

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Cavernous hemangiomas are the most common benign tumor of the liver, and are not infrequently encountered incidentally during US screening. Because the vast majority of hepatic hemangiomas are asymptomatic and require no treatment, they must be differentiated from hepatic malignancies. Most have a distinctive US appearance (1-4) but some, known as atypical hemangiomas, show various US patterns (5-8). For the differentiation of the atypical variety, dynamic contrast-enhanced studies have been widely employed. Using microbubble contrast agents, it has been shown that pulse-inversion harmonic US can effectively depict the typical enhancement patterns of hepatic hemangiomas (9), enabling specific diagnosis. In this essay, we review the spectrum of US appearances of these hemangiomas as seen on conventional gray-scale, power Doppler, and pulse-inversion harmonic US with contrast agents.
Conventional Gray-Scale US
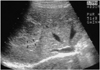
The most common and generally accepted 'typical' US features of hepatic hemangiomas are their small size, uniform hyperechogenicity, well-defined margin, and posterior echo enhancement (1-3) (Fig. 1). In addition, follow-up scanning only rarely shows a change in size, appearance, or detectability (4). Their distinctive appearances at US are considered to be due to histological characteristics. They are usually composed of large blood-filled cavernous spaces, lined by a single layer of flat endothelial cells and separated by fibrous septa; multiple interfaces between the walls of the sinuses and the blood within them account for the typical hyperechogenicity seen at US (4). The enhanced through-transmission observed in many cases reflects the low acoustic impedance of blood-filled spaces and tends to occur in hemangiomas larger than 25 mm (2).
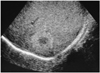
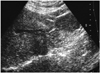
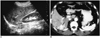
Because hemangiomas may undergo various changes including internal hemorrhage with necrosis, thrombosis, myxomatous change, fibrosis, and- rarely- calcification as they become larger (1, 4), 'atypical' US features are frequently seen in larger ones. Unlike a typical hemangioma, one that is atypical has an internal echo pattern at least partially hypoechoic; a hyperechoic mass with a hypoechoic central portion or decreased echogenicity can be seen throughout the entire lesion (Figs. 2, 3, 4, 5, 6, 7). The most suggestive US feature of this type of hemangioma is an echogenic border, seen as a thick echogenic rind or thin rim around a tumor (4) (Figs. 2 and 6). Although the prevalence of atypical hemangioma has not been precisely determined, it seems that approximately 20-40% of hemangiomas are of this kind (4, 5).
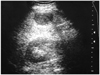
The echogenicity of hepatic parenchyma influences the US appearance of a hemangioma. Because of the increased echogenicity of attenuating fatty liver parenchyma, diffuse fatty infiltration may lead to an atypical echo-poor appearance (6) (Fig. 8). If a 'typical' hemangioma is present in a liver in which fatty infiltration has occurred, its US appearance will be altered. The lesion will initially appear less hyperechoic than isoechoic, and finally hypoechoic relative to infiltrated liver. Fatty infiltration of the liver may also cause obscuration of the echogenic border around the tumor (5).
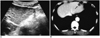
It has recently been shown that the speed of contrast enhancement occurring during incremental dynamic CT or multiphase dynamic MR imaging provides a basis for predicting the echo pattern at US, and vice versa. On dynamic CT or MR images, sonographically hypoechoic hemangiomas tend to show rapid enhancement, but if hyperechoic, they tend to enhance slowly (7, 8) (Figs. 9 and 10).
Power Doppler US
As techniques for evaluating the vascularity of various organs and diseases, color and power Doppler US have recently shown promise. Since power Doppler US is superior to color Doppler US in detecting slow flow, it has been used in atempts to diagnose hepatic hemangiomas specifically on the basis of their typical hemodynamic features. Though it was initially believed that power Doppler is able to depict slow flow within hemangiomas (10), it has been suggested that homogeneous noise from highly reflective interfaces can be misinterpreted as true flow (11). To avoid these false signals, power Doppler parameters must therefore be optimized. A recent study in which a Doppler phantom/flow control system and a 2-4 MHz transducer were used found that for determining the vascularity of hyperechoic tissue, a pulse repetition frequency of 1,000 Hz and a medium wall filter were adequate. Using these optimized parameters, the majority of hepatic hemangiomas produced either no power Doppler signal or one that was minimal (12) (Fig. 11A).
Power Doppler US with a Contrast Agent
The majority of hepatic hemangiomas show a typical enhancement pattern: peripheral nodular or globular enhancement during the bolus dynamic phase and centripetal fill-in and persistent enhancement during the delayed phase, and for this reason, dynamic contrast-enhanced CT or MR imaging has been widely used for diagnosis. Since microbubble contrast agents for US have become available, the efficacy of these for the characterization of focal hepatic lesions has been the subject of numerous investigations (9, 13-15). In hepatocellular carcinoma, the use of contrast agents greatly increases intratumoral Doppler signals (13, 14), but in hemangiomas, the use of power Doppler US with microbubble agents reveals either no internal vascularity or sparse peripheral flow (13, 15) (Fig. 11). Due to its lack of sensitivity in detecting slow flow in hemangiomas, power Doppler US can not therefore, be used for the specific diagnosis of hepatic hemangioma, even with the use of microbubble agents (15).
Pulse-Inversion Harmonic US with a Contrast Agent
Pulse-inversion harmonic US is a newly introduced technique for displaying the amplitude of second harmonic signals resulting from non-linear echoes. In contrast to power Doppler US, pulse-inversion harmonic US with interval delay scanning can provide strong gray-scale enhancement by microbubble contrast agents and detect signals from microbubbles in very slow flow without Doppler-related artifacts. It has recently been shown that this technique can depict the typical enhancement patterns of three different types of liver lesions: hemangiomas, metastases, and hepatocellular carcinomas. While most hemangiomas (95%) show peripheral globular or rim-like enhancement with progressive centripetal fill-in, malignant tumors do not show this pattern (9) (Fig. 12). Pulse-inversion harmonic US with interval delay scanning using a contrast agent is therefore believed to be potentially useful for the specific diagnosis of hepatic hemangiomas by demonstrating their characteristic enhancement features.
CONCLUSION
In the diagnosis of hepatic hemangiomas, the most important aspect is non-invasive differentiation from other tumors. Since US plays a key role in the initial evaluation of these hemangiomas, knowledge of the spectrum of those that are atypical is important and can help avoid most diagnostic errors. At the same time, however, in most cases of hemangioma with atypical sonographic features a specific diagnosis can be established by means of dynamic contrast-enhanced studies such as CT or MR imaging. Because pulse-inversion harmonic US with interval delay scanning using a contrast agent is also believed to be potentially useful for the specific diagnosis of hepatic hemangiomas by demonstrating their characteristic enhancement features, simple and immediate characterization of a focal hepatic lesion newly detected by initial US examination is possible.






 XML Download
XML Download