

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Genes that have the potential to affect physical fitness consist of types sensitive to training [1,2,3,4]. It is considered that the gene polymorphism of the angiotensin converting enzyme (ACE), found in the heart and the skeletal muscles, is closely related to the physical fitness level based on cardiopulmonary function and anaerobic performance [5,6]. The renin-angiotensin system adjusts blood pressure, body fluid and electrolyte concentrations, and is known to affect cardiopulmonary endurance. It is reported that individuals with the II genotype have lower blood pressure and higher cardiopulmonary endurance than those with the DD genotype, who have increased risk of developing cardiovascular diseases [7]. Yet ACE genotype is not a determinant of elite sprint athlete status [8]. Different results [9], however, have been reported as a result of the differences in the physical features among races, gender and diseases [10]. The related mechanism is largely unknown [11].
The α-actinin-3 protein, expressed from the ACTN3 gene, is the main component of the Z line, where both tips of the myomere where the actin filament is crossed are known to be influential factor on exercise ability of exerting muscular strength. It is a main protein required to exert maximum muscular strength, expressed from type II muscular fibers and distinguished from the α-actinin-2, the isoform expressed from all the muscular fibers of the slow and the fast muscles [12,13]. While the XX genotype (R577X), one of the gene polymorphisms of the ACTN3, does not express α-actinin-3 in the fast twitch muscle fibers, the RR genotype (577R) normally expresses α-actinin-3 in fast-twitch myofibers which is considered to be an influential part in producing forceful muscle contractions at high velocity that can be advantageous for sports requiring anaerobic muscular strength and power [14]. Yang et al. [13] showed that the Australian sprinter group had significantly lower frequency of the XX genotype of the ACTN3 gene than the general group, and higher RR genotype. However, the endurance group had much higher frequency in the XX genotype [13], indicating that the 577R opponent of the ACTN3 gene affects the sprint genotype. But the Kenyan and Ethiopian athletes with strength in the endurance show the XX genotype of the ACTN3 gene polymorphism similar to general group [15], and ACTN3 XX genotype is negatively associated with elite sprint athlete status, the underlying low frequency in these populations eliminates the possibility of replicating this association in Jamaican and US African American sprinters [8]. As previous findings have not always been replicated, the extent to which ACTN3 or ACE genotypes influence physical fitness-related phenotypes varies. The genotype and some phenotype might be related each other but the causality could not claim.
As mentioned above, despite evidences showing differences between aerobic and anaerobic exercise performance depending on the polymorphism of the ACE and the ACTN3 genes in skeletal muscles, more studies are required to understand genes and exercise training adaptation [4,16]. In addition, studies examining the contributions of these specific genes and their polymorphism and regular exercise on the growth trend of children are still insufficient. Therefore, this study analyzed the differences in aerobic and anaerobic exercise ability and growth-related indicators depending on the polymorphism of the ACE and the ACTN3 genes and to understand the genetic influence of exercise performance on the growth process of children.
Go to : 
METHODS
Subjects
The subjects of the study were 856 elementary school students (10.32±0.07 years) including 126 athletes (male: n=98, female: n=28) and 730 non-athletes (male: n=524, female: n=206) based upon 6 months athletic career. Questionnaires were used to select participants and those with physical disabilities or diseases were not included in the study. Informed consent for participation was sought from the parents of the participants. The study protocol was in compliance with the Code of Ethics of the World Medical Association (Declaration of Helsinki), and had previously been approved by the Institutional Review Board of the Keimyung University (IRB NO 11-233).
Analysis of the physique and blood parameters
The height and the weight were measured and the body mass index (BMI) was calculated using the formula, 'body weight/height2 (kg/m2)'. The subjects who fasted for more than 12 hours, are rested for 30 minutes then 10ml of the blood was drawn from the antecubital vein. The concentration of IGF-1 in the serum was measured by ELISA kit (Diagnostics Systems Laboratories, USA), and the growth hormone was measured by Radio Immuno Assay method using the GH measurement kit (RIA kit, LINCO Research, INC, USA).
