

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ischemia is restriction of blood supply causing shortage of oxygen and vital nutrients and restoration of blood flow to an ischemic organ is essential to prevent irreversible cellular injury. However, prolonged ischemia and thereafter reperfusion results in ischemia-reperfusion injury [1]. Such injury occurs in a wide variety of clinical problems including ischemic heart diseases, stroke etc. whereby blood supply to an organ or tissue is reduced. Some strategies have been used to minimize this injury; one of such approach is remote ischemic preconditioning. Remote ischemic preconditioning (RIPC) is a unique phenomenon, whereby 3~4 consecutive ischemia-reperfusion episodes are given to a remote tissue (non-cardiac) to provide protection to the target organ (heart) against sustained ischemia-reperfusion injury [2]. An earlier study demonstrated that 4 cycles of 5 min occlusion and reperfusion of the left circumflex artery lessened the infarct size in the left anterior descending coronary artery [3]. In the later years, short episodes of occlusion-reperfusion of the arteries including cerebral, mesenteric, renal arteries [4], abdominal aorta and intestinal [5] induced myocardial protection against sustained ischemia-reperfusion injury in various animals like mice, rabbits, pigs, sheep, swine, dogs [67], and human beings [8].
Recently, RIPC has also been evolved in clinical settings and has been reported to alleviate ischemia-reperfusion injury in patients undergoing coronary angioplasty, coronary artery bypass surgery, percutaneous coronary intervention, elective abdominal aortic aneurysm repair [29]. Furthermore, RIPC significantly improved the coronary microcirculation in myocardial infarction and heart failure patients [10]. The clinical applications of RIPC have been expanding as brief episodes of inflation/deflation of blood pressure cuff at arm, leg or both can be delivered non-invasively [6]. Furthermore, studies have shown that preconditioning ischemia to different organs including kidneys, liver, intestine or limbs produce cardioprotection with comparable efficacy [57].
Although, the mechanisms involved in mediating RIPCinduced cardioprotective effects have not been fully elucidated, yet there have been two theories of RIPC-induced cardioprotective effects viz. neurogenic theory and humoral theory. The neurogenic theory states that RIPC leads to the release of endogenous mediators that activate the afferent nerves to relay signals to the efferent nerves, which convey the cardioprotective signals to the heart [11]. On the other hand, the humoral theory postulates that RIPC encourages the release of endogenous substances into the bloodstream that reach the heart to exert cardioprotective effects [1112]. There have been abundant reports emphasizing the involvement of neurogenic signaling in mediating RIPC-induced cardioprotection (Table 1) [81314151617]. Therefore, the present review was designed to explore the involvement of neurogenic pathways in remote hind limb preconditioning induced cardioprotection.
