

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Tuberculous aneurysm of the aorta occurs only rarely. During the past 54 years, since the introduction of anti-tuberculous drug therapy, only 43 such cases have been reported in the English literature (1).
The first case of tuberculous involvement of the aorta (aortitis) was reported by Weigert in 1882 (2), and no patients are known to have survived a tuberculous aortic aneurysm until the combined technologies of modern imaging capability, anti-tuberculous drugs and vascular grafts became available. In 1952, Herndon et al (3) attempted the first surgical repair of a tuberculous aortic aneurysm, but the patient died six days after surgery. In 1955, Rob and Eastcott (4), using an Orlon cloth graft, reported the first successful reconstruction in such a case.
Tuberculous aneurysm of the aorta is noteworthy because of the high risk of sudden rupture if neither medical nor surgical treatment is attempted, and no patients have survived without medical therapy. Those who underwent surgery but did not receive anti-tuberculous drugs died, as did those who did not undergo surgery. With the early recognition of aneurysms and prompt surgical treatment by means of in-situ graft placement or extra-anatomic bypass surgery followed by anti-tuberculous medication, successful treatment is now possible, however.
This report describes two cases involving successful repair of tuberculous aneurysm of the abdominal aorta using endovascular stent grafts.
CASE REPORT 1
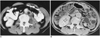
A 42-year-old woman who two months earlier had undergone surgical drainage of a psoas abscess was found to have relapsed. Cultures of the abscess had been positive for Mycobacterium tuberculosis, but chest radiographic finding were normal. The patient took anti-tuberculous drugs (isoniazid, rifampin and pyrazinamide) for two months, but abdominal pain and a palpable mass developed in the right lower quadrant. CT revealed that in the suprarenal abdominal aorta, a saccular aneurysm about 6×5×3 cm in size was surrounded by a large abscess involving the right psoas muscle and posterior pararenal space. There was associated destruction of adjacent vertebrae (Fig. 1A). Due to the high risk involved, surgery was not attempted, and urgent repair of the aneurysm by mean of an endovascular stent graft was thus required. The stent consisted of three Z-segments covered with expanded polytetrafluoroethylene (Taewoong Medical, Seoul, Korea) and with the upper one-third partially fenestrated to ensure flow along the celiac axis (Fig. 1B). A right femoral arteriotomy was performed after skin preparation, and using a 5-F pigtail catheter, an abdominal aortogram was obtained. This revealed occlusion of the superior mesenteric artery at the orifice, due to surrounding inflammation, and that supply of this vessel, from the celiac axis and inferior mesenteric artery, was retrograde. An 18-F introducer (Cook, Bloomington, IN), 50 cm in length, was cut and modified for pre-loading of the stent graft. After pre-loading, the introducer was inserted over an Amplatz heavy-duty wire (Cook, Bloomington, IN), and after exact orientation, the stent graft was deployed. To confirm successful occlusion and the patency of arterial branches, aortography was then repeated. Post-procedural angiography and CT showed that the celiac axis, renal artery, and superior mesenteric artery were patent. After stent graft placement, anti-tuberculous medications were prescribed for seven months, and CT images obtained one year after the procedure showed that the aneurysm had completely disappeared and the psoas abscess completely healed. Although the stent graft was placed in an inflamed aorta, neither CT (Fig. 1C) nor two-year clinical evaluation revealed complications such as prosthetic infection, tuberculous bacteremia, the recurrence of the psoas abscess or aortitis, or aneurysmal rupture.
CASE REPORT 2
A 41-year-old man admitted to our hospital because of diffuse abdominal pain lasting five days was referred to our department due to rupture of an abdominal aortic aneurysm during surgery. Chest radiographic finding were normal, but abdominal CT showed an irregular low-attenuation mass, about 3×4×5 cm in size and with rim enhancement, in the left para-aortic region anterior to the left psoas muscle, as well as a small aortic aneurysm (Fig. 2A). At that time, the radiological diagnosis indicated a psoas abscess. After surgical drainage of this and biopsy of the lesion, rupture of the aortic aneurysm and massive bleeding developed, and we therefore promptly deployed an endovascular stent graft 5 cm in length and 15 mm in diameter (Vanguard Straight; Boston Scientific) through the right femoral artery. Angiography revealed a 6×12 mm-sized aortic aneurysm at the level of the inferior mesenteric artery, and this was successfully occluded with the stent graft. The biopsy specimen consisted mainly of clots, and the polymerase chain reaction technique showed that this was positive for tuberculosis. After placement of the stent graft, anti-tuberculous medicine (isoniazid, rifampin, and etambutol) was administered, and follow-up CT three months later showed that the aneurysm had completely disappeared and the psoas abscess completely healed (Fig. 2B). Eighteen months after the procedure, neither complications related to stent-graft deployment nor a recurrent psoas abscess had been encountered.
DISCUSSION
Tuberculous aortitis was first described by Weigert in 1882 (2). An aortic aneurysm usually results from transmural perforation of the aortic wall caused by direct extension from a contiguous tuberculous focus, usually lymphadenitis. Rarely, direct hematogeneous invasion of the vasa vasorum may occur, producing an aneurysm, of which there are two types: a true aneurysm involves permanent dilatation of all layers of weakened but intact wall, while a false aneurysm consists of the tissue of the infected contiguous structure; there is focal perforation, and all layers of the wall are disrupted. Most tuberculous aneurysms are false; they are usually saccular and rarely dissecting. Symptoms are related to the size, position, and rapid growth of the aneurysm as well as to the activity of the primary disease.
The use of covered stents in humans with abdominal aortic aneurysms has been previously described (5). With the increasing use of endovascular stents and the continued development of newer stent designs, interest in the non-surgical management of aortic aneurysms in patients at high surgical risk is growing.
In 1955, Rob and Eastcott (4), using an Orlon cloth graft, reported the first successful reconstruction of a tuberculous aortic aneurysm, and since then, in-situ graft placement or extra-anatomic bypass surgery followed by effective anti-tuberculous medication has become standard therapy for tuberculous aortic aneurysm (6). There may, however, be surgical mortality, especially in patients with high risk factors such as old age or severe cardiac, renal, or pulmonary diseases. Percutaneous endovascular stent graft treatment offers shorter hospitalization and a shorter convalescent period, and avoids the morbidity and mortality associated with surgery. In patients with non-tuberculous mycotic aneurysms, despite placement of the stent graft at the site of primary infection, complications involving persistent bacteremia, reinfection, delayed rupture, paraplegia, distal emboli, or surgical conversion have not been reported (5).
To our knowledge, our reports are the first to describe the non-surgical treatment of tuberculous aortic aneurysm by mean of endovascular stent grafts. In one case, a surrounding psoas abscess and suspected aortic necrosis prevented surgical intervention (7).
In conclusion, the use of a stent graft combined with anti-tuberculous medication may be a relatively easy and rapid method of repairing tuberculous aneurysm of the aorta.

 XML Download
XML Download