The genotypes of ACE and ACTN3
Plasma obtained from EDTA tubes was used to obtain genomic DNA from the monocytes by the phenol-chloroform extraction method. Primers (Bionix INC, Seoul, Korea) were used to amplify the ACE genes. The sense primer was 5'-CTGGAGACCACT CCCATCCTTTCT-3' and the antisense primer was 5'-ATGTGGCCA TCACATTCGTCAGAT-3'. The polymerase chain reaction was performed as below using the PC320 (ASTEC, Japan). PCR product was confirmed by electrophoresis. A band was observed at 490 bp for type II, 2 bands were observed at 190 bp and 490 bp for the ID type and a band was observed at 190 bp for the DD type. All the samples of the DD type were PCR again to prevent the error that the DD type may be included in the ID type. For the 2nd PCR, sense primer 5'-TGGGACCACA GCGCCC GCCACTAC-3' and the antisense primer 5'-TCG CCAGCCCTCCCATGCCCATAA-3' were synthesized. The PCR product was electrophoresed. A band was observed at 310 bp for the ID type. The ACTN3 gene was also analyzed by PCR. The sense primer was 5'-CTGGAGACCACTCCC ATCCTTTCT-3' and the antisense primer was 5'-ATGTGGC CATCACATTCGTCAGAT-3'. The XX type showed bands at 108 bp, 97 bp and 86 bp, the RX type showed 4 bands at 205 bp, 108 bp, 97 bp and 86 bp and the RR type showed 2 bands at 205 bp and 86 bp.
Physical fitness
Grip, back strength and leg strength were measured with the muscular strength gauge (TTK, Japan). Sit-up were used as a measurement for muscular endurance, sit & reach for flexibility, side step test and response to light and sound using the reaction time gauge (TTK, Japan) for agility, and physical efficiency index from the Harvard step test for cardiovascular endurance. Power was measured by the vertical jump, long jump, medicine ball throw with under or over, 30 m sprint test and 100 m dash.
Bone growth
The non-dominant hand (mainly left hand) was used for X-ray measurement of bone age. The chronological age is calculated by subtracting the date of taking the X-ray from the date of birth. Bone age is calculated from the X-ray picture taken by the TW2-RUS method. A total of 20 bones were analyzed. The time for completing the bone maturity is when the total bone score reaches 1000. The early bone age is the value extracting the chronological age from the bone age.
Statistical analysis
The anthropometric and biochemical features are presented as mean and SEM. To determine the differences in continuous variables among the three genotype groups ANOVA was employed and a follow up analysis using contrast test was used when the distribution of the variable or of the logarithmically transformed variable approached a normal distribution and the variances of the variables were equal in the groups compared. Otherwise the Mann-Whitney U test was used. Bonferoni's test was utilized to determine differences in continuous variables between ACE II+ID and DD or ACTN3 RR+RX and XX with gene allele's types. Using Bonferoni's test, the combined effect of ACE I/D and ACTN3 R577X polymorphisms on the study phenotypes was analyzed by using four genotype combinations, i.e. ACE DD and ACTN3 RR+RX (which, at least hypothetically, might be more suitable for power/hypertrophy-oriented exercise tasks), ACE II+ID and ACTN3 XX group, ACE II+ID and ACTN3 RX group, and ACE DD and ACTN3 XX group [17,18]. The significance of deviations of observed genotype frequencies from those predicted by the Hardy- Weinberg equation were evaluated with X2 tests between athletes and non-athletes groups. A binary logistic regression model was used to test for the association of ACE I/D or ACTN3 R577X genotypes and early bone age, controlling for the risk factors of athletic career and gender by calculating the odds ratios (95% confidence interval) and corresponding p values. The level of significance was set at p<0.05.
Go to :
RESULTS
The genotype distribution of the ACE I/D polymorphism for all the subject shows 36.8%, 49.6% and 13.6% for the II, ID and DD types, respectively and the D allele frequency is 0.384, meeting the Hardy-Weinberg equilibrium. In addition, the athlete group and the non-athlete group reveal almost the same distribution (χ2=2.058, p=0.357). Also the distinction between the male (χ2=0.878, p=0.645) and the female (χ2=2.571, p=0.277) students exhibit almost the same distribution (Table 1). On the other hand, the genotype distribution of the ACTN3 R577X polymorphism for all the subjects indicate that the RR, RX and XX type are 30.7%, 48.6% and 20.7%, respectively and the X allele frequency is 0.450, which also meets the Hardy-Weinberg equilibrium. In addition, the athlete group and the non-athlete group show almost the same distribution (χ2=0.001, p=0.951). The distinction between the male (χ2=0.081, p=0.960) and the female (χ2=0.059, p=0.971) students display almost the same distribution (Table 2).
