

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sepsis is a severe medical condition caused mainly by the influx of bacteria into the blood [1]. The immune system reacts against the influx of bacteria [2]. In addition, blood clot occurs due to the immune response to the whole body [3]. Blood flow is reduced by blood clotting during, which interferes with blood, nutrients, and oxygen supply and then causes organ damage and hypoperfusion [4]. Sepsis usually alters glucose regulation in the whole body and tissue [5]. The sepsis-induced glucose imbalance is characterized by an initial hyperglycemia followed by a progressive hypoglycemia. The sepsis-induced hyperglycemia may be due to an acute early host response leading to an increase of hepatic gluconeogenesis by activation of the immune response [67]. Hyperglycemia may also be developed in septic patients due to insulin clearance leading to a reduction in insulin-mediated glucose uptake [8]. However, during the late phase of sepsis, organ dysfunction is usually occurred [9]. Furthermore, hypotension and hypoglycemia are produced eventually [10]. Hypoglycemia is observed in 16.3% of sepsis patients [11]. Moreover, the exact mechanism of sepsis-induced hypoglycemia is not well elucidated. Some previous studies have reported that hypoglycemia occurred by certain infectious diseases is associated with the limited glycogen stores (e.g., liver disease), impaired gluconeogenesis and increased peripheral glucose utilization [6121314].
Several lines of evidence have demonstrated that the blood glucose level may be one of the critical factors for rescuing from the dangers of fatality induced by sepsis. In support of the hypothesis, a recent study has demonstrated that ghrelin exerts a protective effect against sepsis-induced lethality by elevating a blood glucose level [1516]. Although these observations suggest that the blood glucose level control may be one of the important strategies, the clear conclusion on this issue has not been drawn yet. We found recently that the activation of α2-adrenergic receptors located in the spinal cord elevates the blood glucose level [17], and spinally administered clonidine protects against sepsis-induced mortality (unpublished observation). Moreover, in our previous studies we have reported that PTX produces hypoglycemic effect [181920]. However, the role of the blood glucose level on sepsis-induced mortality has not been characterized yet. Thus, the present study was designed to examine the effects of D-glucose administered orally on mortality and hypoglycemia induced by LPS/GaLN treatment. Furthermore, the role of spinally located PTX-sensitive G-proteins on the pharmacological effect of D-glucose in the regulation of mortality and the blood glucose level in sepsis animal model was examined.
Go to : 
METHODS
The experiments were approved by the Hallym University Animal Care and Use Committee (Registration Number: Hallym 2009-05-01). All procedures were conducted in accordance with the 'Guide for Care and Use of Laboratory Animals' published by the National Institutes of Health and the ethical guidelines of the International Association for the Study of Pain.
Experimental animals
Male ICR mice (M.J. LTD., Seoul, Korea) weighing 23~25 g were used for all the experiments. Animals were housed five per cage in a room maintained at 22±0.5℃ with an alternating 12 h light/dark cycle. Food and water were available ad libitum. The animals were allowed to adapt to the laboratory for at least 2 h before testing and were only used once. Experiments were performed during the light phase of the cycle (10:00~17:00 h). These experiments were approved by the University of Hallym Animal Care and Use Committee.
Oral (p.o.), intraperitoneal (i.p.) and intrathecal (i.t.) administration
Oral administration was performed with gage in a volume of 500 µl/25 g body weight. I.p. injection was conducted to anesthetized mice with the volume of 250 µl. The i.t. the administration was performed following the method of Hylden and Wilcox [2122] using a 30-gauge needle connected to a 25 µl Hamilton syringe with polyethylene tubing. The i.t. injection volume was 5 µl, and the injection site was verified by injecting a similar volume of 1% methylene blue solution and determining the distribution of the injected dye in the spinal cord. The dye injected i.t. was distributed both rostrally and caudally but with short distance (about 0.5 cm from the injection site) and no dye was found visually in the brain. The success rate for the injections was consistently found to be over 95% before the experiments were done.
Blood glucose measurement
The blood was collected shortly as much as possible with a minimum volume (1 µl) from the tail-vein. The glucose level was measured using Accu-Chek Performa blood glucose monitoring system (glucometer) (Roche Diagnostics, USA). The blood glucose level was measured at 0.5, 1, 3, 6, 12, 24, 36, 48, 72, 96 h after oral administration with D-glucose (n=10).
