

 PDF
PDF ePub
ePub Citation
Citation Print
Print


ABBREVIATIONS
MMC
mitomycin C
5-FU
5-fluorouracil
VEGF
vascular endothelial growth factor
ECM
extracellular matrix
HTFs
human Tenon's fibroblasts
TEM
transmission electron
microscopy
DMEM
Dulbecco's modified Eagle's medium
CO2
carbon dioxide
D-PBS
Dulbecco's PBS
MTT
3-[4,5-dimethylthiazol-2-yl]-2, 5-diphenyl tetrazolium bromide
LDH
lactate dehygrogenase
PIP
procollagen type I C terminal propeptide
MMP
matrix metalloproteinase
INTRODUCTION
Pterygium is a degenerative conjunctival condition related to fibrovascular proliferation [12]. The main goal of pterygium surgery is to prevent postoperative recurrence. However, several reports have suggested a high recurrence rate after pterygium surgery ranging between 7.5% and 44.4%, which undermines current operative methods and adjuvant treatments [345].
Several intra- and post-operative treatments, including mitomycin C (MMC), 5-fluorouracil (5-FU), and corticosteroids, have been recommended to prevent postoperative pterygium recurrence [6]. Because a pterygium is composed of fibrovascular proliferative tissue and postoperative recurrence is related to new vessels formation [2], fibrovascular inhibitors may affect the formation and progression of pterygium. Recently, bevacizumab (Avastin, Genentech, South San Francisco, CA), a recombinant, humanized anti-vascular endothelial growth factor (VEGF) antibody, is used to prevent pterygium recurrence after surgery. Many studies have suggested that bevacizumab has anti-inflammatory and anti-proliferative effects on fibrovascular pterygium tissue [789]. However, the efficacy of bevacizumab treatment on pterygium tissue remains still controversial.
To date, none of the studies have evaluated the effective concentrations of bevacizumab contingent upon pterygium recurrence, especially in cell levels. In addition, no study has compared the difference in extracellular matrix (ECM) synthesis after bevacizumab exposure between primary and recurrent pterygium. Here, we investigate the biologic effects of bevacizumab on cultured human Tenon's fibroblasts (HTFs) obtained from primary and recurrent pterygium. The anti-fibrotic effect of bevacizumab on fibrovascular pterygium tissue at varying concentrations was specifically examined. The effect of bevacizumab on ECM (e.g., collagen and laminin) synthesis was also evaluated using immunoassays. Finally, HTFs were examined by phase-contrast and transmission electron microscopy (TEM) to identify cellular morphological changes caused by bevacizumab exposure.
METHODS
Human Tenon fibroblasts were obtained from explanted subconjunctival Tenon's capsule that was isolated during primary and recurrent pterygium surgery. The study was approved by the Ethics Committee of Pusan National University Hospital (IRB No. E-2014129). All study conduct adhered to the tenets of the Declaration of Helsinki and written informed consent was obtained from all patients.
Cell culture and preparation
Primary cultures of HTFs were obtained from a 2×2 mm piece of excused tissue. All tissue were prepared for culture in 35 mm Petri tissue-culture dishes that contained Dulbecco's modified Eagle's medium (DMEM; Gibco BRL, Grand island, NY, USA) supplemented with 10% fetal bovine serum (Gibco BRL), L-glutamine 2 mM, penicillin (20 ug/mL; Sigma-Aldrich, St. Louis, MO, USA), and streptomycin (200 g/mL; Sigma-Aldrich). Cells were incubated at 37℃ in a humidified environment of 95% air and 5% carbon dioxide (CO2). The culture medium was changed every 2 to 3 days. Cells were then enzymatically detached with 0.25% trypsin and 0.002% EDTA (Irvine Scientific, Santa Ana, CA, USA) at 37℃. After sitting for 10 minutes and being washed once with Dulbecco's PBS (D-PBS; Gibco BRL), HTFs were centrifuged at 400 G for 10 minutes. The supernatant was removed and fresh medium was added. The cell suspension was counted in a hemocytometer, and 5×103 cells/well were plated using 96-well tissue culture plates. The second to fourth-passage HTFs were used in all experiments. After incubation in 1 ml of culture medium at 37℃ (5% CO2, 95% air), cells were allowed to attach to the bottom of the well for 24 hours. The effect of a drug on HTFs can be underestimated when cells are too dense. Therefore, cells were cultured for approximately 2~3 days to allow the cells to cover approximately 80~90% of the medium. The same procedure was performed in the recurrent pterygium HTFs.