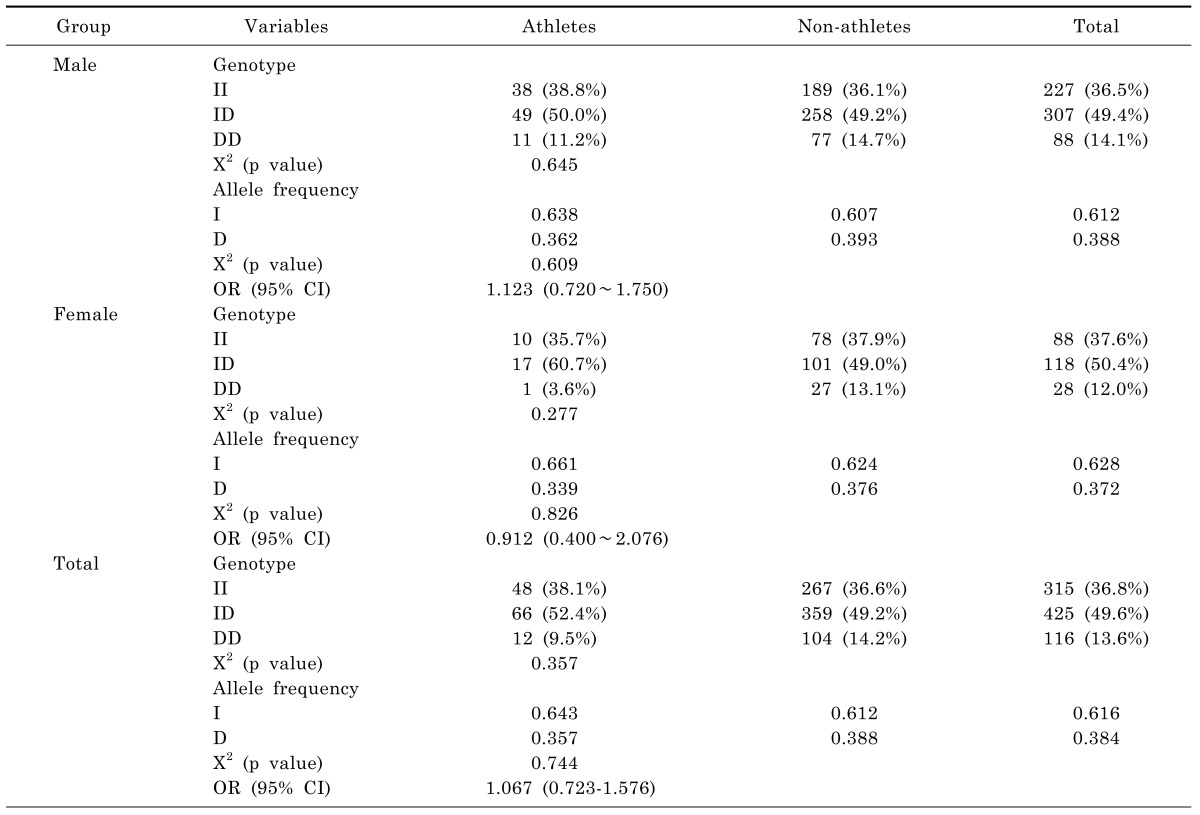
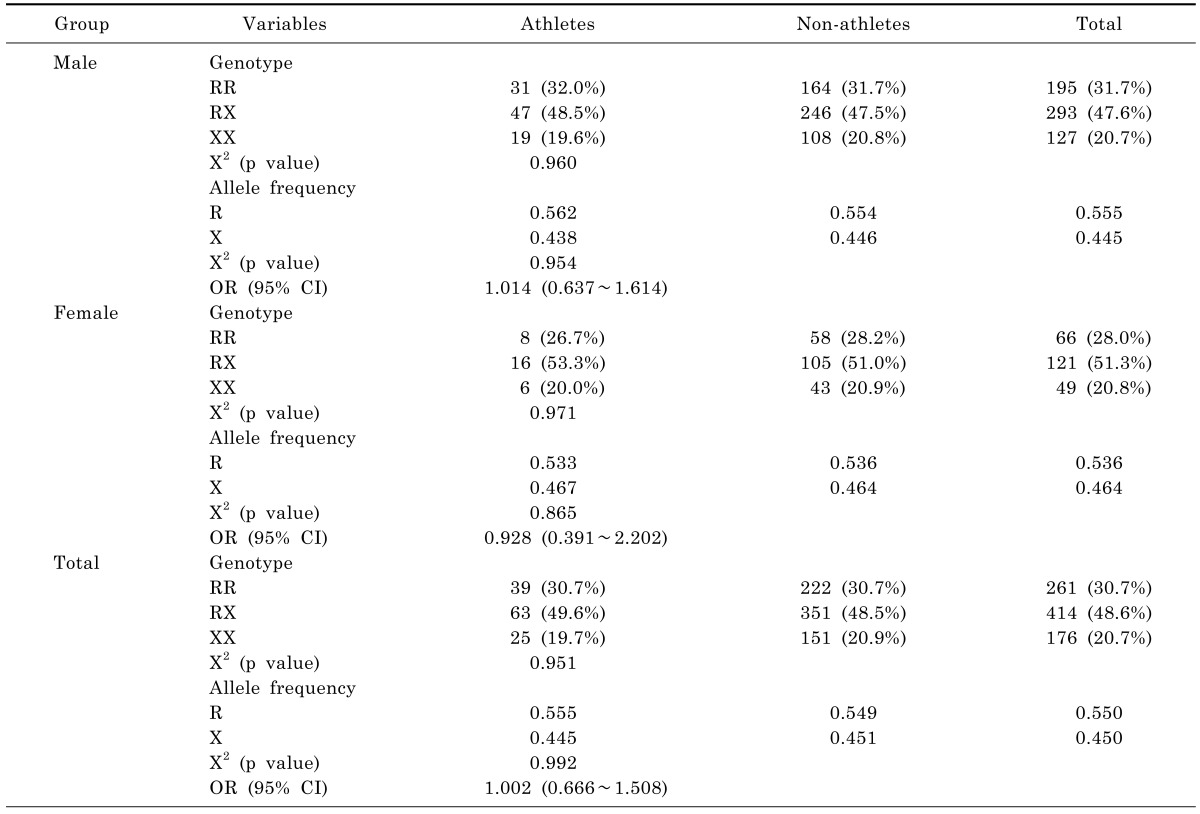
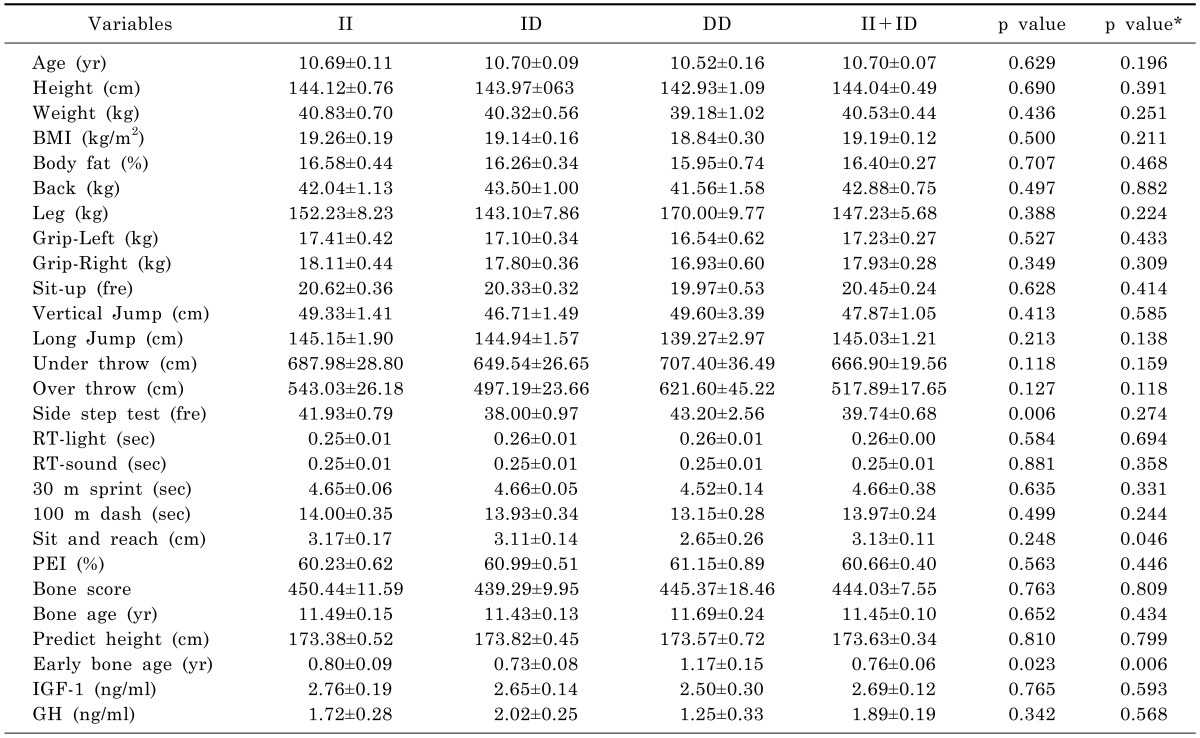
Table 3 shows the comparison of the anthropometric parameters, physical fitness and growth factors depending on the genotype of the ACE gene I/D polymorphism for all the subjects. Most of these items do not demonstrate significant differences in the genotype except the side step test which shows that the DD type is the highest (p<0.05) and the early bone age shows that the DD type is significantly higher than the II+ID type (p<0.05).
