

 PDF
PDF ePub
ePub Citation
Citation Print
Print


ABBREVIATIONS
5-HT
5-hydroxytryptamine
ACTH
adrenocorticotropic hormone
ALD
aldosterone
AngII
angiotensin II
CORT
corticosterone
CRH
corticotropin-releasing hormone
DA
dopamine
E
epinephrine
ET
endothelin
Hcy
homocysteine
HFD
high fat diet
HPAA
hypothalamus-hypophysis-adrenal cortex axis
HPLC
high-performance liquid chromatography
HPTA
hypothalamus-hypophysis-thyroid gland axis
IFN-γ
interferon-γ
IL
immune factors
LDL-c
low density lipoprotein cholesterol
NE
norepinephrine
NEI
neuro-endocrine-immune
NO
nitric oxide
PCA
principal component analysis
PRA
plasma renin activity
RAAS
renin-angiotensin-aldosterone system
SAM
sympathesis-adrenal-medulla axis
sICAM-1
soluble intercellular adhesion molecule-1
Sim
simvastatin
T3 or T4
thyroid hormone
TC
total cholesterol
TG
triglyceride
TNF-α
tumor necrosis factor-α
TRH
thyrotropin-releasing hormone
TSH
thyrotropic-stimulating hormone
vWF
von Willebrand factor
INTRODUCTION
The neuro-endocrine-immune (NEI) network, first proposed by Besedovsky in 1977 [1], plays a pivotal role in regulating homeostasis and optimizing health and makes great contributions to various complex diseases. Endothelial dysfunction of either the coronary-, the peripheral- or the cerebral vasculature is a predictor of vascular events and appears to be a marker of atherosclerotic risk. As the largest endocrine organ of the body, the endodermis can receive signals of neurotransmitters, hormones and cytokines [2], and can this way be controlled by the NEI network. This fact suggested that NEI network may be a potentially ideal index for the evaluation of endothelial dysfunction.
A variety of cardiovascular risk factors have been shown to induce vascular endothelial dysfunction, including smoking [3], hyperlipidemia [4], hypertension [5], hypoxia [6] and high levels of homocysteine (Hcy). Hyperlipidemia and hyperhomocysteinemia are closely associated with diet, and are currently occurring more often with the popularity of fast food. This problem has been attained global scale. Therefore, in this study high fat diet (HFD) and high methionine diet were used to induce endothelial dysfunction model in rats.
Statins are powerful lipid-lowering drugs, widely used in patients with hyperlipidemia and coronary artery disease. It was found that statins appear to have a pleiotropic effect beyond their lipid-lowering ability. They can also exert anti-inflammatory, anti-thrombotic and anti-oxidant effects, increase NO production and improve endothelial function [7]. Here, an interesting question is proposed that whether statins can also improve the expression of NEI network.
The objective of the present study was to determine the correlation between endothelial function and NEI network under different endothelial dysfunction models caused by HFD, Hcy and Hcy+HFD. The effect of simvastatin (Sim) on NEI network profile was also evaluated in the models of endothelial dysfunction.
METHODS
Animals and experimental groups
The experiment was approved by the Institutional Animal Care and Use Committee of Shanghai University of Chinese Medicine. Fifty male Wistar rats (Shanghai Lab. Animal Research Center, China) weighing 200~250 g were randomly divided into five groups fed on either ordinary diet (control group), high fat diet (HFD group; every 100 g ordinary diet was supplemented with 15 g of palm oil, 5 g of dried whole milk, 3 g of cholesterol and 0.5 g of sodium cholate), high Hcy diet (Hcy group; ordinary diet containing 3% methionine), high Hcy and high fat diet (Hcy+HFD group), or high Hcy and high fat diet combined with simvastatin (Hcy+HFD+Sim group; simvastatin was administered via gavage with a dose of 5 mg/kg per day, simvastatin was provided by Hangzhou MSD Pharmaceutical Co. Ltd). The animals were housed in an environmentally controlled room (temperature 20~25℃; humidity 45%~65%) for 12 weeks. Throughout the study, the animals were allowed free access to food and tap water.