Go to : 
EVIDENCES REGARDING THE INVOLVEMENT OF NEUROGENIC PATHWAY IN RIPC
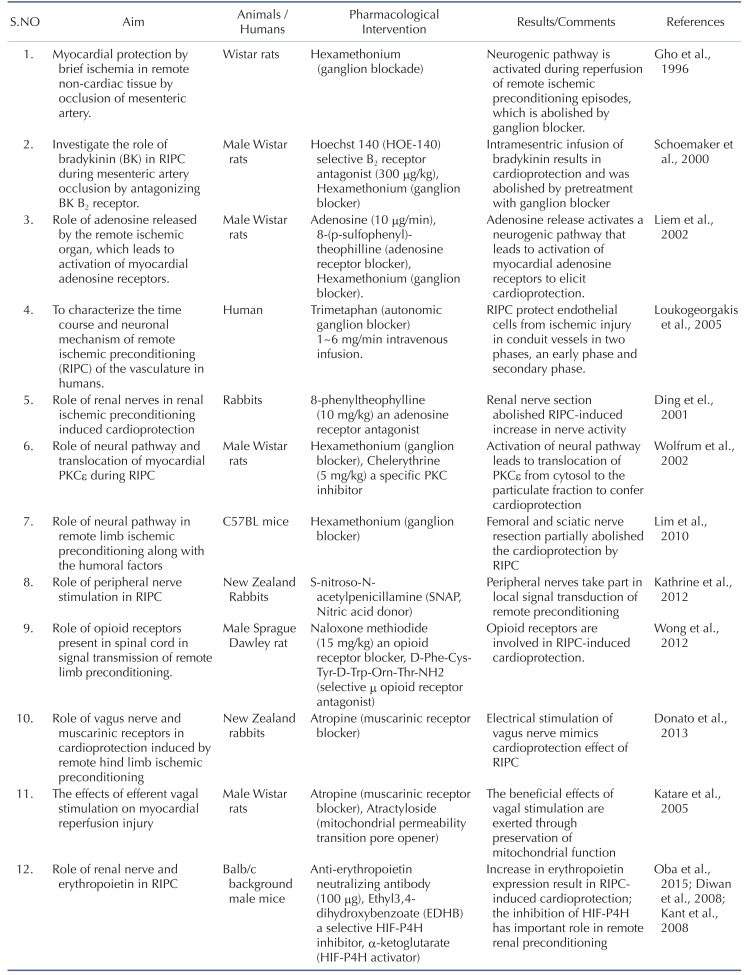
Gho et al. (1996) studied myocardial protection by the application of brief ischemia in remote noncardiac tissue in male Wistar rats in the form of mesenteric artery occlusion. The mechanism of protection in latter differs from that of short ischemic episodes due to coronary artery occlusion (ischemic preconditioning) because the ganglion blocker (with hexamethonium) abolished protection in mesenteric artery occlusion, but not in coronary artery occlusion. The authors demonstrated that the neurogenic pathway is activated during reperfusion phase of remote ischemic preconditioning episodes and sustained mesenteric artery occlusion failed to produce the cardioprotection [13]. Schoemaker et al. (2000) investigated the role of bradykinin in remote preconditioning and hypothesized that during RIPC, the sensory nerves may be stimulated in the ischemic region to activate the neurogenic pathway to produce cardioprotection. Administration of selective B2-receptor antagonist, HOE-140 (300 µg/kg) completely abolished the cardioprotective effects of remote as well as classical ischemic preconditioning. Furthermore intramesentric infusion of bradykinin resulted in significant cardioprotection, which was abolished by pretreatment with ganglionic blocker (hexamethonium) [14].
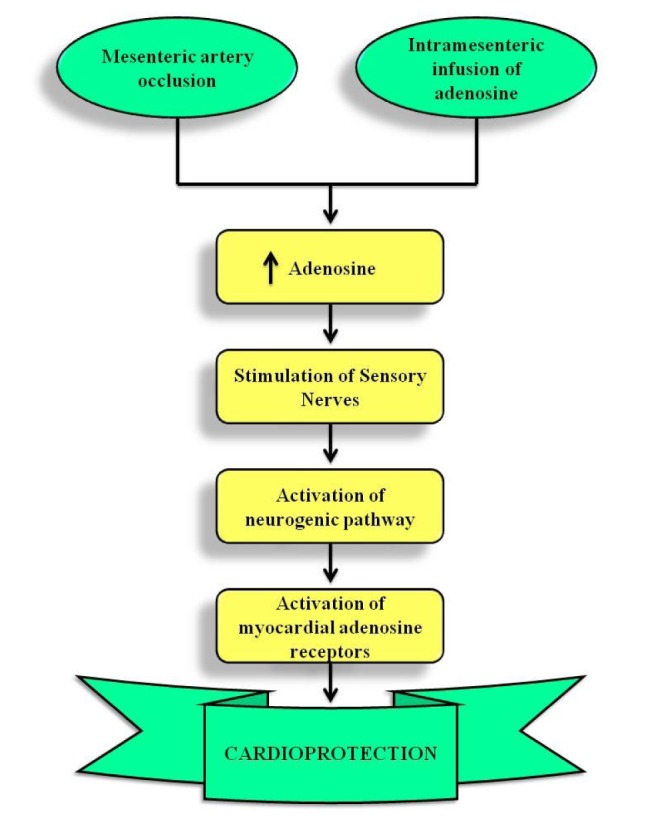
Liem et al. investigated the sites of action of adenosine in interorgan preconditioning of the heart. They showed that adenosine is locally released during intestinal ischemia reperfusion episodes of remote preconditioning, which stimulates the afferent nerves in the mesenteric bed during early reperfusion. The role of adenosine was also confirmed by infusion of adenosine (10 µg/min) in intramesentric artery, which mimicked the cardioprotective effects of remote ischemic preconditioning. However, these effects were attenuated by adenosine receptor blocker 8-(p-sulfophenyl)-theophilline or hexamethonium, administered before or after 5 min of mesenteric artery reperfusion. Accordingly, it was proposed that interorgan preconditioning induced adenosine release initiates a neurogenic pathway that leads to activation of myocardial adenosine receptors to elicit cardioprotection (Fig. 1)[16].
