

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Since the first introduction of percutaneous transcatheter renal artery embolization in 1964 (1), the devices used in interventional radiology have made rapid progress and super-selective catheterization is now possible. For successful renal artery embolization, both the selection of appropriate embolic material and adequate operator experience are prerequisites. The embolic materials used in renal vascular lesions include absolute ethanol, ethibloc, gelfoam, polyvinyl alcohol, coils and detachable balloons (2). Some of these are, however, hard to prepare and/or difficult to use in super-selective embolization and may result in incomplete occlusion and/or recanalization. Embol (Department of Biomedical Engineering, Seoul Health College, Kyonggido, Korea) is a new embolic material obtained by partial hydrolysis of polyvinyl acetate mixed in absolute ethanol and Iopromide 370, and manufactured by Schering Korea, Kyonggido, Korea. Portal vein embolization using Embol has been reported (3, 4). We describe the results of six cases of endovascular treatment for renal vascular lesions using this new liquid embolic material.
MATERIALS AND METHODS
Embol is prepared in a polymerized state and is insoluble in water. When it comes into contact with blood, ethanol is washed out, resulting in precipitation of the embolic material and obstruction of the vessel. Partial hydrolysis of polyvinyl acetate increases the hydrophilic property of the polymer, making it soluble in a larger amount of angiographic contrast medium and increasing the radiopacity of the solution. We retrospectively reviewed the angiographic findings and medical records of six patients with renal vascular lesion who had undergone endovascular treatment with Embol. Four were male and two were female, and their ages ranged from 11 to 70 (mean, 53) years. Clinical or radiological diagnoses referred for endovascular treatment were renal cell carcinoma in three patients, angiomyolipoma in two and pseudoaneurysm of the renal artery with retroperitoneal hematoma which developed after renal biopsy in one. Analysis of adverse reactions resulting from renal artery embolization with Embol continued until the date of discharge.
Procedures
For angiographic evaluation, percutaneous transfemoral catheterization using Seldinger s method was employed. Diagnostic aortography and selective renal angiography involved the use of a 5-Fr Cobra catheter (Cook, Bloomington, Ind.) and the digital subtraction technique. When the proximal main renal artery was embolized, an iliac sheath and balloon occlusion catheter were used to exclude possible regurgitation. In these cases, Embol was injected through the catheter. Where embolization was performed superselectively at the segmental artery, various coaxial catheters were used, without a balloon occlusion catheter. In one patient with pseudoaneurysm of the renal artery, stenosis of the proximal renal artery was combined and Embol was injected percutaneously under sonographic guidance.
After embolization, the catheter was flushed with 35% ethanol, and 15 to 20 minutes were allowed for Embol to precipitate. Post-embolization angiography was then performed. Patient characteristics and the devices used are summarized in Table 1.
RESULTS
Angiographic results
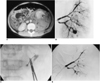
In all cases the procedures were performed in a single step, and embolization was performed immediately after selective renal angiography. During embolization, Embol was clearly visualized fluoroscopically. Total occlusion of renal vascular lesions was achieved immediately in all six patients, although in one, a stainless steel coil (Cook, Bloomington, Ind.) was also used (Fig. 1). No renal parenchymal infarction was seen in non-embolized kidney segments.
Clinical results
One of the three patients with renal cell carcinoma (patient 1) underwent radical nephrectomy three days after embolization, and a pathologic specimen revealed 40% tumor necrosis. Nine months after surgery, this patient was doing well, without tumor recurrence (Fig. 1). One patient with renal cell carcinoma (patient 2) refused further treatment and was discharged, but was still alive six months after embolization. The one remaining patient with advanced renal cell carcinoma (T4) at the time of diagnosis (patient 3) expired three months after embolization due to deterioration in his general condition. In both patients with angiomyolipoma, right lower quadrant abdominal pain was successfully controlled. Follow-up sonography revealed that the angiomyolipomas had decreased in size from 7.5 to 6 cm in one patient (Fig. 2) and from 3.1 to 2.3 cm in the other. In the patient with pseudoaneurysm of the renal artery and retroperitoneal hematoma, bleeding stopped immediately after embolization. Serial follow-up sonograms indicated that retroperitoneal hematoma resolved gradually and no recurrent pseudoaneurysm was found (Fig. 3).