Cell metabolism assay
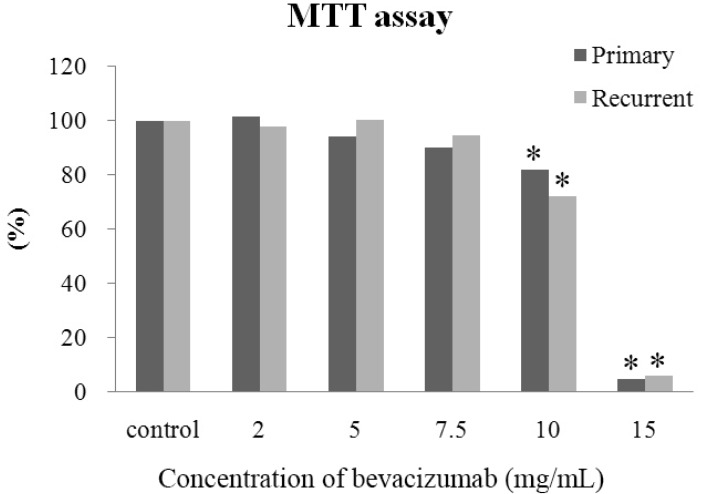
The metabolic activity of HTFs was determined using the colorimetric tetrazolium salt 3-[4,5-dimethylthiazol-2-yl]-2, 5-diphenyl tetrazolium bromide (MTT; Sigma-Aldrich) test [10]. The MTT assay is based on purple formazan production from a methyl tetrazolium salt by viable cell mitochondrial enzymes. Cultured cells, at a concentration of 4,000 cells/well, were seeded in 96-well culture plates and allowed to form a monolayer over 24 hours. Cells were then exposed to 150 µL of DMEM medium containing 2.0, 5.0, 7.5, or 15.0 mg/mL concentration of bevacizumab for 24 hours. After bevacizumab exposure, cells were washed twice with D-PBS and were incubated in culture media for 24 hours. The MTT assay was then performed. The balanced salt solution treated group was used as a control.
At the end of the incubation period, the MTT solution was carefully aspirated, taking care not to disturb the purple formazan crystals at the bottom of each well. The formazan reaction product was dissolved by adding 150 µL of dimethyl sulfoxide (Sigma), and the optical density of each well was measured using an automatic plate reader (Molecular Devices, Sunnyvale, CA, USA) with a 570 nm test wavelength and a 690 nm reference wavelength. All cell metabolism assays were repeated in triplicate.
Cell metabolism was calculated as the mean absorption rate of each exposure time and concentration and was calculated using the following formula:
Data were analyzed for statistical significance using the Wilcoxon signed rank test. Statistical significance was defined at p<0.05.