Loukogeorgakis et al. interrogated the time course and neuronal mechanism of remote ischemic preconditioning of vasculature in humans. The study demonstrated that RIPC protects endothelial cells from ischemic injury in conduit vessels in two phases, an early phase which is activated immediately and continued up to 4 hours, and secondary phase which starts after 24 hours of RIPC stimulus and sustained for at least 48 hours. Endothelial function of brachial artery was assessed by flow mediated dilation (FMD) before and after RIPC. Both phases of protection was dependent on the intact autonomic function, confirmed by the administering autonomic ganglion blocker trimetaphan (1~6 mg/min intravenous infusion), which attenuated both early and delayed phases of RIPC [8]. Ding et al. investigated the role of renal nerves in renal ischemic preconditioning induced cardioprotection in rabbits. The authors demonstrated an increase in discharge from afferent renal nerves in response to transient renal ischemia and afferent activity was measured by amplifier (AVB-II) and was expressed by impulses/second. However, pretreatment with adenosine receptor antagonist 8-phenyltheophylline, (10 mg/kg) and renal nerve section abolished RIPC-induced increase in renal nerve afferent activity [15]. Wolfrum et al. interrogated the role of myocardial PKCε-isoform in RIPC-induced cardioprotection in male Wistar rats. Administration of ganglion blocker hexamethonium, or specific PKC inhibitor chelerythrine (5 mg/kg) before RIPC abolished the cardioprotection and blocked the translocation of PKCε from cytosol to the particulate fraction. It suggests that the activation of neural pathway during RIPC induces the translocation of PKCε from cytosol to the particulate fraction to confer cardioprotection [17].
Lim et al. also studied the role of neural pathway in remote limb ischemic preconditioning along with the humoral factors. Both the femoral and sciatic nerve resection partially abolished the cardioprotection by RIPC as compared to sham procedure in C57BL mice [11]. Redington et al. studied the role of peripheral nerve stimulation and topical capsaicin application in remote cardioprotection in New Zealand rabbits. It was suggested that direct electrical or peripheral neural stimulation evokes the release of cardioprotective substances into the blood, which reduce the infarct size and improve the post cardiac performance. Previously, the same group of authors also showed that RIPC by limb ischemia or intra-arterial adenosine releases a dialyzable cardioprotective circulating factors [18]. The release of these factors required an intact neural connection to the limb and the release of these factors was abrogated by prior femoral nerve transaction. The direct stimulation of femoral nerve itself induced cardioprotection and pretreatment with S-nitroso-N-acetylpenicillamine (SNAP) abrogated the cardioprotective effect of dialysate. These results confirm the role of peripheral nerves in the local signal transduction of remote preconditioning [19].