Sample preparation and measurement
To evaluate endothelial function, some indices such as endothelin (ET), nitric monoxide (NO), von Willebrand factor (vWF) [8] and soluble intercellular adhesion molecule-1 (sICAM-1) [9,10] were determined. In addition, nineteen indices were measured to reflect the profile of NEI network, they are:
Hypothalamus-hypophysis-adrenal cortex axis (HPAA)
corticotropin releasing hormone (CRH), adrenocorticotropic hormone (ACTH), corticosterone (CORT);
Hypothalamus-hypophysis-thyroid gland axis (HPTA)
Thyrotropin releasing hormone (TRH), thyrotropic stimulating hormone (TSH), thyroid hormone (T3,T4);
Renin-angiotensin-aldosterone system (RAAS)
plasma renin activity (PRA), angiotensin II (AngII), aldosterone (ALD);
Immune factors
Interleukin (IL)-1β, IL-2, IL-6, interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α).
At the end of the experiment, blood samples were collected from the carotid artery after the rats were anesthetized (30 mg/kg butaylone intraperitoneally). Each blood sample was divided into three aliquots. The first aliquot (1 ml) was mixed with 30µL of 10% EDTA and 40µL of aprotinin. Samples were centrifuged at 3000 rpm for 5 min at 4℃. Radio-immunoassays were performed to measure the levels of ET, CRH, ALD and ACTH (test kits were provided by Purevalley Biotech, China). The second aliquot of serum (0.5 ml) put into an anticoagulant tube with 10% EDTA-Na2 and enzyme inhibitor, and was kept on ice. After mixing the serum was centrifuged at 3000 rpm for 5 min. at 4℃. Radio-immunoassays were used to measure the levels AngII of and PRA (test kits were provided by Beijin North Institute of Biological Technology, China), the total Hcy were determined using high-performance liquid chromatography (HPLC) [11]. A third aliquot of serum (3 ml) was used for ELISA detection of vWF, sICAM-1, NE, E and TRH. The levels of TSH, T3, T4, CORT, IL-1β, IL-2, IL-6, IFN-γ and TNF-α were measured by radio-immunoassays (test kits were provided by Beijin North Institute of Biological Technology). Serum NO concentration was measured by the method of nitric acid reductase (test kits were provided by Nanjing Jiancheng Bioengineering Institute, China). The serum concentrations of triglyceride (TG), the total cholesterol (TC) and the low density lipoprotein cholesterol (LDL-C) were measured using an auto-biochemical analyzer (OLYMPUS AU-600).
After the blood sampling, the hypothalamus was resected immediately and the obtained tissue was snap-frozen in dry ice (-70℃) and stored until use for biochemical assessments. DA and 5-HT were assayed by electrochemical detection using HPLC [12].
Data Processing
SAS v9.1.3 software was used for data analysis. Results were presented as means±SD. The significance of differences between groups were analyzed by the Dunnett's t-test and the student's t-test. Statistical significance was set at p<0.05.
