

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Heitzman (1) suggested that very heavy lobes, when filled with fluid, pneumonic consolidation, or tumor, might migrate within the hemithorax with changes in the body position, adopting a dependent position. Since Heitzman's suggestion, a few cases of migration of a heavy atelectatic lobe have been reported (2, 3). Lobar migration is a shifting process within a hemithorax. The appearance of migration of an atelectatic lobe may mimic that of lung torsion (4-11), although the differential radiologic findings have not been described. Nor is it clear from the literature whether migration of an atelectatic lobe has been considered synonymous with lobar torsion (4-6).
Between 1987 and 1996 we encountered six cases of migrating lobar atelectasis of the right lung without clinical or radiologic evidence of lobar torsion. The aim of this study is to describe the radiological findings of migrating lobar atelectasis of the right lung.
MATERIALS AND METHODS
In six cases of migrating lobar atelectasis of the right lung, the radiologic findings were analyzed. The patients were two men and four women aged between 29 and 87 (mean, 59) years. Underlying diseases were bronchogenic carcinoma (n = 4), the fibrotic stage of bronchial tuberculosis (n = 1), and tracheobronchial amyloidosis (n = 1), and were confirmed by bronchoscopic biopsy (n = 5) and cytologic examination of the pleural fluid (n = 1). In two patients, open thoracotomy was performed for surgical resection of bronchogenic carcinoma. During surgery, no evidence of lobar torsion was found, and the right major and minor fissures were complete.
For these six patients, erect posteroanterior (PA) (n = 7), supine anteroposterior (AP) (n = 5), erect lateral (n = 4), supine cross-table lateral (n = 2) chest radiographs, and chest CT scans (n = 5) were available. In one patient, migrating atelectasis was seen on a follow-up erect PA chest radiograph obtained two days after the initial erect PA radiograph; migration was observed in the erect position. In one other, in order to confirm migration, fluoroscopic examination of the thorax was performed just after obtaining the chest radiographs. In all six patients, chest radiographs were obtained with the patients in different position (same position in one) within three days of initial radiography. Chest radiographs and CT scans were obtained within ten days.
Chest radiographs and CT scans were retrospectively analyzed by two chest radiologists, who reached a consensus. On radiographs, position of the atelectatic lobes, orientation of the interlobar fissures, hilar size, branching pattern of the hilar vessels, and bronchial changes were analyzed. Additional findings, if any, were also recorded. CT scans were examined for possible causes of atelectasis, and the presence or absence of hilar or mediastinal adenopathy were confirmed.
RESULTS
The right upper lobe (RUL) (n = 3) and both the RUL and right middle lobe (RML) (n = 3) were atelectatic.
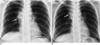
On supine AP radiographs (n = 5) and on an erect posteroanterior radiograph (n = 1), the atelectatic lobe(s) occupied the right upper lung zone with an inverted wedge shape abutting onto the right mediastinal border and the apex of the hemithorax (Figs. 1, 2). On erect PA radiographs (n = 6), the heavy lobe(s) were seen to have migrated downward, forming a peri- or infrahilar area of increased opacity and obscuring the right cardiac margin (Figs. 1, 2). Migration was observed in one patient on a follow-up erect radiograph, which had not previously been noted on a radiograph of this same type.
On supine cross-table lateral radiographs (n = 2), the atelectatic lobe(s) were seen in the anterosuperior portion of the thorax. Erect lateral radiographs (n = 4) showed inferior shift of the anterosuperiorly located atelectatic lobe(s) to the anteroinferior portion of the hemithorax.
In all patients, small right hilar size and displacement or splaying of the right hilar vessels were seen on both erect PA radiographs and/or supine AP radiographs. Fluoroscopic examination, performed in one patient, showed that the position of the atelectatic lobe had changed (Fig. 3). In two patients, right pleural effusion was seen.
Because all CT scans were obtained with patients in the supine position, dynamic changes in lobar migration could not be demonstrated on CT as they could on chest radiographs obtained in different positions. In all patients, CT scans (n = 5) demonstrated findings related to the causes of atelectasis as well as the atelectatic lobe(s) per se.
DISCUSSION
Findings of migrating RUL (right upper lobe) or combined RUL and RML (right middle lobe) atelectasis in our six patients were as follows: (1) on supine anterosuperior radiographs the atelectatic lobe(s) occupied the right upper lung zone, and a wedge shape abutting onto the right mediastinal border. This is a usual manifestation of RUL or combined RUL and RML atelectasis; (2) in an erect position, the heavy lobe(s) migrated downward, forming a peri- or infrahilar area of increased opacity obscuring the right cardiac margin and sometimes mimicking a RML lesion or an anterior mediastinal mass; (3) an erect lateral radiograph showed inferior shift of the RUL or both RUL and RML to the anteroinferior portion of the hemithorax, which had been located anterosuperiorly on a supine crosstable lateral radiograph.
Migrating lobar atelectasis per se may have no radiologic significance. When a lobe or lobes are migrating and occupying a dependent position on erect posteroanterior and lateral radiographs, however, the atelectatic lobe(s) can mimic a lesion in the RML or a hilar or mediastinal mass. In this condition, if lobar atelectasis is to be diagnosed, secondary findings such as a small displaced hilum, splaying of the pulmonary vasculature, and oligemia of the ipsilateral lung should be sought.
Lobar migration is a shifting process within the hemithorax, while lobar torsion is a rotatory or twisting process around its pedicle (bronchovascular bundle). It has been suggested, however, that lobar migration indicates torsion (4-6). As far as lobar torsion is concerned, the most commonly related conditions are previous surgery and trauma (8). In post-traumatic and postoperative torsion, clinical signs are often attributable to torsion and ensuing lobar infarction. Air leak, shock, sepsis, and deterioration of the patient may appear abruptly and progress rapidly (4). Despite migration in our cases, none of the six patients had symptoms suggestive of lobar torsion. Because spontaneous torsion itself is, in fact, seldom symptomatic (12), it may, however, be dangerous to differentiate simple migration from torsion merely on the basis of symptoms and signs.
In summary, migrating lobar atelectasis of the right lung usually involves the RUL or both the RUL and RML. On supine AP radiographs, the right upper lung zone is occupied by the atelectatic lobe(s), which form a wedge shape. On erect PA radiographs, the heavy lobe(s) are seen to migrate downward to form a peri- or infrahilar area of increased opacity obscuring the right cardiac margin. Recognition of the presence of simple migrating lobar atelectasis without torsion should preclude unnecessary emergency surgery.


 XML Download
XML Download