

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Alveolar soft-part sarcoma is a highly vascular malignant tumor that occurs most often in the soft tissue of lower limbs. It is a slow-growing but nevertheless malignant soft tissue tumor arising in muscle, usually in young adults. It is rare and accounts for less than one percent of soft tissue sarcoma (1, 2). The cell from which it originates is as yet unknown and the matter is open to debate.
At the time of excision of the primary tumor, vascular invasion and metastasis are frequent, and the lung is one of the most common sites of metastasis (2-4). Radiologic findings of primary tumor have been described in detail (1, 2, 5), but only a few reports have described the CT findings of pulmonary metastatic lesions. We describe the CT findings of pulmonary metastases of alveolar soft-part sarcoma in three patients.
CASE REPORTS
Clinical and radiologic findings of three patients are summarized in Table 1.
Case 1
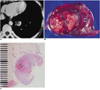
A 32-year-old woman presented with chest discomfort. Five years previously a mass involving the left foot had been widely excised. It had been diagnosed as alveolar soft-part sarcoma and the patient had undergone radiotheraphy. Chest radiography at that time had revealed a small, well-defined nodule in the left lower lung zone, but biopsy was not performed. Enhanced CT scan demonstrated a clearly enhanced nodule containing focal low attenuation, and clearly enhanced tubular structures, thought to be dilated vessels, were seen in the left lower lobe (Fig. 1A). The attenuation of the focal low-attenuated area and the tubular structures was 18±12 H and 92±8 H, respectively, while the attenuation of back muscle was 42±13 H. Wedge resection of the lung was performed, and gross examination showed that tumor size was 2.0×1.5×1.5 cm (Fig. 1B). Microscopic examination revealed dilated vessels corresponding to the enhanced tubular structures demonstrated by CT scan (Fig. 1C). The pathologic diagnosis was alveolar soft-part sarcoma.
Case 2
A 24-year-old man presented with neck stiffness and headache. Eight years previously a chest wall mass originating from the right second and third ribs had been removed. A chest radiograph obtained on admission showed a mass in the right paratracheal area and multiple nodules in both lungs. CT scan demonstrated a 5×5-cm-sized, well-circumscribed, enhanced mass compressing the Superior vena cava in the right paratracheal area. High-attenuated tubular structures within the mass, suggesting dilated vessels, were noted, and multiple enlarged hilar lymph nodes and nodules were observed in both lungs. Brain MR images showed clearly enhanced nodules in the right cerebellar hemisphere and at the right occipital pole. Resection of the cerebellar lesion and biopsy of the pulmonary nodule were performed, and pathologic examination revealed metastatic alveolar soft-part sarcoma of the brain and lung.
Case 3
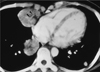
A 31-year-old woman was admitted with left lower leg mass and pain, and she also complained of coughing and blood tinged sputum. Enhanced CT scan revealed multiple enhanced masses of various sizes and intratumoral dilated vessels (Fig. 2). Incisional biopsy of the leg mass revealed alveolar soft-part sarcoma.
DISCUSSION
Alveolar soft-part sarcoma was initially defined in 1952 by Christopherson et al. (6) and was described as 'characterized by pseudoalveolar or organoid arrangement of cells in relation to numerous delicate endothelial-lined vascular sinuses and septa'. They described twelve cases of rare soft tissue tumor that showed remarkable uniformity and an alveolar pattern. Because of the uncertain origin of the cells, they were forced to use the descriptive term 'alveolar soft-part sarcoma'. The histogenesis of this neoplasm remains uncertain.
Gross pathology shows the tumors to be firm, often bulging slightly, variegated in color, and frequently hemorrhagic and necrotic; a tumor may clearly extend into blood vessels. The mass often appears to be well encapsulated but almost always there is histologically proven infiltration. Microscopically, the granular cells are arranged in nests ('alveoli') separated by connective septae that have a rich vascular networks (3).
The tumor usually involves patients between the second and fourth decade of life, and involves the lower extremities, the head and neck, the upper extremities, and the trunk, in decreasing order of incidence. There is female predominance and the median age at diagnosis is 22 years for females and 27 years for males (3).
Alveolar soft-part sarcoma is of particular clinical significance because of the high prevalence of metastases; at original diagnosis this involves 24 percent of patients. Of those without metastases at original diagnosis, 40% develop these within five years, 62% within 10 years, and 85% within 20 years (3).
Pulmonary metastases are found in 42-65% of patients (2), and the lung is the most commonly involved site by metastatic tumor The brain and skeleton are the next most commonly invowed sites. The median survival term in patients in whom metastases do not develop is 11 years, but with metastases, this period is reduced to three years (7). In cases of extrapulmonary disease that can be controlled, complete resection of pulmonary metastases of soft tissue sarcoma, including alveolar soft-part sarcoma, can prolong survival even if multiple pulmonary metastases are present (8). Because of the high prevalence of pulmonary metastasis and good clinical results of pulmonary metastasectomy, annual screening of chest CT for an indefinite period might be beneficial for patients with alveolar soft-part sarcoma.
The conventional radiographic and sonographic findings of this condition at the primary site are nonspecific (2). When unenhanced CT is used, the soft-tissue tumor is of lower attenuation than muscle (2). Enhanced CT scans show significant tumor enhancement and tortuous, dilated, and early draining veins (1, 2, 5). Similar findings were present in the pulmonary metastatic lesions present in our patients. Angiography of primary site lesions revealed hypervascularity of the tumor, with multiple enlarged tortuous vessels, prolonged tumor staining and early draining veins (1, 2, 5).
On MR imaging, the mass showed high signal intensity on T1-weighted image and very high signal intensity on T2-weighted image. Tubular areas of signal void within the tumor, as seen on both T1-weighted image and T2-weighted image, are typical of rapid blood flow in enlarged vessels (2, 5).
On CT, our cases typically showed dilated, tortuous and tubular structures within the pulmonary metastatic masses, and these represent engorged vessels. These CT findings are the same as those for primary masses of alveolar soft-part sarcoma and may reflect the characteristic pathologic findings of this rare malignant tumor. These findings are, therefore, even if not specific, helpful for differential diagnosis of pulmonary masses. They are, however, present only in cases involving masses larger than 2 cm. Nodules smaller than 2 cm show homogenous enhancement and rarely contain tortuous vascular structures. Because enhanced CT is not generally accepted in work up for pulmonary metastasis, our observation is in addition, limited.
In conclusion, we have described the CT findings of pulmonary metastatic alveolar soft-part sarcoma of the lung which on enhanced scans manifested as clearly enhanced pulmonary nodules or masses with dilated and tortuous intratumoral vessels, similar to those of the primary lesion. Alveolar soft-part sarcoma is rare, but in cases involving a clearly enhanced pulmonary mass with tortuous and dilated vessels in young adult patients, the possibility of metastatic alveolar soft-part sarcoma should be included in the differential diagnosis.

 XML Download
XML Download