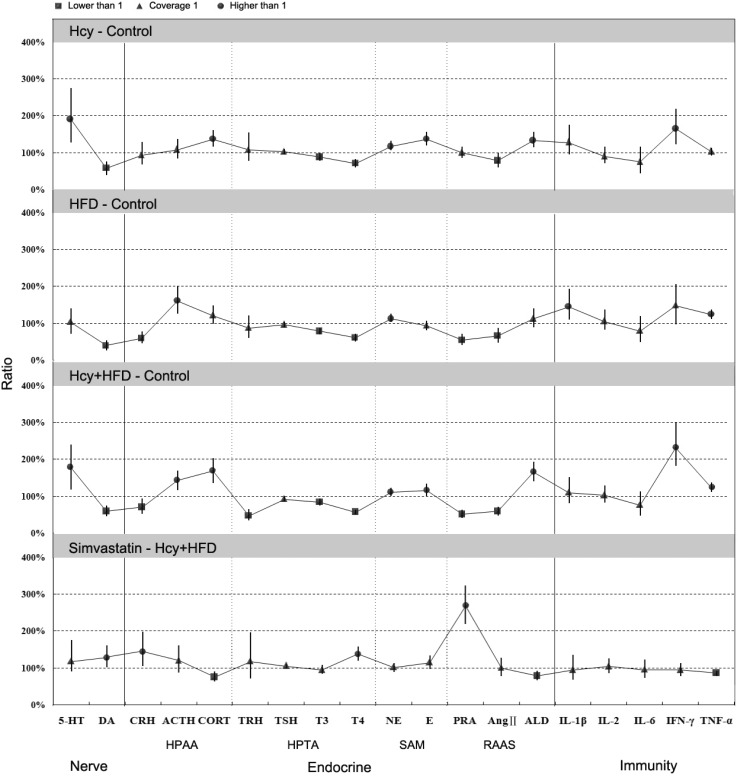
The bootstrapping method was repeated 1000 times to estimate the 95% confidence interval of the ratio of each NEI index between the groups. If 95% confidence interval of the ratio is lower or higher than 1, this indicates that the expression of the index in the test group is significantly lower or higher than that in the control group.
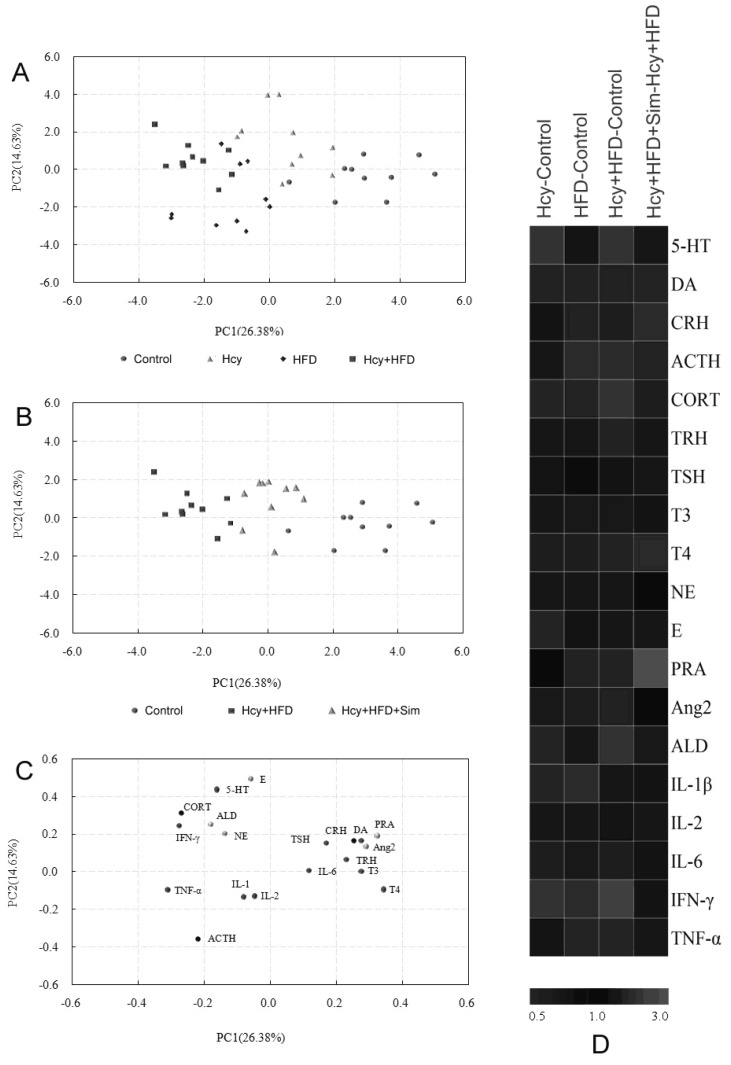
The NEI network data with 19 indices can be simplified by principal component analysis (PCA) [13,14], which can transform a large number of indices into only two or three latent variables known as principal components. Thus, the high dimension information can be visualized as a scatter plot, in which each data point represents one rat sample, and the distance between points in the score plot is an indication of the similarity between samples. In addition, loading plots from PCA were used to rank the importance of each variable to further capture the differentially expressed indices accountable for the separation between groups.