Elevated blood urea nitrogen and creatinine levels were seen after embolization in one patient with renal cell carcinoma (patient 2). This patient refused further treatment, however, and was discharged. The patient with pseudoaneurysm of the renal artery (patient 6) experienced renal failure before embolization and had elevated levels of blood urea nitrogen and creatinine, though no changes in these were observed before or after embolization. Transient elevated blood pressure was also seen in this patient, but the pressure decreased to normal within three days, without medication. Post-embolization syndrome of fever, nausea, vomiting, flank pain and/or leukocytosis occurred in four of six patients (Table 2). At the end of the procedure, transtumoral shunting of Embol to the renal vein occurred in one patient (patient 3) with advanced renal cell carcinoma (T4). Embolization was stopped immediately and balloon occlusion of the proximal renal artery was performed. Follow-up chest radiographs revealed no subjective chest symptoms or consolidation.
DISCUSSION
Since Edling first introduced renal artery embolization in 1964 (1), the applications of renal intervention have rapidly extended. Current indications for transcatheter renal artery embolization include hemorrhage resulting from trauma or renal tumor, renal arteriovenous malformation, end-stage renal disease, severe hypertension refractory to other methods of treatment, and recurrent infected hydronephrosis in a hemophilic patient (5).
There is little support for routine embolization of renal cell carcinoma during the immediate preoperative period (2, 6, 7). It is, rather, performed for conservative purposes in cases of solitary kidney, bilateral tumors, inoperable cases and tumor bleeding. Indications for the embolization of angiomyolipomas are a tumor larger than 4 cm or any tumor with continuous symptoms (8, 9). Renal arteriovenous fistulas and pseudoaneurysms are common complications occuring at a rate of 0.2 to 2% after renal biopsy (10), and for these lesions, transscatheter embolization is an effective method of treatment (10, 11). In all our cases, Embol was also effective, providing immediate total occlusion of the renal vascular lesion.
The development of co-axial catheters has facilitated super-selective embolization, with less trauma to unwanted segments of renal parenchyma (12). In addition, newer embolic materials are still being developed and tested (3, 4, 13-16). Embolic materials used in renal vascular lesions include absolute ethanol, ethibloc, gelfoam, polyvinyl alcohol, isobutyl-2-cyanoacrylate, coils, detachable balloons and autologous tissues. Some of these materials, however, involve tedious preparation, unequal suspension, high friction, difficulty in injecting through a microcatheter, incomplete occlusion and recanalization. Since the beginning of the 1980s, absolute ethanol or a mixture of absolute ethanol and oidized oil has been the recommended agent for embolization of renal vascular lesions (2, 7, 9). Absolute ethanol is fluoroscopically radiolucent, and unintentional embolization of non-target organs can occur. Embol, on the other hand, is radiopaque and unintentional embolization of the non-target organs can be prevented. Intratumoral arteriovenous shunt occurred in our series, at the end of the procedure, in a patient with renal cell carcinoma. Embolization was stopped immediately and balloon occlusion of the proximal renal artery was performed. After embolization, no pulmonary complication was noted either clinically or on chest radiographs.
A demerits noted during embolization with Embol is its high viscosity, and high pressure is thus required for injection, especially when coaxial microcatheters are used. In addition, there is a waiting time of 15 to 20 minutes for Embol to precipitate, and persistent pain occurs during embolization, though this is less than when absolute alcohol is used. A further disadvantage of Embol is the fact that it is difficult to ascertain the exact point before termination of the procedure at which precipitation actually occurs.
The reported complications of renal artery embolization include renal failure, post-infarction syndrome, gas formation in necrotic tissue and unintentional embolization of non-target organs (5, 17). Post-infarction syndrome was seen in four of six patients in our study, but the symptoms subsided with conservative care.
In conclusion, Embol is an effective embolic material which offers immediate and total occlusion of renal vascular lesions. It also appears to be safe to use, since it is adequately radiopaque during embolization, and no significant changes in blood pressure, body temperature, or blood urea nitrogen and creatinine levels occur after embolization. To avoid reflux of Embol to non-target organs, balloon occlusion catheters should be used during embolization of the proximal main renal artery. When embolization is performed after super-selection of the segmental branch, balloon occlusion will not be necessary.



 XML Download
XML Download