobes of the liver (Fig. 3). Lesion margins were either distinct or indistinct, and some were confluent. In two patients (cases 4 and 7) who underwent three-phase helical CT scanning, segmental and subsegmental low-attenuated lesions were prominent during portal venous phase CT, but these were not prominent or were totally invisible on both arterial and delayed phase CT images. In one patient (case 4), the posterior segmental branch of the right portal vein was significantly narrowed. One patient with subsegmental involvement (case 3) exhibited clustered, round or oval low-attenuated lesions, with enhanced rims in the anterior segment of the right hepatic lobe (Fig. 4).
Histopathologic examination of liver biopsy specimens disclosed severe infiltration of periportal spaces, the sinusoids and the central veins by eosinophils and mononuclear cells (Fig. 1F). Small portal venules demonstrated severe inflammation, and the lumens were obliterated. In two patients (cases 3 and 4), an eosinophilic abscess was also noted.
DISCUSSION
Hepatic involvement is known to occur in 40-90% of patients with hypereosinophilic syndrome presenting with hepatomegaly and abnormal liver function tests (1, 2, 6). Several reports have described the varied radiological appearance of hypereosinophilia with hepatic involvement (4-10), characterizing the hepatic lesions as small and focal. CT images demonstrated that these hepatic lesions were small, oval or round, showed low attenuation, and were scattered throughout the liver, especially in areas adjacent to the portal veins. Their average diameter was 2 (range, 1-4) cm. These foci were either well- or ill-defined, and were hypoattenuated (6-9); they were reported to be most conspicuous during the portal venous phase, gradually becoming obscured during the equilibrium phase (7, 8). The number of foci was closely correlated with the percentage of eosinophils in peripheral blood, and decreased as the level of eosinophils decreased (7, 9). Ultrasound revealed that the foci were mostly hypo- (7, 10) but sometimes hyperechoic (10).
CT scans of our seven patients demonstrated hepatic lobar, segmental, and subsegmental low-attenuated lesions. In patients with lobar involvement, the margin was sharp or fuzzy and the border was straight or shaggy. Attenuation within lobar lesions was heterogeneous, and the peripheral zone was more predominantly involved. In patients with segmental or subsegmental involvement, the lesions were located predominantly along the peripheral zone of the liver, and were oval or wedge-shaped, with low attenuation. The margins were usually sharp, but some were ill-defined. Some subsegmental lesions were fused, thus creating a segmental, low-attenuated zone at the periphery of the liver.
As this is the first description of lobar or segmental involvement in patients with hypereosinophilic syndrome, the cause of lobar or segmental distribution of eosinophilic infiltration has not been discussed. We speculate that this may be related to periportal infiltration of eosinophils and portal venous thrombophlebitis, thereby resulting in decreased portal venous blood flow. It is well known that eosinophilic infiltration occurs predominantly in the periportal area (11, 12). Fauci et al. (2) hypothesized that eosinophil cationic protein might be partially responsible for thromboembolic phenomena, particularly through the formation of mural thrombi, leading to embolization. As a result, the diameter of the portal vein branches was reduced. In two of our patients, CT scanning of the right hepatic lobe indicated that the posterior branches of the right portal vein were significantly narrowed and the right hepatic lobe showed low attenuation. In one patient, follow-up CT scans obtained after corticosteroid therapy showed that normal portal vein diameter had been restored, and the right hepatic low-attenuated lesion was nearly normal.
It is well known that a transient attenuation difference seen on CT is related to portal venous obstruction or portal flow cessation caused by diseases such as hepatocellular carcinoma, liver cirrhosis or pylephlebitis (11-17). In such cases, however, the involved parenchyma shows transient hyperattenuation during arterial-phase CT, while the hyperattenuated area becomes isoattenuated during the portal phase. These findings are quite different from the CT findings observed in cases of hypereosinophilic syndrome; attenuation difference is seen mainly during the portal venous phase and the lesions are isoattenuated during the arterial and equilibrium phases. Hepatic parenchymal damage caused by eosinophil infiltration such as eosinophilic abscess, or parenchymal infarction due to vascular damage, may also play a role in decreasing hepatic attenuation during portal venous phase CT. Characteristic hypereosinophilia in peripheral blood is the important clue in establishing a differential diagnosis of lobar or segmental abnormality.
In summary, marked hypereosinophilia causes profound eosinophil infiltration of liver parenchyma and periportal spaces and resultant narrowing of the intrahepatic portal veins. Portal-phase CT scans may thus disclose the presence of lobar or segmental low-attenuated lesions.


 XML Download
XML Download