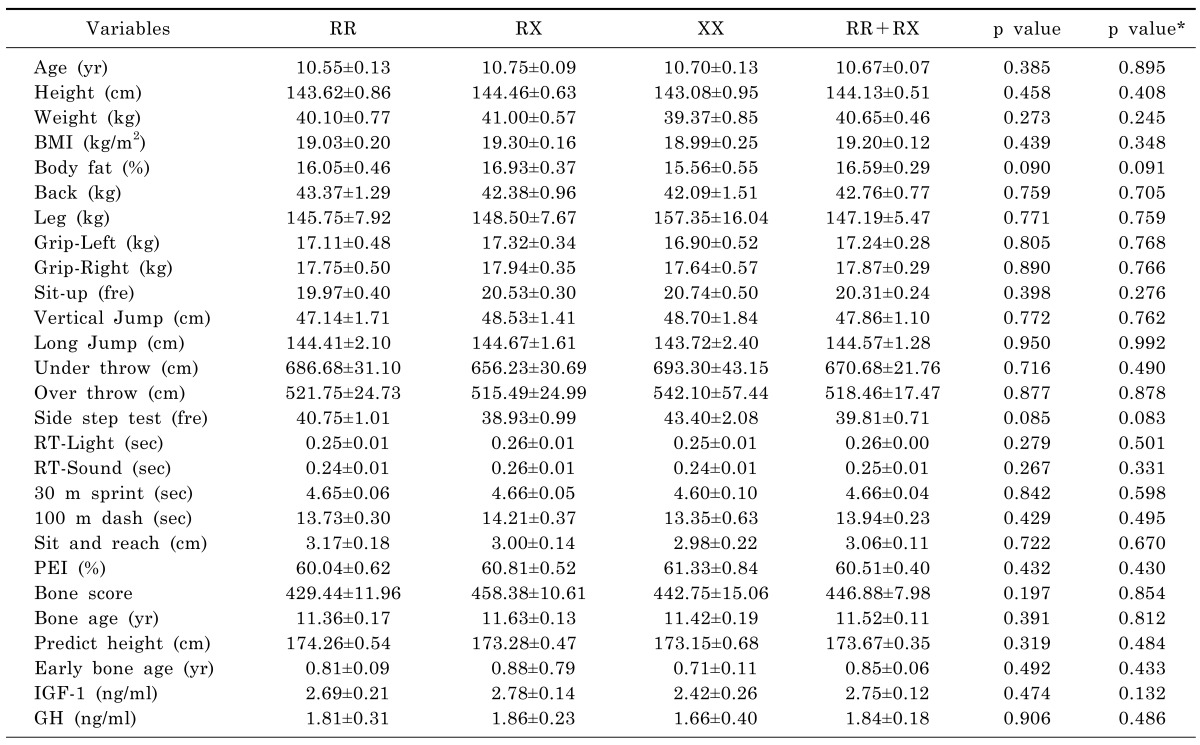
As shown in Table 4, the comparison of the anthropometric parameters, physical fitness and growth factors depending on the ACTN3 gene R577X polymorphism shows no significant difference for all the items in the genotype, and there is no significant difference between the II+ID type and the DD type.
As shown in Table 5, there is no significant difference for all the items except early bone age among the 4 groups (the ACE gene II+ID and the ACTN3 gene XX type group, the ACTN3 gene RR+RX and the ACE gene DD type group, the ACE II+ID and the ACTN3 RX type group, and the ACE DD and ACTN3 XX type group) to analyze the complex impact of the polymorphism in the ACE gene I/D and the ACTN3 gene R577X. However, the group which combines the ACE gene II+ID and the ACTN3 gene XX type shows consistent higher tendency than the group with the ACTN3 gene RR+RX and the ACE gene DD type in the aspect of all the items related to physical fitness, and it shows that the group with the ACTN3 gene RR+RX and the ACE gene DD type is significantly higher than the group with the ACE gene II+ID and the ACTN3 gene XX type for the early bone age (p<0.05) (Fig. 1).