Wong et al. interrogated the role of opioid receptors present in the spinal cord in the signal transmission of remote hind limb preconditioning and remote preconditioning of trauma (RPCT). Intraspinal administration of naloxone methiodide (15 mg/kg) in male Sprague-Dawley rat blocked the cardioprotective effects of both types of remote preconditioning by antagonizing the opioid receptors present in the spinal cord. Since the drug does not cross the blood barrier, therefore the reported effects of naloxone can be ascribed to blockade of opioid receptor present on the heart (periphery). Furthermore, intraspinal administration of selective µ opioid receptor antagonist, D-Phe-Cys-Tyr-D-Trp-Orn-Thr-NH2, blocked the effect of remote preconditioning suggesting the involvement of µ opioid receptors in RIPC-induced cardioprotection [20]. An earlier study of Jones et al. also verified the role of neurogenic pathway in RPCT, in which an abdominal surgical incision reduced the infarct size in the myocardium. Administration of hexamethonium, before abdominal incision, inhibited the protective effects of RPCT against myocardial infarction suggesting the involvement of nerve transmission in cardioprotection induced by RPCT. Pretreatment with lidocaine (local anesthetic), before incision, completely abolished the protective effect of RPCT, while treatment with a chemical nociceptive stimulator, capsaicin, mimicked the cardioprotective effects of RPCT confirming the role of neurogenic signaling in RPCT-induced cardioprotection [21].
Donato et al. (2013) investigated the involvement of vagus nerve and muscarinic receptors (parasympathetic nervous system) in cardioprotective effects of remote hind limb ischemic preconditioning in New Zealand rabbits. Three short cycles of hind limb ischemic and reperfusion, significantly attenuated global ischemia-reperfusion induced injury in ex vivo model of Langendorff system. To study the participation of afferent neural pathway, the different nerves including femoral, sciatic nerve and spinal cord were sectioned (T9-T10 level). In different groups, the loss of protection after sectioning of the femoral nerve, sciatic nerve and spinal cord showed the involvement of afferent neural pathways in RIPC-induced cardioprotection. The sectioning of vagus nerve and atropine administration also abolished the effect of RIPC suggesting the involvement of vagus nerve and muscarinic receptors in efferent neural pathways of remote preconditioning. Furthermore, the electrical stimulation of vagus nerve was also found to reduce the infarct size and mimic the cardioprotective effects of remote preconditioning, again suggesting that the parasympathetic nervous system constitutes an efferent neural pathway in conferring RIPC-induced cardioprotection [22]. Earlier study also showed that efferent vagal stimulation in male Wistar rats, before or even during coronary occlusion, protected the heart against ischemia-induced lethal arrhythmias through prevention of the loss of Cx43 gap-junction channels. Immunohistochemistry confirmed that the Cx43 form of gap junction was preserved during vagal stimulation and administration of atropine abolished the effects of vagal stimulation on Cx43 preservation [23]. The same group of scientists also examined the effect of vagal stimulation on ischemic insult during coronary occlusion showing that vagal stimulation significantly reduces the infarct size independent of the bradycardiac effect. In addition to its anti-infarct effect, vagal stimulation exerted beneficial effect on ventricular performance and significantly increased ATP content at end of ischemia. The beneficial effects of vagal stimulation were exerted through preservation of mitochondrial function as administration of mitochondrial permeability transition pore opener atractyloside blocked the effect of RIPC [24].
Oba et al. studied the role of renal nerve mediated release of erythropoietin in Balb/c background male mice in cardioprotective effects of RIPC. The authors also demonstrated the significant increase in the expression of HIF-1α in the border area between the medulla and cortex of kidney in RIPC subjected animals. However, no such increase was reported in animals with non RIPC stimulus. HIF1α is the main transcriptional factor of erythropoietin expression and hence, its increased expression suggests the increased levels of erythropoietin in response to RIPC. Anti-erythropoietin neutralizing antibody (100 µg) and renal nerve denervation abolished the cardioprotective effects suggesting the key role of erythropoietin expression and renal nerves in RIPC-induced cardioprotection [25]. The studies from our laboratory had also demonstrated the key role of erythropoietin and HIF1α in remote renal preconditioning-induced cardioprotection in rats [426]. The exogenous administration of erythropoietin mimicked the cardioprotective effects of RIPC, while RIPC failed to trigger cardioprotection in renal failure in rats with reduced erythropoietin levels [26]. Furthermore, administration of ethyl3,4-dihydroxybenzoate (EDHB), a selective HIF-P4H inhibitor, mimicked cardioprotective effect of remote renal preconditioning, while administration of α-ketoglutarate (HIF-P4H activator), abolished the cardioprotective effect induced by EDHB preconditioning and remote renal preconditioning. This study concluded that inhibition of HIF-P4H has an important role in remote renal preconditioning induced cardioprotection [4].