RESULTS
The levels of lipids and Hcy in each group
As shown in Table 1, the levels of TC, TG and LDL-C in the HFD and Hcy+HFD groups were significantly increased as compared with the control group. In addition, the Hcy level was significantly increased in the Hcy and the Hcy+HFD groups compared to those of the control group. These results indicated that the models were successfully established.
Vascular endothelial function
As shown in Table 2, vascular endothelial function was found to be impaired at different levels in the Hcy-, HFD- and Hcy+HFD groups. Hcy+HFD induced endothelial dysfunction was most serious. However, ET level was not significantly changed following HFD when compared with normal rats. In addition, simvastatin showed a protective effect on endothelial function.
NEI network profile
A number of marked changes in the NEI network were observed in rats following the different treatments. The bootstrapping method was used to estimate the 95% confidence interval of the ratio of the test group, relative to the control group (Fig. 1). In order to make the results better interpretable, principle component analyses (PCA) were employed for processing these complex data.
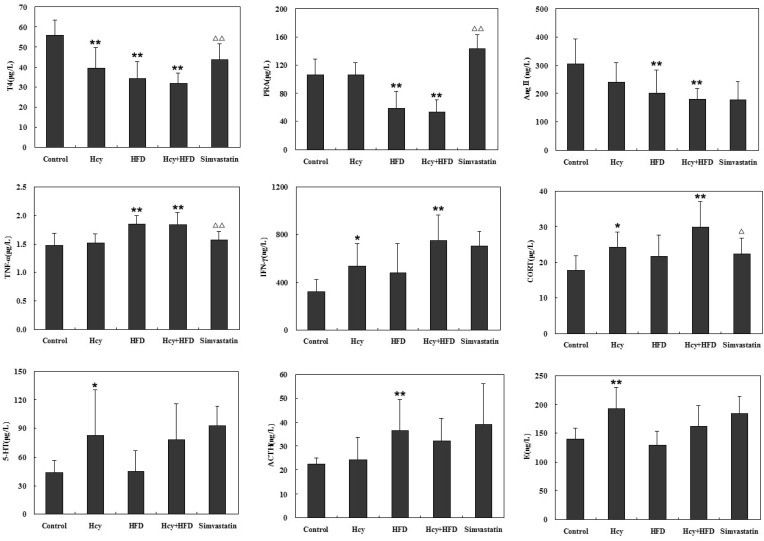
The PCA score plots showed an almost complete separation among the control and model groups (Fig. 2A), principal components 1 (PC1) and 2 (PC2) explained 26.38% and 14.63% of the total variance. The PCA loading plots (Fig. 2B) indicated the contribution of the 19 indices to the differences observed among the samples. Hcy+HFD treated animals were well separated from the normal animals along the first PC, and this mainly arose from the variation of T4, PRA, AngII, TNF-α, IFN-γ and CORT data. The results indicated that the PC1 mainly reflected the information of the RAAS and immune system. HFD treaded animals were separated from Hcy treated animals along the PC2, and this arose from the main variation of 5-HT, ACTH and E data. These key indices selected from PCA model showed significant differences between the control and the experimental groups (Fig. 3).
The PCA model calculated from the data of the control and model groups was then used to predict the scores of PCs in the Hcy+HFD+Sim group. As shown in Figure 2B, the expression of NEI network in the Hcy+HFD+Sim group obviously deviated from that in the Hcy+HFD group, and approached the state of the control group. The results suggested that simvastatin has an obvious regulatory effect on the NEI network.