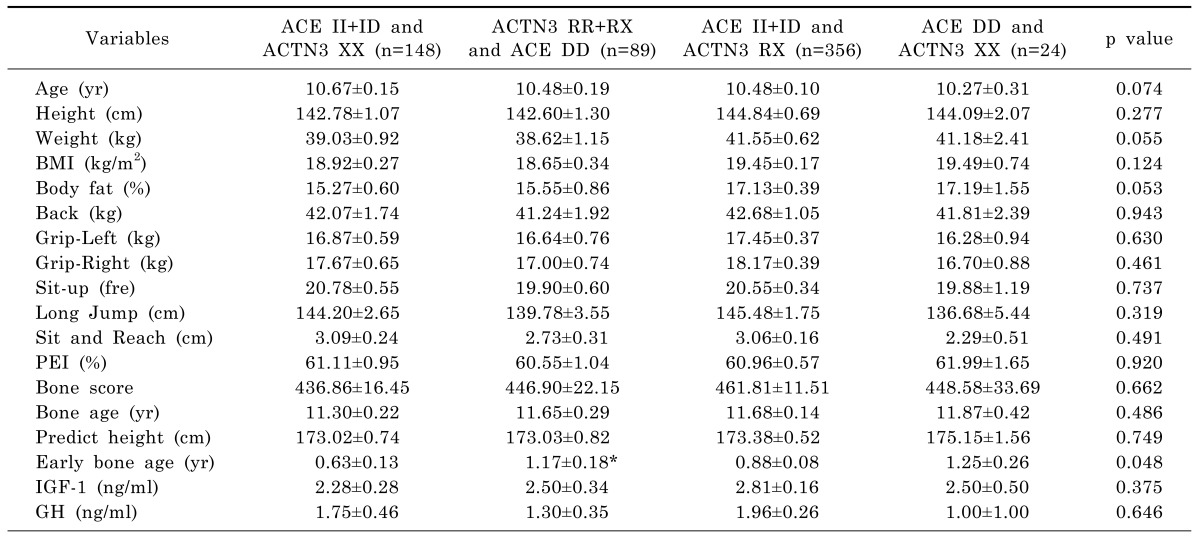
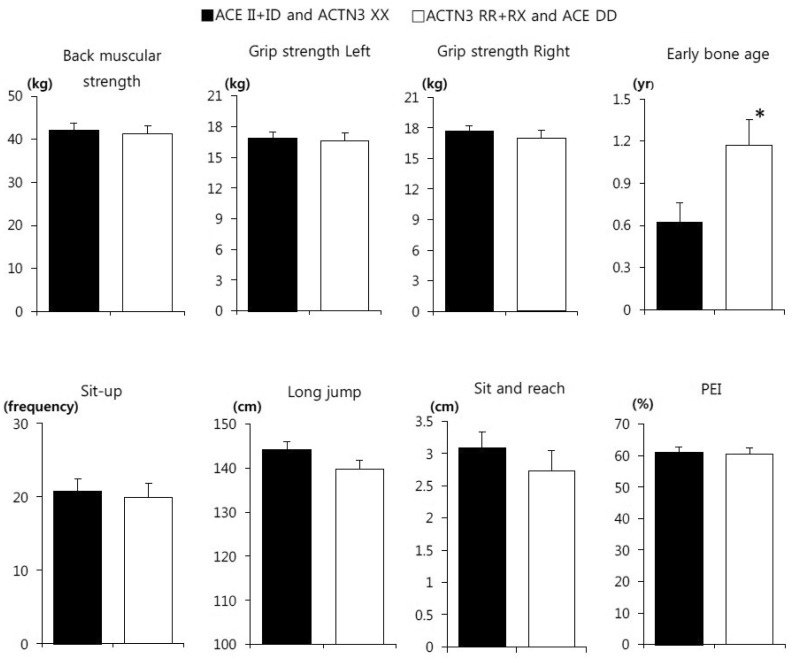 | Fig. 1Comparison of physical fitness and bone growth factors between the ACE II+ID and ACTN3 XX and ACE DD and ACTN3 RR+RX groups. PEI, physical efficiency index of Harvard step test. *p<0.05 Compared to ACE II+D and ACTN3 XX genotypes.
|
Table 5
Comparison of anthropometric parameters, physical fitness, and bone growth factors among the 4 groups
Values are mean and SE. Back/Leg/Grip-Left/Grip-Right, muscular strength; RT, reaction time; PEI, physical efficiency index of Harvard step test; IGF-1, insulin-like growth factor-1; GH, growth hormone.
p value: One-way ANOVA among 4 groups, *Significant different as compared to ACE II+ID and ACTN3 XX group with Bonferoni's test.