Apart from these there have other studies also suggesting the key role of neurogenic pathways in remote preconditioning-induced cardioprotection. Dong et al. demonstrated that femoral nerve section and a selective adenosine A1 receptor antagonist 8-cyclopentyl-1,diproylxanthine (DPCPX) completely abolishes the cardioprotection afforded by limb ischemic preconditioning. Accordingly, it is proposed that during limb preconditioning episodes, there is a local release of adenosine, which may activate the relevant neural pathway to induce cardioprotection [27]. The study of Jensen et al. demonstrated that the release of cardioprotective humoral circulating factor during remote ischemic preconditioning is dependent on the intact and uninjured (preserved) neural pathways in diabetic patients. The blood dialysate obtained from non-diabetic subjects, with no peripheral neuropathy, after remote preconditioning stimulus reduced the infarct size and improved hemodynamic recovery. However, the same dialysate obtained from diabetic persons suffering from neuropathy failed to induce cardioprotection suggesting that the release mechanism of humoral factor during remote preconditioning involves the intact neural pathways [28]. Song et al. described the involvement of neurogenic and sensory pathway in the cardioprotective effects of late-phase remote preconditioning of trauma (RPCT) in a murine I/R injury model. Furthermore, pharmacological experiments in transgenic mice-implicated the role of bradykinin receptors, β-adrenergic receptors, protein kinase C, and NF-κB, but not iNOS signaling in the cardioprotective effects of late RPCT (Fig. 2) [29].
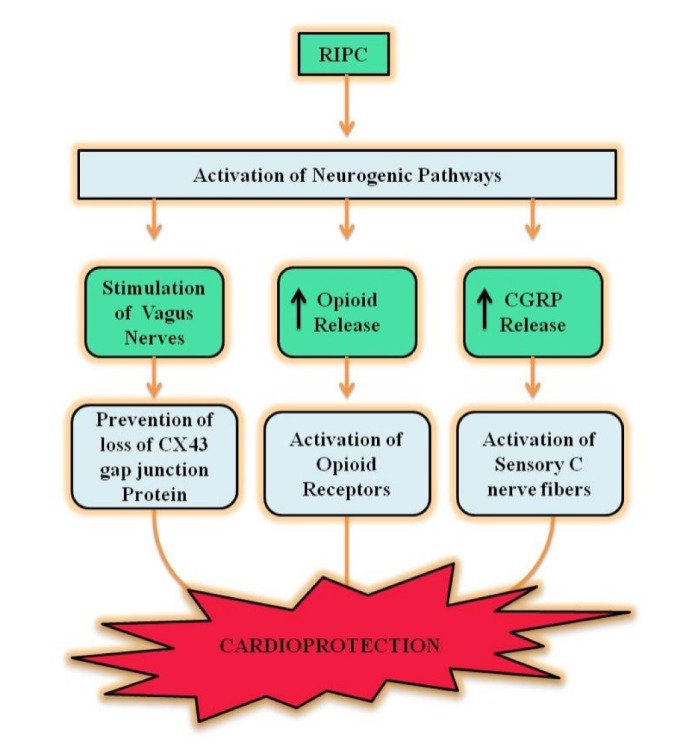 | Fig. 2RIPC activates neurogenic pathways including stimulation of vagus nerves which in turn prevents the loss of CX43 gap junction proteins to provide cardioprotective effects.Secondly, RIPC stimulus enhances opioid release and activates myocardial opioid receptors to induce cardioprotection. Furthermore, RIPC also increases CGRP release and activates sensory C nerve fibers to induce cardioprotection.