Drugs
D-Galactosamine, Lipopolysaccharide, and D-glucose were purchased from Sigma Chemical Co. (St. Louis, MO, USA). Pertussis toxin was purchased from Research Biomedicals (Natick, MA, USA). All drugs used for injection were dissolved in sterile saline (0.9% NaCl with saline or test drugs. The pretreatment time was the same solution). All drugs were prepared just before use. Blood glucose meter, lancing device and strips were purchased from Roche Diagnostics (Accu-Chek Performa, Germany).
Statistical analysis
Statistical analysis was carried out by ANOVA (Bonferroni test) for multiple comparisons, by using GraphPad Prism Version 4.0 for Windows (GraphPad Software, San Diego, CA, USA). p-values less than 0.05 were considered to indicate statistical significance. All values were expressed as the mean±S.E.M. In our study, we established the mean blood glucose value of the control group through many experiments under matching conditions. Selected mice of established blood glucose level were then used in replication experiments.
Go to :
RESULTS
Effect of D-glucose fed orally on sepsis-induced mortality and blood glucose level
To produce sepsis, the mixture of GaLN (0.6 g/10 ml) and LPS (27 µg/27 µl) was treated i.p. To assess the possible protective effect of D-glucose against sepsis-induced mortality, D-glucose (from 1 to 8 g/kg) was fed orally 30 min prior to GaLN/LPS administration As shown in Fig. 1A, the mortality rate in GaLN/ LPS-induced sepsis group, was 50% at 12 h, 70% at 24 h up to 96 h after GaLN/LPS administration. Although D-glucose at the lowest dose (1 g/kg) used did not affect sepsis-induced mortality, D-glucose at higher amounts (2, 4 and 8 g/kg) reduced mortality rate in a dose-dependent manner. In the sepsis group, the blood glucose level began to fall 1 h and was further down-regulated up to 4 h after sepsis induction as shown in Fig. 1B. D-glucose feeding at the dose of 1 g/kg did not affect the blood glucose level in sepsis group. However, higher amounts (from 2 to 8 g/kg) of D-glucose increased the blood glucose level in a dose-dependent manner. At highest dose (8 g/kg) of D-glucose, the blood glucose level reached at its highest level 30 min and maintained up to 1 h and began to return toward the control level 2 h after oral feeding.
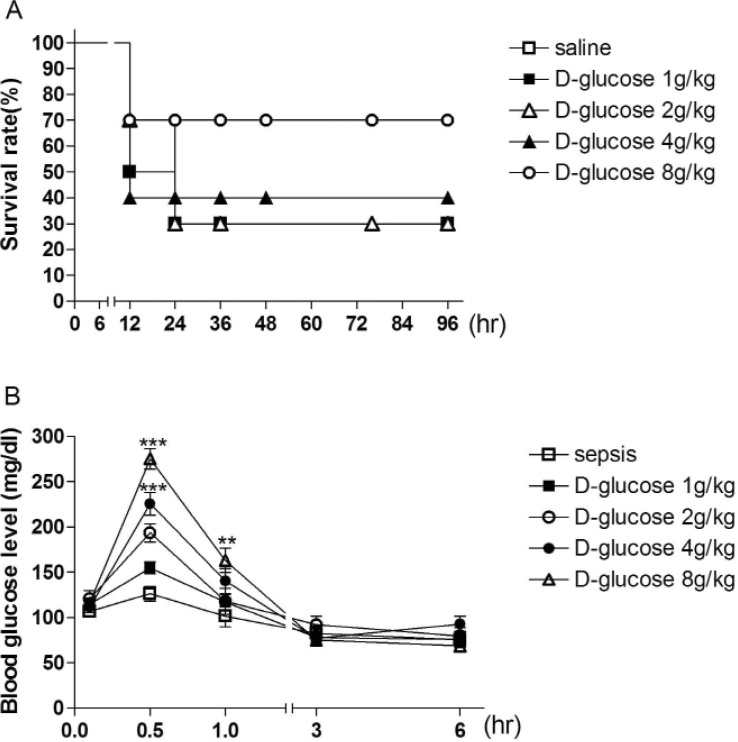 | Fig. 1Dose-dependent effects of D-glucose on mortality and hypoglycemia induced by sepsis.Mice were orally fed with various amounts (from 1 to 8 g/kg) with D-glucose 30 min prior to i.p. administration with GaLN (0.6 g/10 ml)/LPS (27 µg/27 µl). (A) The mortality rate was measured at 12, 24, 36, 48, 72, 84 and 96 h after GaLN/LPS injection. (B) The blood glucose level was measured in sepsis mice model after various doses of D-glucose (1~8 g/kg) at 30 min, 1 h, 3 h and 6 h. The number of animals used for each group was 10 (***p < 0.001; compared to sepsis group, **p<0.01; compared to sepsis group).