![]()
A logistic regression analysis with early bone age as the dependent variable and ACE I/D genotypes, ACTN3 R577X genotypes, gender, and athletic career showed no association of the ACTN3 R577X genotypes and gender with early bone age (Table 6). However, athletic career (OR=2.139, p=0.002) or ACE DD type (OR=1.938, p=0.019) conferred an approximately twofold increased effect for early bone age (Table 6).

Go to :
DISCUSSION
The frequency of D allele of ACE I/D gene was 0.384, and the percentage of DD genotype subjects was 13.6%, which was similar to Korean adults [19] and other Asian population [20,21]. We could confirm the lower prevalence of ACE DD genotype and frequency of D allele of ACE I/D gene in Asian populations as compared with American or European [20,21,22,23]. Pitsiladis et al. [24] suggested the typical allele frequencies for the I and D alleles of the ACE I/D polymorphism in a European population are 43% and 57%, respectively.
As the stop codon variant is quite common in human ACTN3 gene, XX homozygotes are in an estimated 1 billion people in the world [25]. The frequency of α-acinin-3-deficient genotype (577XX) varies from 25% in Asian population to <1% in an African Bantu population; the frequency in Europeans is ~18%. This raises the possibility that ACTN3 genotype confers differential fitness in humans, under certain environmental conditions [13]. Extremely low 577XX genotype frequencies were observed in Kenyan and Nigerian athletes versus controls (1% vs 1% and 0% vs 0%, respectively), and theirs were much lower than in any other non-African populations, where frequency of the 577XX genotype is 18% in Australian Caucasians, 10% in Aboriginal Australians, 18% in Spanish Caucasians and 25% in Japanese [24]. As the frequency of 577XX was 20.7% in this study, we could confirm the higher prevalence of 577XX genotype in Asian populations.
The ACE I/D genotype shows different influence due to a number of reasons including racial features, age groups and exercise status, meaning, it is difficult to draw a consistent conclusion on the polymorphism of a single gene. The ACE gene is a representing candidate which affects the endurance exercise ability and it is considered that the I allele and the D allele affect endurance and anaerobic power [26,27]. The occurrence frequency in the I allele showed a high relationship to endurance as seen in British mountaineers [28], South African triathletes [29], British distance runners [30], and Australian rowers [7]. It is reported that the occurrence frequency in the D opponent had high relation to power in short-distance swimming [27], sprinting [30], Poland's power-based sports [15]. Similar findings were reported in non-athletic populations [31,32,33]. However, Ash et al. [34] found no significant differences in ACE I/D polymorphism's distribution in Ethiopian distance runners. Other studies suggested a positive relationship in endurance capacity with DD type in young Chinese adults [35], Israel's endurance runners [36], and Korean athletic runners [37]. In addition, Scott et al. [8] found that ACE genotype was not a key determinant of the success of the world's top sprinters from Jamaica and the United States. The study may not confirm the impact of the ACE I/D genotype on muscular strength, throwing, jumping and sprint, general parameters of measuring the muscular functions and the power. In addition, the PEI, an item related to the cardiopulmonary function, did not show a significant difference depending on the ACE I/D genotype. However, the side step test, an agility item, showed that the DD type is significantly excellent, confirming the positive impact of the DD type on the speed. This means that the ACE I/D genotype may partially affect the agility of the Korean teenagers but the study may not confirm the significant difference between the physique and the physical fitness in the ACE I/D genotype. Therefore, the relationships between ACE I/D genotypes and physical characteristics or fitness remain ambiguous. It was also found out that the physique, physical fitness and growth indicators did not show significant differences in the R577X polymorphism of ACTN3 gene. The variant of stop codon 577 of ACTN3 is quite common in humans, with an estimated 1 billion people worldwide being XX homozygotes [25]. Gomez-Gallego et al. [17] reported that the ACTN3 577RR/RX genotypes highly appeared around the maximal power and the ventilatory threshold level, and Ahmetov et al. [38] claimed that the opponent frequency of the ACTN3 577X was low for endurance Russian athletes and related to the performance of rowing athletes. However, the data for the role of the ACTN3 in training response to cardiorespiratory fitness traits were insufficient, while the definitive impacts on the skeletal muscles were not entirely [39,40]. Norman et al. [41] even argued that it was not an important factor in muscle power or sprint performance. In particular, the hypothesis that α-actinin-3 deficiency may positively affect endurance was not be supported by prior studies [42,43,44,45]. It is reported that it is rarely related to the maximal oxygen uptake in Spanish or Russian endurance athletes [42,46]. This study on Korean children showed that the ACTN3 R577X genotypes are rarely related to physical fitness levels.
