

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Solitary necrotic nodule of the liver is an uncommon non-malignant lesion first described by Shepherd and Lee in 1983 (1) and comprising a central necrotic core enclosed by a hyalinized fibrotic capsule containing elastic fibers. Several pathogenic mechanisms including the possibility that the condition has a traumatic etiology, or is a consequence of previous parasite infection or sclerosing hemangiomas have been suggested (2, 3). Such lesions are frequently found in a subcapsular location, protruding slightly from the surface of the liver and with a sharply defined border, and may be mistaken for metastasis. In the published literature, the histopathologic features and pathogenesis of the solitary necrotic nodule have been discussed (1-4), but as far as we are aware no reports have emphasized the radiologic findings.
The purpose of this report is to describe the radiologic findings of two cases of solitary necrotic nodule of the liver mimicking hepatic metastasis.
CASE REPORTS
Case 1
A 54-year-old woman was admitted for evaluation of a polypoid gallbladder mass measuring 2.0 cm in diameter and a hepatic low-echoic nodule discovered by US examination during a check-up. Serum CEA, CA 19-9, and alpha-fetoprotein levels were normal. Arterial- and portal-phase spiral CT revealed focal wall thickening with enhancement in the fundus of the gallbladder and a poorly-defined, ovoid hypoattenuating nodule with peripheral rim enhancement measuring 1.0 cm in diameter in the right lobe of the liver. These findings suggested gallbladder cancer with hepatic metastasis. For evaluation of metastasis prior to surgery, the patients underwent CT during arterioportography (CTAP) and during hepatic arteriography (CTHA). An ovoid portal perfusion defect area was demonstrated by CTAP (Fig. 1A), and a highly enhancing nodular lesion in the same area of the right lobe of the liver by CTHA (Fig. 1B). One week later, surgery was performed. Intraoperative US showed that the lesion was a target-appearing hypoechoic nodule measuring 1.0 cm in diameter. In addition, two other nodules each with a diameter of 0.5 cm, were present in the same segment of the liver (Fig. 1C). The patient underwent right hepatic lobectomy and cholecystectomy. Histopathologic examination indicated that the gallbladder lesion was an adenocarcinoma with tubular, well-differentiated characteristics and had invaded the perimuscular connective tissue. The hepatic nodules were diagnosed as a solitary necrotic nodule composed of a central necrotic core and a peripheral fibrotic capsule with inflammatory cells (Fig. 1D).
Case 2
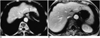
A 72-year-old man was admitted for vomiting and poor oral intake, which had lasted for six days. Six years earlier, due to gastric cancer, he had undergone a subtotoal gastrectomy with Billroth II anastomosis. On plain radiographs of the abdomen, diffuse dilatation of the proximal jejunal loop, with collapsed distal loop, suggesting jejunal obstruction, was seen. Abdominal CT showed a dilated proximal jejunal loop, with an abrupt transitional zone and bowel wall thickening. In addition, an elliptical, hypoattenuating nodule measuring 1.0 × 0.3 cm in diameter was observed in the lateral segment of the left lobe of the liver (Fig. 2A). T2-weighted MR imaging (T2WI) indicated that a nodule at the same site was hyperintense, and T1WI that it was isointense, while Gadolinium-enhanced study suggested the presence of a subtle, peripheral enhancing nodule (Fig. 2B). We regarded these imaging findings as indicative of small bowel obstruction due to tumor recurrence, with hepatic metastasis, and later, as adhesive ileus and nontumorous lesion of liver. The patient underwent surgery and this indicated that the proximal jejunum, about 10 cm from the Treitz ligament, had adhered to the operative wound. In addition, a hard, whitish mass 1.0 cm in diameter, was found in the liver. The patient underwent adhesiolysis of the jejunal loop and wedge resection of the liver lesion. On histopathologic examination, the liver mass was diagnosed as solitary necrotic nodule.
DISCUSSION
Solitary necrotic nodule of the liver is an uncommon lesion on the basis of US or CT examination, which has often been diagnosed as necrotic metastasis (1-4). A solitary necrotic nodule, despite its name, may be multiple (5), and in a large number of cases, may represent the end-stage of a variety of benign lesions such as larval infestation, sclerosed hemangioma or trauma (2-4). Histologically, the lesion consists of an outer fibrotic capsule with inflammatory cells and a central core of amorphous necrotic material, and occurs in a subcapsular location or in deep liver parenchyma (3).
Recent advances in hepatic surgery have lead to in an increase in the number of candidates for partial hepatic resection due to metastatic diseases. The major roles of imaging are to provide a clear and detailed map of hepatic metastasis and to make a careful preoperative selection of patients, thus avoiding unnecessary surgical exploration. Noninvasive imaging techniques, including US, CT, and MR imaging, have recently improved the detection of hepatic metastasis. Among these modalities, CTAP is known to be most sensitive for the detection of focal hepatic lesions, though its high false-positive rate is considered a disadvantage (6). Intraoperative US has also been used to detect small metastases not identified by direct palpation or by other preoperative imaging techniques (7). However, the radiologic features of these modalities are not sufficiently specific for the accurate characterization of liver tumors.
On contrast-enhanced CT, hepatic metastases usually present as focal hypoattenuating areas relative to normal hepatic parenchyma, on CTAP as oval or round areas of perfusion defect, and on US as target-appearing hypoechoic nodules. In patients with primary malignancy, the focal hepatic lesion mimicking hepatic metastasis include liver abscess, inflammatory pseudotumor (8), and focal eosinophilic infiltration (9, 10). In our cases, the radiological findings of solitary necrotic nodule of the liver on each modality were similar to those of hepatic metastasis. Because solitary necrotic nodule of the liver exhibits central hypoattenuation of the necrotic area and peripheral hyperattenuation due to the presence of fibrosis, differentiation by means of CT between this nodule and hepatic metastasis is very difficult or impossible. The intraoperative US findings of the lesion also simulated hepatic metastasis, even though lesion multiplicity had been elucidated. A hepatic metastatic tumor usually appears as a well-defined, round mass, but in our cases, a solitary necrotic nodule of the liver seen as a relatively ovoid or elliptical mass. Such a finding is not specific for this condition, however, and for correct diagnosis, needle biopsy may therefore be necessary.
In conclusion, solitary necrotic nodule of the liver may be revealed by on radiologic imaging as single or multiple lesions of the liver, a finding which may be misinterpreted as metastatic hepatic tumor.

 XML Download
XML Download