Lactate dehydrogenase assay for cell viability
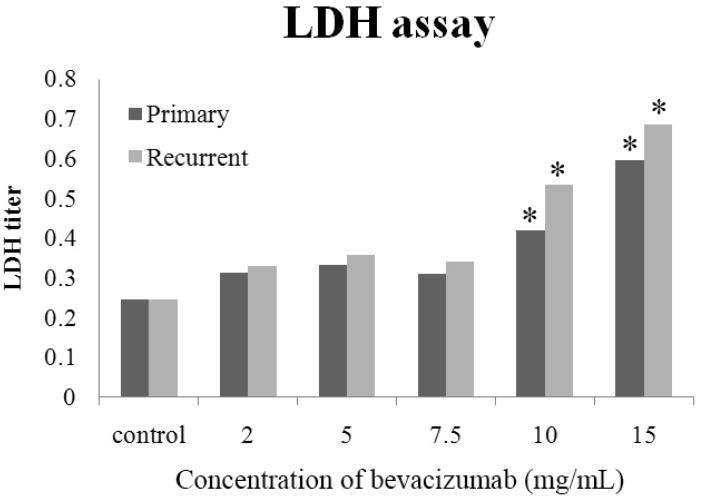
Leakage of lactate dehygrogenase (LDH) from the cytoplasm to the extracellular medium was measured via the LDH assay. The presence of LDH (exclusively located in the cytoplasm) in cell culture medium represents cell membrane damage. For the LDH assay, 4.0×103 HTFs/mL were seeded in each well of 96-microtiter plates. Twenty-four hours after cell seeding, cells were exposed to each concentration of bevacizumab (2.0, 5.0, 7.5, and 15.0 mg/mL). The LDH titer of each drug was assessed 24 hours after adding bevacizumab to the medium. After 24 hours, supernatant was collected from each well. The cell monolayer was then treated with a cell lysis solution for 30 min at room temperature to lyse the cells. Cells and lysate were then collected. The LDH activity was measured in both the supernatant and the cell lysate fractions using CytoTox 96 (Promega, Madison, WI, USA), a nonradioactive cytotoxicity assay kit, in accordance with the manufacturer's instructions. Absorbance was measured at a wavelength of 490 nm using a 96-well plate enzyme-linked immunosorbent assay reader. The LDH activity is proportional to color intensity and is expressed as optical density. The balanced salt solution treated cells and supernatant were used as controls. To evaluate the statistical significance of cell viability differences, data were analyzed using the Wilcoxon signed rank test. Statistical significance was defined at p<0.05.
Extracellular matrix evaluations
Cultured cells at a concentration of 4,000 cells/well were seeded in 24-well culture plates and allowed to form a monolayer for 24 hours. Cells were then exposed to 150 µL of DMEM that contained various bevacizumab concentrations, as described earlier. After exposure to bevacizumab for 24 hours, the medium was removed and stored at -80℃. Levels of procollagen type I C terminal propeptide (PIP), laminin, matrix metalloproteinase (MMP)-1, and MMP-2 were then determined using ELISA kits (Takara, Tokyo, Japan).
Cell morphology evaluations
Cellular morphological changes were investigated using phase-contrast microscopy (Nikon, Japan). Cells (5×104 cell/mL/well) that were grown to confluence on 24-well plates were seeded at 500 µL/well on six-well plates. These cells were then incubated in DMEM in 5% CO2 and 95% air at 37℃, reaching subconfluence in the plates. After exposure to each tested concentration of bevacizumab for 24 hours, HTFs were monitored using an inverted phase-contrast light microscope equipped with a photographic system.
Cells were prepared for TEM as they were for phase-contrast microscopy. Cells were then rinsed with 0.1 M sodium cacodylate buffer and fixed with Karnosky fixative (2% paraformaldehyde, 2.5% glutaraldehyde, and 0.1 M sodium cacodylate buffer) for 2 hours. After being rinsed with 0.1 M sodium cacodylate buffer three times, cells were post fixed with 0.1% osmium tetroxide and deturgenced with an ethanol solution. Next, specimens were embedded in an Epon® 812 (Shell. Chemical Co., USA) mixture and sectioned into 60~80 nm thick slices. Slices were then stained with uranyl acetate and lead citrate and examined with TEM (JEOL 1200EX, Tokyo, Japan).
RESULTS
Cell metabolism
Both primary and recurrent pterygium HTFs had a dose-dependent response to bevacizumab. When both types of HTF were exposed to 10.0 and 15.0 mg/mL concentration of bevacizumab, metabolic activity significantly decreased compared to that measured in control HTFs (primary HTFs: p=0.04, recurrent HTFs p<0.001). There was no significant difference of cellular metabolism between primary and recurrent pterygium HTFs at any concentration of bevacizumab (Fig. 1).