Even though significant features in physical fitness were not found due to individual gene polymorphism, Bouchard [1] proposed that the compounding impact of genes on training was related to the changes in the maximum oxygen intake which can be accurately investigated by the analysis of the complicated genes. However, scarce data are available on the combined influence of ACE I/D and ACTN3 R577X polymorphisms on fitness phenotypes. Rodrigez-Romeo et al. [47] found no differences of peak power output between those cyclists with the ACE DD and ACTN3 RR+ RX and ACE II+ID and ACTN3 XX genotype combinations. Eynon et al. [48] reported an association between the combination of both ACE and ACTN3 polymorphisms and elite sprint athletic status. This is different from the earlier finding for it proposed that the combination for a sprinter was the ACTN3 R allele+the ACE I allele. Bustamante-Ara et al. [49] reported no association (individually or combined) between power muscle phenotypes and ACE I/D plus ACTN3 R577X genotype combinations in non-athletic elderly populations. The study investigated the compounding impact of the ACE gene and the ACTN3 gene for all parameters related to physical fitness and found no significant difference as well, indicating insufficient results to explain the individual genetic variability. However, as shown in Fig. 1, the group where the ACE gene II+ID and the ACTN3 gene XX type were combined shows consistent higher tendency in all the physical fitness parameters than those of the group with ACTN3 gene RR+RX and the ACE gene DD types, indicating a possibility that the I and D alleles of the ACE gene are determinants of endurance and power, respectively, and that the R and the X alleles of the ACTN3 gene are prominent in power and endurance, respectively. It is possible that proper combinations of the 2 genetic opponents may be prominent to specific physical fitness parameters. However, young children may develop overall physical fitness in the early stage if the I allele of the ACE gene and the X allele of the ACTN3 are combined. It is suggested that the combined influence of ACE I/D and ACTN3 R577X polymorphisms on fitness phenotypes may affect others depending on the degree of experience in the exercise and on age wherein the ACTN3 X allele+the ACE I allele may positively affect the overall improvement in the physical fitness before the peculiarity in exercise ability emerges. The relationship between growth pace and genetic polymorphism in young children showed that early bone age was affected by the ACE DD type and exercise experience with the group combining the ACTN3 gene RR+RX and ACE gene DD types being significantly higher than the group with the ACE gene II+ID and ACTN3 gene XX types (p<0.05).
Claims that regular exercise may positively stimulate growth in young may not be always true because of compounding variables [26]. Family and twin studies have estimated that up to 60~80% of the variance in peak bone mass is attributable to genetic factors [50]. Regular exercise induces several beneficial changes in organs and biological pathways that lead to better physical performance and improved health outcomes. It is not clear, however, how exercise affects growth, which may depend on gender as well as specific features of the bones including the skeletal parts and the bone density [51]. It is evident that there are marked individual differences in physiological changes brought about by regular physical activity. It may be advantageous to have early morphological traits that favor performance in these competitive activities or a genotype that drives a slower rate of sexual maturation. In contrast, boys who excel in competitive sports tend to exhibit advanced skeletal and sexual maturity [52]. The exercise experience and the DD type of the ACE gene affect the early maturity of bones but how such growth stimulation affects the physique development warrants confirmation. We should consider that genes influence phenotypes varies in response to gender and athletic career. We performed an analysis based on the ossification process of the hand because of the possibility that early ossification may negatively affect growth [53]. The significant impact of the ACE DD type on early bone age may be considered as a related anabolic factor for the ACE DD type in the genetic aspect of the growth. However, additional confirmation is required because the growth hormone and the blood concentration of the IGF-1 show no significant difference between both individual and complex analyses of the ACE and ACTN3 gene polymorphism.
In conclusion, exercise and the DD type of the ACE gene may affect the early maturity of bones. Further research is needed to confirm these relationships.
Go to :
 XML Download
XML Download