|
Effect of D-glucose post-treated orally on sepsis-induced mortality and blood glucose level
Since pretreatment of D-glucose was effective in protecting against sepsis-induced mortality, first, D-glucose at a dose of 8 g/kg was post-treated orally at 1, 3, 6, 9, and 12 h after GaLN/ LPS administration and its effect on sepsis-induced mortality and blood glucose profile was observed. As revealed in Figs. 2A and 2B, D-glucose post-treated 1 or 3 h after GaLN/LPS administration significantly protected sepsis-induced mortality. However, the protective effect of D-glucose against the sepsis-induced mortality was reduced in the groups post-treated at 6, 9, or 12 h after sepsis induction (Figs. 2C, 2D, and 2E). As revealed in Figs. 3A and 3B, D-glucose post-treated at 1 or 3 h after GaLN/ LPS administration was able to increase the blood glucose level in sepsis group. However, 6, 9, or 12 h post-treatment with D-glucose did not affect the blood glucose level in sepsis group (Figs. 3C, 3D, and 3E).
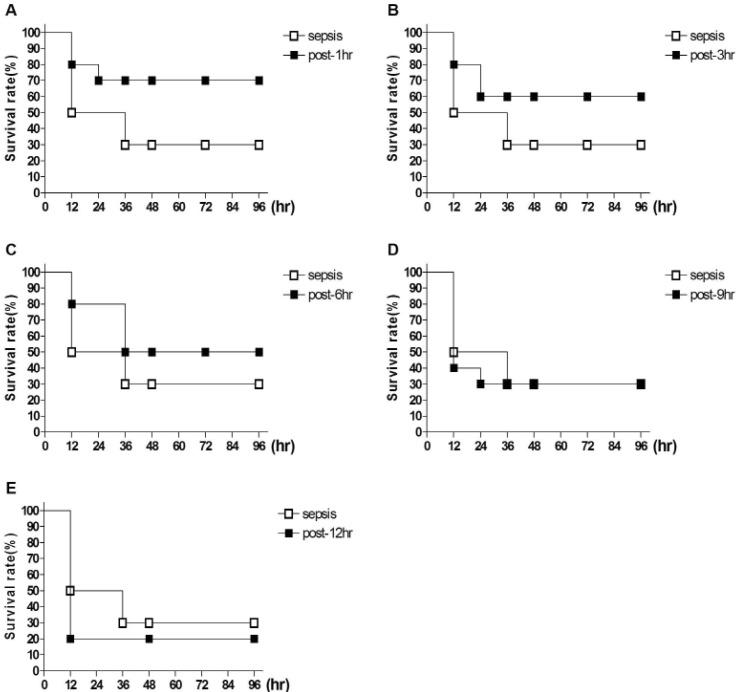 | Fig. 2Effect of D-glucose post-treated orally on sepsis-induced mortality.The mice were orally fed with D-glucose (8 g/kg) at 1 (A), 3 (B), 6 (C), 9 (D) and 12 (E) h after i.p. administration with GaLN (0.6 g/10 ml)/LPS (27 µg/27 µl). The mortality rate was counted at 12, 24, 36, 48, 72, 84 and 96 h after GaLN/LPS injection. The number of animals used for each group was 10.
|
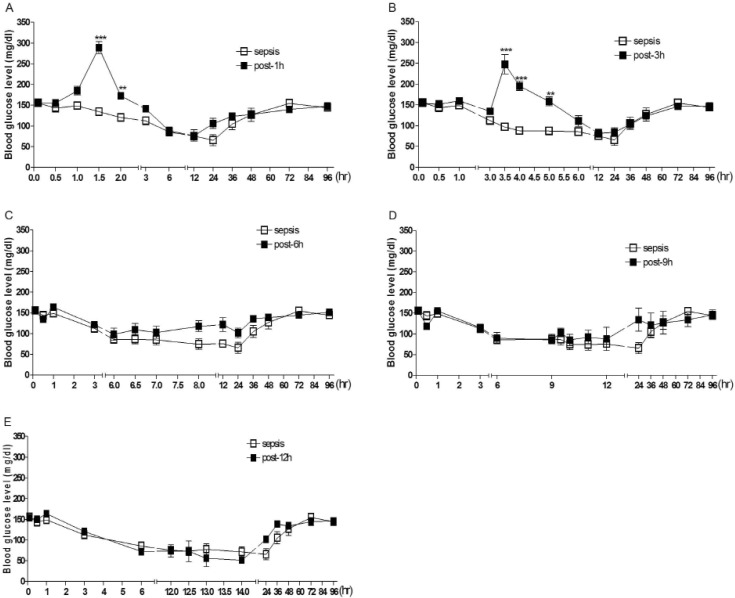 | Fig. 3Effect of D-glucose post-treated orally on sepsis-induced hypoglycemia.The mice were orally fed with either D-glucose (8 g/kg) at 1 (A), 3 (B), 6 (C), 9 (D) and 12 (E) h after i.p. administration with GaLN (0.6 g/10 ml)/LPS (27 µg/27 µl). The blood glucose level was measured at various times after GaLN/LPS injection. The number of animals used for each group was 10. (***p,#x003C;0.001; compared to sepsis group, **p,#x003C; 0.01; compared to sepsis group).