|
Go to :
SUMMARISED FINDINGS
There have been number of studies suggesting the involvement of neurogenic pathway in remote preconditioning induced cardioprotection [11]. The scientists have mainly employed the pharmacological tools including hexamethonium, (a ganglion blocker) [1113141617], Hoechst 140α, (selective B2 receptor antagonist) [14], 8-(p-sulfophenyl)-theophilline, (an adenosine receptor blocker) [16] and trimethaphan, (an autonomic ganglion blocker) [8] to demonstrate the neurogenic activation during RIPC. Furthermore, scientists have also employed nerve sectioning techniques including sectioning of femoral, sciatic nerves [1122], or spinal cord [22] to demonstrate that nerves carry the impulses from the site of application of remote ischemia to brain, which in turn convey the cardioprotective signals to heart. Amongst the mediators that may actively participate in neurogenic activation during RIPC, the role of bradykinin [14], adenosine [16] and TRPV1 channels [30] has been demonstrated. Apart from it, the key role of vagus nerve [2223] and muscarinic receptors [22]; opioid receptors in the spinal cord [20]; gap junctions [23]; erythropoietin and HIF1α [42526]; and PKCε [17] has also been demonstrated in neurogenic pathway activated during RIPC. Nevertheless further studies are required for unifying mechanisms which are activated during neurogenic activation in RIPC.
Go to :
CLINICAL IMPLICATIONS OF RIPC
RIPC treatment strategy is a major breakthrough in the cardiovascular field that has been translated into the clinical settings [2]. In clinical set-ups, RIPC stimulus is delivered via inflating (≥120 mm) and deflating the blood pressure cuff alternatively, tied on the upper arm of the individual for three to four consecutive times. RIPC is a noninvasive and safe technique that provides shielding effect against ischemia-reperfusion injury. Moreover, skeletal muscles are comparatively more resistant to ischemia-reperfusion injury [31] in comparison to other highly perfused organs including intestine and kidney. RIPC stimulus tends to reduce cardiac injury in the patients undergoing various surgical interventions including valve replacement [32], coronary angioplasty [33], coronary artery bypass grafting [34]. Furthermore, RIPC has the capability to reduce kidney injury in patients undergoing cardiac surgeries [35]. Also, RIPC reduces ischemia-reperfusion injury after liver transplantation [36] and renal transplantation [37].
Go to :
FACTORS AFFECTING RIPC-INDUCED CARDIOPROTECTION
The various factors that can affect the protective effects of RIPC in humans include aging, comorbidities and concomitant medication. Aging is a crucial factor which considerably influences RIPC-induced cardioprotective effects. Animal studies indicate that senescence reduces the preconditioning-induced protective effects in the myocardium [38]. Clinically, aging reduces preconditioning-induced cardioprotective effects in the masses [39] possibly due to deterioration of the contractile function and weakened cardioprotective signaling [40]. Also, angina prior to myocardial infarction elicits ischemic preconditioning like cardioprotective effects in the adult patients which start disappearing after aging [41]. Apparently, comorbidities including stable angina, pulmonary hypertension and type II diabetes also influence the ability of RIPC stimulus to induce cardioprotective effects. The patients with stable angina pectoris encounter transient ischemic episodes that mimic preconditioning like effect on the heart and therefore such patients have better ability to withstand myocardial infarction [42]. Hence, the patients with stable angina or peripheral arterial disease experience preconditioning like effect and may not gain additional benefit from RIPC. Also, diabetes leads to accumulation of glycosylated proteins and thus, reduces preconditioninginduced cardioprotection in these patients [43]. Moreover, long standing diabetes is associated with development of neuropathy and there is possibility that due to injury to the neural system (during neuropathy), there may be an interference with the neurogenic signaling during RIPC. Furthermore, RIPC doesn't provide cardioprotective effects against ischaemic-reperfusion injury in pulmonary hypertensive infants receiving ventricular septal defect repair [44]. Besides this, concurrent medication including sulfonylureas (oral hypoglycemic agents) may lay remarkable impact on RIPC-induced protective effects as these have the ability to inhibit mitochondrial KATP channels and possibly reduce RIPC-induced cardioprotection [45]. In addition, the outcome of RIPC is also influence by the type of anesthetic employed during surgery. The anesthetics tend to reduce the ischemic response in humans required to produce the preconditioned state and therefore may not offer additional benefit after RIPC [46].
Go to :
 XML Download
XML Download