Cell viability
The LDH activity of both HTFs had a dose-dependent cytotoxic response to bevacizumab. When exposed to 10.0 and 15.0 mg/mL concentration of bevacizumab, the cellular viability of both HTFs was significantly less than that of control HTFs (primary HTFs: p=0.03, recurrent HTFs: p<0.001). The LDH titers were not significantly different between primary and recurrent pterygium HTFs at any bevacizumab concentrations (Fig. 2).
Extracellular matrix production
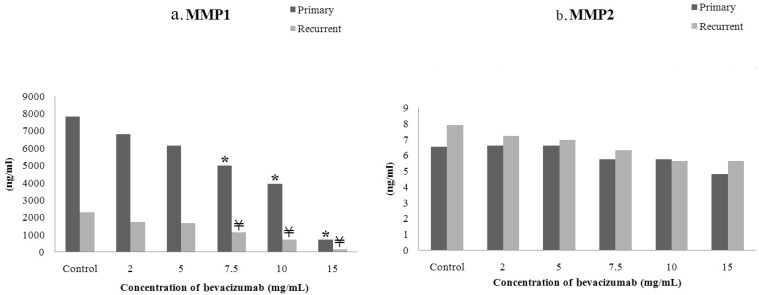
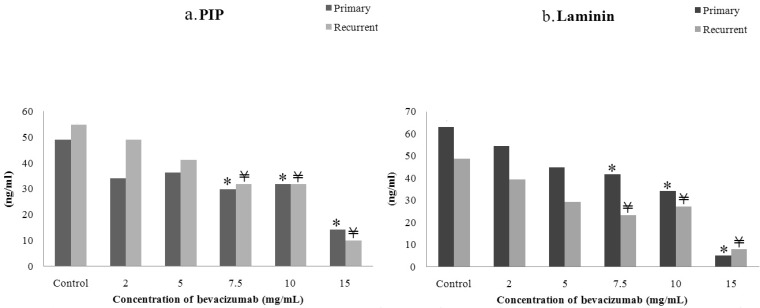
After exposure to bevacizumab, the levels of MMP-1, MMP-2, PIP, and laminin all decreased in a dose-dependent manner (Fig. 3 and 4). The MMP-1, PIP, and laminin production measured from primary and recurrent pterygium was significantly different from that of control HTFs at bevacizumab concentration of 7.5, 10.0, and 15.0 mg/mL (Fig. 3 and 4). Interestingly, MMP-1 level in primary pterygium HTFs were significantly higher than that of the recurrent pterygium HTFs (Fig. 3a).
Morphologic changes in human Tenon's fibroblasts following bevacizumab exposure
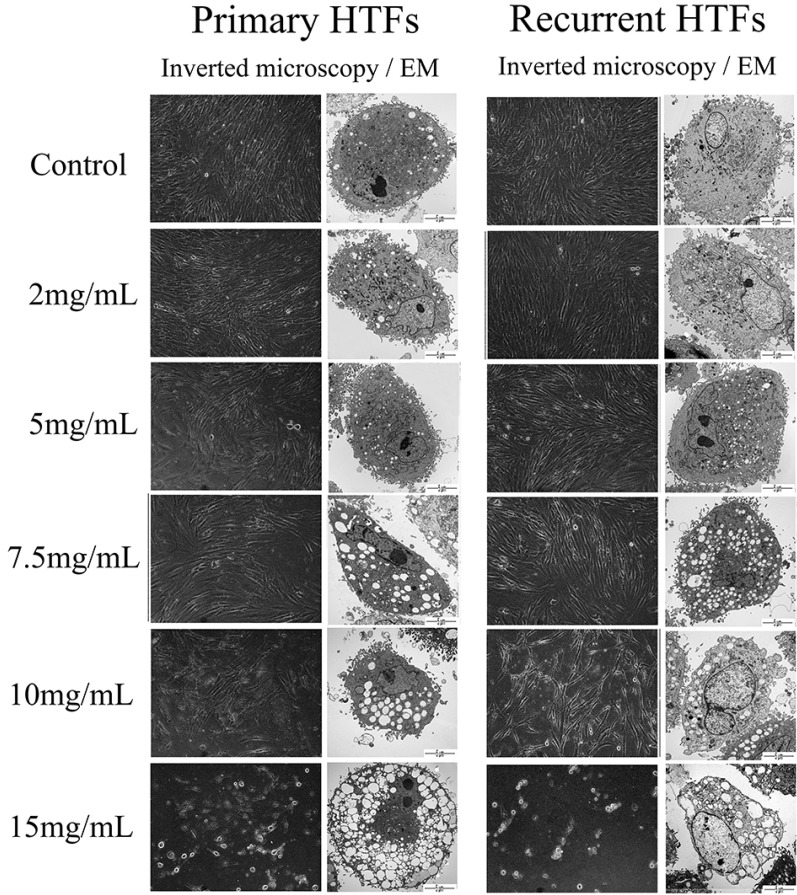
Before the bevacizumab application, inverted phase-light microscopy showed that HTFs were uniform and densely distributed in the culture medium. After 24 hours exposure to 2.0 mg/mL concentration of bevacizumab, primary and recurrent pterygium HTFs had similar culture densities as that of control HTFs. When HTFs were exposed to bevacizumab concentrations greater than 7.5 mg/mL, a significant reduction in cellular density was observed and significant morphological changes developed. Interestingly, only primary pterygium HTFs had a reduction in cellular density at a bevacizumab concentration of 5.0 mg/mL. Significant changes in cellular density and morphology both occurred at bevacizumab concentrations greater than 7.5 mg/mL (Fig. 5).
Control HTFs had plasma membranes with microvilli, a nuclear membrane, regular cytoplasm, epithelial cell nuclei, and subtle mitochondria and rough endoplasmic reticulum enlargements. However, after 24 hours of bevacizumab exposure, changes in HTFs cytoplasm and nucleus were observed. These morphological changes included dilated rough endoplasmic reticulum, enlarged mitochondria, microvilli loss, cytoplasmic membrane disruption, cytoplasmic vacuole formation, and nuclear damage. Chromatin margination of the nucleus and severe enlargement of mitochondria and cytoplasmic organelles was observed, in both types of HTFs following exposure to bevacizumab concentrations greater than 7.5 mg/mL (Fig. 5).