|
Effect of i.t. pretreatment with pertussis toxin on pharmacological responses of D-glucose in sepsis model
To examine if spinal inhibitory G protein is involved in D-glucose-induced survival, and hyperglycemic effects in sepsis model, the effect of PTX pretreated i.t. on D-glucose-induced hyperglycemic and survival effects in sepsis model was investigated. PTX (0.1 µg/0.5 µl) was pretreated once for 6 days, and D-glucose (8 g/kg) was administered orally. The i.t. treatment with PTX alone caused a slight hypoglycemic effect as shown in (Fig. 4B). The i.t. pretreatment with PTX attenuated D-glucose-induced hyperglycemic effect and protective effects against mortality produced by sepsis (Figs. 4A and 4B).
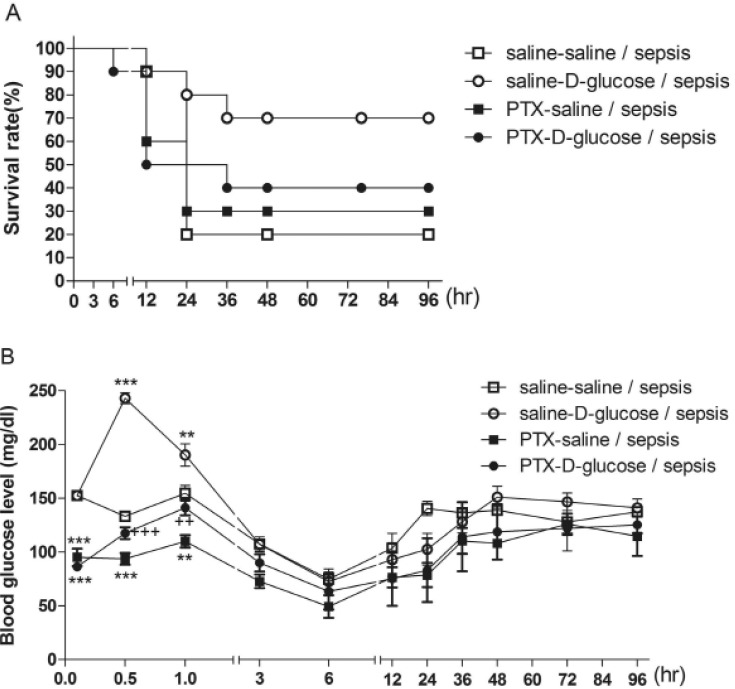 | Fig. 4Effect of i.t. pretreatment with PTX on D-glucose-induced survival and hyperglycemic effects in sepsis model.Mice were pretreated i.t. once with either saline or PTX (0.1 µg/0.5 µl) once for 6 days and D-glucose (8 g/kg) was orally fed 30 min prior to i.p. administration with GaLN (0.6 g/10 ml)/LPS (27 µg/27 µl). The mortality rate (A) was measured at 12, 24, 36, 48, 72, 84 and 96 h after GaLN/LPS injection. the blood glucose level (B) was measured at various times after GaLN/LPS injection. The number of animals used for each group was 10 (***p,#x003C;0.001; **p,#x003C;0.01; compared to Saline+Saline/sepsis group, +++p,#x003C;0.001; ++p,#x003C;0.01; compared to Saline+D-glucose/sepsis group).