DISCUSSION
Endothelial dysfunction is thought to be a key event in the development of atherosclerosis and has been reported to predate clinically obvious vascular pathology by many years. Previous literatures have demonstrated that exposure to homocysteine (Hcy) and high fat diet (HFD) can lead to vascular endothelial dysfunction, but the main differences between Hcy and HFD is still unclear. In this study, we compared two models of exposure to Hcy and HFD respectively, with the combined model of Hcy+HFD on vascular endothelial function. The results showed that the vascular endothelial function was affected in all three model groups, in which the No level was significantly decreased and the vWF and sICAM-1 levels were significantly increased. However, there were still some differences among the model groups. For example, the ET level was not obviously changed in the HFD group, and endothelial function was impacted most seriously in the Hcy+HFD group. In addition, endothelial function of the rats in the Hcy+HFD+Sim group showed a recovery tendency because the levels of ET, vWF and sICAM-1 were significantly lower and NO was significantly higher than in the Hcy+HFD group.
The interdisciplinary fields of neuroendocrine and immune systems have undergone explosive growth in recent years [15]. Increasing evidence has shown that the NEI network plays a pivotal role in regulating homeostasis and optimizing health and makes great contributions to various complex diseases [16]. In this study, we also observed the changes of the NEI network in the three models. The results suggested that Hcy mainly affected the balance of neurotransmitters, HPTA and SAM, while HFD mainly influenced the HPAA, HPTA and RAAS. The combination of Hcy and HFD impacted almost the whole NEI network and showed synergetic damaging effects. It is worth mentioning that, simvastatin reversed the imbalance of the NEI network disturbed by the Hcy+HFD, especially visible at the levels of DA, CRH, CORT, T4, PRA, ALD, IL-6 and TNF-α, suggesting that the regulatory role of simvastatin on endothelial function may be associated with the NEI network.
A growing number of reports have demonstrated the close relationship between endothelial function and NEI network: (1) Endothelial function in patients with severe chronic heart failure can be improved by DA [17], suggesting that neurotransmitters may play a key role in the pathogenesis of endothelial dysfunction; (2) AngII can lead to endothelial dysfunction via AngII receptor subtypek 1 activation and reactive oxygen- and nitrogen species generation [18]; (3) L-thyroxine therapy can improve endothelial function in the subclinical hypothyroidism patients [19]; (4) CRH can induce a significant increase of ET-1 release [20]; (5) Endothelial dysfunction occurring in the metabolic syndrome is the result of effects of the inflammatory cytokine TNF-α and subsequent production of superoxide [21,22]. The studies mentioned above indicated that NEI network has a tight connection with endothelial function.
Observing the profile of NEI network is a good method to distinguish disease states induced by different risk factors, this approach is similar to the Metabonomics [23], which used metabolic fingerprints to study the physiopathologic state. However, the potential biomarkers found by metabonomics may be surrogates of the metabolic process rather than direct reporters of disease target. Conversely, NEI network has tight connection with disease state, and the discriminating indices captured in the PCA loading plots may lead to therapeutic targets. For example, in this study, we found the levels of T4 in the three model groups were significantly lower than the control group, and these changes can be reserved by simvastatin. This result suggested that T4 may be the key index for vascular endothelial dysfunction. Clinical studies have shown that there is an association between subclinical hypothyroidism and coronary artery disease, and that after treatment with L-thyroxine the endothelial function in the subclinical hypothyroidism patients was improved [19,24]. This fact supported the idea that T4 plays a key role in endothelial function.
In addition, NEI network can also be used to evaluate drug effects. In this study, significant effects on the NEI network were observed in the simvastatin group. It is particularly suitable for the evaluation of Chinese medicine, which acts through complex mechanisms featured as multicompound, multitarget and multipathway. It has become more recognized that Chinese medicine produces the healing efficacy in a more holistic way. However, researchers typically only focus on a single or several indices associated with a disease. Obviously, NEI network is a better indicator for Chinese medicine to evaluate its holistic effect on the body.
In summary, the changes of NEI network were well observed in the three endothelial dysfunction model groups. The effect of simvastatin treatment in the NEI network was also studied. The results indicated that NEI network has a tight connection with endothelial function, and this relationship can be used to distinguish different risk factors and evaluate drug effects. It should be noted that, the mechanisms of endothelial dysfunction are now well recognized, therefore, these aspects are not the focus of the study.


 XML Download
XML Download