DISCUSSION
Many studies have shown VEGF to be increased during pterygium development [111213], but studies examining bevacizumab therapy for pterygium have reported mixed results [71415]. Systemic administration of bevacizumab has a small but significant risk of thromboembolic events [16]. As much smaller dose is administered topically to treat pterygium, we assume that this mode of administration could have some localized side effects included punctuate epithelial erosions, temporary conjunctival injection, or elevated intraocular pressure related with adjunctive ocular injection without systemic side effects. In addition, there has been some concern on the safety of bevacizumab used on the level of cells at anterior and posterior segment [171819].
Based on our study results, anti-fibrotic effect of bevacizumab on HTFs increases in a dose-dependent manner. And the effect especially increased at more than 10 mg/mL of bevacizumab concentrations. Morphological analysis also showed a significant reduction in cellular density and a significant change in cell organelles, after exposure to bevacizumab concentrations more than 7.5 mg/mL. These results are similar with those obtained by O'Neill et al. [20], who reported in vitro bevacizumab-induced fibroblast cell death at the bevacizumab concentrations greater than 7.5 mg/mL.
Excessive fibrovascular proliferation is the most common cause of postoperative pterygium recurrence. Adjuvant MMC and 5-FU are clinically used to inhibit fibrosis and improve surgical outcomes [6], but these agents are associated with serious postoperative complications, including corneal and scleral melt. Our study indicates that bevacizumab at concentrations greater than 7.5 to 10.0 mg/mL has a significant anti-fibrotic effect. And this result suggests that bevacizumab concentrations greater than 7.5 to 10.0 mg/mL might be used as a useful adjuvant treatment for both primary and recurrent pterygium.