|
Go to :
DISCUSSION
Several studies have previously reported that the hypoglycemia usually occurs during the sepsis [6121323]. In addition, several lines of evidence have demonstrated that the control of the blood glucose level could be a beneficial strategy to reduce the sepsis-induced lethality [2425]. Furthermore, even up-regulation of the blood glucose level exerts a protective effect against sepsis-induced mortality is evidenced in other studies in that ghrelin, which produces hyperglycemia, is able to reduce the mortality rate found in cecum ligation and perforate (CLP)- or endotoxininduced sepsis models [1516]. To examine this hypothesis, we examined the effects of various amounts of D-glucose feeding on sepsis-induced mortality and the blood glucose level. In the present study, we found that oral feeding of D-glucose from 2 to 8 g/kg can significantly improve the GaLN/LPS sepsis-induced mortality rate in a dose-dependent manner. Moreover, we observed that that post oral administrations with D-glucose (8 g/ kg) up to 3 h after sepsis induction show the protective effect against sepsis-induced mortality. However, post-treatment with D-glucose (8 g/kg) at 6, 9, and 12 h after sepsis production was not significantly effective to prevent the mortality induced by sepsis. This finding suggests that the critical time of period for a protective effect of D-glucose against sepsis-induced mortality appears to be located between 3 and 6 h after sepsis induction.
In general, hypoglycemia is produced during the severe sepsis [142426]. In the present study, we found that the blood glucose level began to fall 1 h and was continuously further down-regulated up to 4 h after sepsis induction. We observed that higher amounts (from 2 to 8 g/kg) of D-glucose cause an elevation of the blood glucose level in a dose-dependent manner. This hyperglycemic effect of D-glucose feeding is still manifested even in the sepsis group post-treated with D-glucose up to 3 h. However, interestingly, oral post-treatment with D-glucose at 6, 9, or 12 h after sepsis induction is not able to cause a hyperglycemia, suggesting that the organs of the body cannot work or perform for normal function, for example, in the regulation of the blood glucose level at 6 h after sepsis induction. This finding demonstrates that the production of hyperglycemia by D-glucose feeding up to 3 h appears to be required for the survival from sepsis-induced mortality. Taken together these observations, we propose a hypothesis that D-glucose feeding may produce the protective effect against sepsis-induced mortality by counteracting against the hypoglycemic effect induced by sepsis. The findings observed in the present study are supported by our recent studies. We found recently that spinal administration of clonidine, an a–2 adrenergic receptor agonist, causes a profound hyperglycemia and shows a protective effect against sepsis-induced mortality in a similar pattern of pharmacological action observed in the present study [unpublished observation]. Furthermore, systemic injection of clonidine also exerts a protective effect against fatality observed in CLP sepsis model [23].
Some studies have examined the influence of diabetes on sepsis patients. However, the findings are somewhat conflicting. Some of the studies showed the harmful effect of diabetes [27282930], other studies have shown no influence of diabetes [313234], and some other studies represent protective effect [35,36,37]. Some clinical studies have shown that hyperglycemia is associated with high mortality in various groups of hospitalized patients [383940]. Targeting normoglycemia with the use of continuous insulin infusions improves outcomes in a selected group of critically ill patients [4142]. Our present study indicated that hyperglycemia improves the survival rate in sepsis mouse model. Previous in vitro studies have shown that acute fluctuations of glucose can induce endothelial cell damage and apoptosis [43]. Whereas, some clinical studies have also shown a coalition between hypoglycemia and increased mortality among ICU (Intensive Care unit) patients [4445]. There is insufficient information to determine the optimal blood glucose level in the septic patient [46]. However, whether the maintenance of the blood glucose level just up to the normal level, not to a hyperglycemic state, is able to save the sepsis-induced mortality should be further characterized in the future study.
We found in the present study that spinally pretreated PTX attenuates the hyperglycemic and survival effects induced by D-glucose in sepsis model. This result suggests that inhibitory G-protein located at the spinal cord appear to be involved in the production of hyperglycemia induced by D-glucose-feeding. Several lines of evidence have previously demonstrated that PTX-sensitive G-proteins are involved in the production of hypoglycemia. For example, PTX administered systemically produces a hypoglycemic effect in in vivo study and in in vitro study PTX appears to increase the secretion of insulin [47,48,49,50]. In addition, we have recently reported that spinal administration with PTX exerts a persistent hypoglycemia in a long-term manner [1819]. Although the exact mechanism is not fully understood yet, it is speculated that some endogenous factors are activated after D-glucose feeding triggering their action on spinal PTX-sensitive inhibitory G proteins, in turn, leading to produce a hyperglycemia. It is suggested that blocking effect of PTX against the hyperglycemic effect induced by D-glucose appears to be responsible for reversing survival effect induced by D-glucose in sepsis model.
In conclusion, based on the results found in the present study, we propose that the production of a hyperglycemia induced by oral glucose feeding might be a good therapeutic strategy for the protection against sepsis-induced mortality.
Go to :
 XML Download
XML Download