Matrix metalloproteinases are enzymes that degrade the ECM. The MMPs can be divided into five subgroups, including collagenases (MMP-1, MMP-8, MMP-13), which are capable of cleaving intact fibrillar collagen, and gelatinases (MMP-2, MMP-9), which can further degrade collagen and basement membrane collagen type IV [21]. Matrix metalloproteinases are known to play an important role in tissue remolding, healing, and angiogenesis [2122], and the expression of several types of MMPs is increased in pterygium tissue [2324]. However, some controversy exists on the levels of MMPs in a pterygium and its fibroblasts [23242526]. In our study, the level of MMP-1 significantly decreased after exposure to bevacizumab concentrations greater than 7.5 mg/mL. But, MMP-2 level was not affected by any concentration of bevacizumab which were examined in our study. This evidence suggests that the effect of bevacizumab is related to a reduction in collagenase, and not in gelatinase. As the primary HTFs produces larger amounts of MMP-1 compared to recurrent HTFs, the susceptibility of primary HTFs to bevacizumab at lower concentrations is not surprising. The significant reduction in MMP-1 level in primary pterygium HTFs is likely to be related to the faster cellular density changes in primary pterygium HTFs after exposure to 5.0 mg/mL concentration of bevacizumab. The VEGF is generally thought to induce fibrosis mainly through promoting angiogenesis [712]. Anti-fibrotic effect induced by anti-angiogenic effect of bevacizumab might have reduced the MMP-1 level which is resulted from the pathologic angiogenesis and fibrosis of pterygium tissue. Based on the result of this study, the levels of MMP-1 which was produced from HTFs decreased in a dose-dependent manner after exposure to bevacizumab. This presumption matches with the O'Neill et al. [20]'s report that bevacizumab inhibits fibroblast proliferation and induces fibroblast cell death in addition to its effect on angiogenesis. Although our study did not investigate the anti-fibrotic characteristic effect of bevacizumab on HTFs, higher concentrations of bevacizumab have caused more severe morphological damages of HTFs, compared to the lower concentrations. Morphological damages, including cytoplasmic membrane disruption, cytoplasmic vacuole formation, and nuclear damage, enable us to assume that more cell death is estimated after higher concentrations of bevacizumab compared to lower concentrations. However, additional studies are needed to confirm these findings. In addition, even before the bevacizumab exposure, primary pterygium HTFs showed significantly higher MMP-1 level compare to that of recurrent pterygium. This result is supported by our previous report showing a significant increase in collagenase level in primary pterygium compared to recurrent pterygium [27]. The difference of MMP-1 level between primary and recurrent pterygium shown in this study may be related to the immaturity of pterygium fibroblasts [27]. Fibrillar collagen is synthesized in fibroblasts as procollagen, containing an N-terminal and a C-terminal propeptide [28]. The 100-kDa PIP is cleaved from procollagen type I during synthesis of fibril-forming collagen type I. Therefore, serum concentration of PIP is a useful marker of fibrosis [29]. Laminins are major proteins in the basal lamina and play an important role in cell differentiation, migration, adhesion, and survival [30]. Laminins are also considered to be noninvasive biomarker of fibrosis [31]. Procollagen type I and laminin showed a significant decrease after exposure to bevacizumab concentration greater than 7.5 mg/mL, suggesting that the anti-fibrotic effect of bevacizumab is related to ECM production. Identifying morphological differences between primary and recurrent pterygium tissue is difficult. Our study showed considerably higher ECM production in primary pterygium than in recurrent pterygium, especially in MMP-1 level. This result might be useful in discriminating between primary and recurrent pterygium tissue, which will enable further studies related to pterygium recurrence.
Our study showed a dose-dependent inhibitory effect of bevacizumab in both primary and recurrent pterygium HTFs. A significant increase in the anti-fibrotic effect, changes in the morphology, and reduction in the collagenase activity, occurred at bevacizumab concentration greater than 7.5 mg/mL. The inhibitory effect of bevacizumab on MMP-1 related with collagenase activity in primary pterygium HTFs was significantly higher than that of recurrent pterygium.
 XML Download
XML Download