

 PDF
PDF ePub
ePub Citation
Citation Print
Print


ABBREVIATIONS
EP
early follicular phase
LP
late follicular phase
VO2max
volume of maximal oxygen uptake
HR
heart rate
SV
stroke volume
CO
cardiac output
TVC
total vascular conductance
SBP
systolic blood pressure
DBP
diastolic blood pressure
MAP
mean arterial blood pressure
SVi
SV index
BSA
body surface area
HPLC
high-performance liquid chromatography
INTRODUCTION
Several studies have shown that blood pressure fluctuates during the phases of the menstrual cycle and tends to be highest at the onset of menstruation (e.g., early follicular phase) [1-4]; Moreover, these peak values are associated with time reductions in peripheral vascular reactivity [1,5]. These observations raise the possibility that the blood pressure response to exercise may also fluctuate during the menstrual cycle. In this regard, administration of estrogen can attenuate contraction-induced increases in blood pressure in cats [6] and forearm vasoconstriction in postmenopausal women [7]; suggesting that reduced levels of estrogen during menstruation may lead to abnormal blood pressure responses to exercise.
These previous studies focused on effects of isometric exercise. Effects of dynamic exercise on healthy premenopausal women may be of interest because there are differences in the pattern of the cardiovascular response to the two modes of exercise. For example, at a given level of oxygen consumption, blood pressure increases more during static compared to dynamic exercise [8]. Also, differences in muscle mass, tension production and metabolism during dynamic and static contraction may lead to differential effects on the magnitude of the corresponding blood pressure responses [9,10]. Thus, an understanding of the extent to which low levels of estrogen affect the pressor response to dynamic exercise and the hemodynamic mechanisms responsible may be clinically important as this type of activity is performed in clinical exercise testing and cardiac rehabilitation programs and has been shown to lower both resting and exercise blood pressure in postmenopausal women [11].
Results of a small cohort of previous investigations have revealed no menstrual cycle-induced differences in blood pressure during dynamic exercise. However, differences in methodology may have had intervening effects on the results. They include selection of time points for exercise testing where estrogen concentrations were not different [12] or where menstrual cycle effects on resting blood pressure were not seen [13,14]. Based on the totality of these observations, we tested the hypotheses that, when resting blood pressure is greater in the early versus the late follicular phase of the menstrual cycle: 1) blood pressure during dynamic exercise is also greater and 2) this greater blood pressure is associated with augmented vasoconstriction.
METHODS
Study population
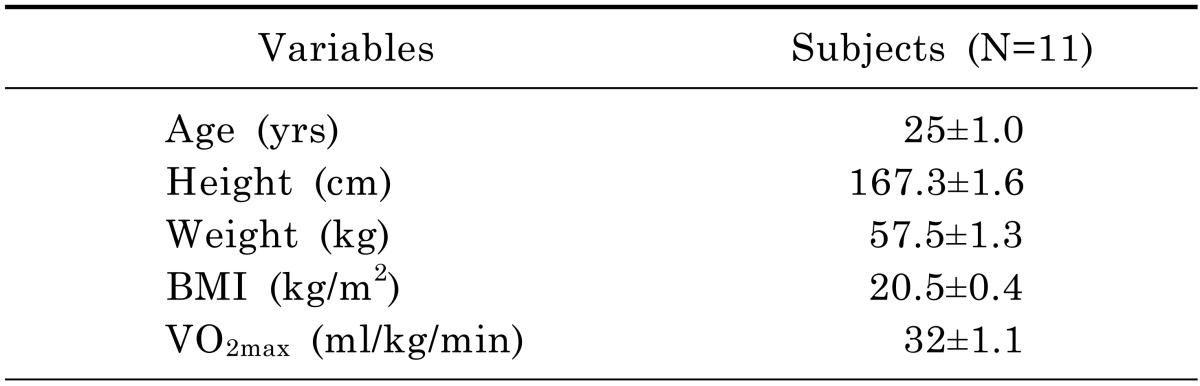
Data were collected from Kyung Hee University in Yongin, Korea. All procedures were reviewed and approved by the Kyung Hee University Institutional Review Board (KHU 2011-002). All subjects signed informed consent. We studied 11 healthy women (age 25±1 yr) during two phases of their ovarian cycle: days 1~4 (early follicular phase, EP) and days 10~12 (late follicular phase, LP) [15]. These time points were chosen because estrogen levels are near their lowest concentrations during days 1~4 and are near their maximal levels during days 10~12) [16]. Moreover, progesterone levels are low at both of these time points [16]. This was an important consideration, because progesterone can antagonize beneficial effects of estrogen on vascular reactivity [17].
All subjects were nonsmokers in good health who were not taking cardiovascular medications and had regular menstrual cycles as assessed by medical history. All subjects were sedentary. The order in which the cycle phase was studied was the late follicular phase followed by the early follicular phase.
Exercise protocols
Resting blood pressure was evaluated in a seated position. We obtained a minimum of 2 blood pressure measurements, which were taken 2 min apart using a sphygmomanometer. To determine the relative exercise intensities of the two workloads used in the study (40% and 60% of maximal oxygen uptake [VO2max]), a maximal exercise test was performed using a cycle ergometer (Manark 828, Sweden). All subjects cycled at 0 watts for 2 min followed by increases of 30 watts every min until they could no longer maintain a pedal cadence of 60 rpm. Respiratory gases were measured using an Ultima CPX Metabolic Measurement Cart (Medgraphic, USA). The VO2max obtained from this test was used as an index of functional capacity. All subjects, in turn, completed a progressive exercise test consisting of 5 min of cycling at each of the two work intensities (mild: 40% of VO2max and moderate: 60% of VO2max). This test was performed during both the early and late follicular phases of the ovarian cycle.
Measurement of hemodynamic variables
Stroke volume (SV) and HR were measured continuously via impedance cardiography (Physio Flow, Manatec Biomedical, France). This noninvasive device provides real-time CO data and measures hemodynamic parameters in healthy subjects [8,18,19]. In brief, SV was measured by the bioimpedance method based on changes in transthoracic impedance during the cardiac cycle [20]. One set of two electrodes (one transmitting and one sensing) was placed above the supraclavicular fossa at the base of the left side of the neck. A second set was placed at the xiphoid process. A third set was used for recording the ECG. CO was determined according to the following formula: CO=HR×SVi×BSA, where HR (heart rate) was measured from the R-R interval obtained from the first derivative of the ECG. SVi is the SV index (i.e., SV÷BSA). BSA (body surface area) (m2) was determined based on the Haycock formula: BSA=0.024265×BM0.5378×H0.3964, where BM is the body mass in kilograms and H is height in centimeters.
Brachial artery blood pressure was measured by a sphygmomanometer during mild and moderate exercise in steady-state conditions. Mean arterial blood pressure (MAP) was calculated using the formula: MAP=[(SBP-DBP)×1/3]+DBP. Total vascular conductance (TVC) was calculated as CO÷MAP. Blood pressure was measured by the same investigator in each subject for all interventions.
Measurement of catecholamine
To obtain blood samples for measurement of norepinephrine and epinephrine concentrations, a catheter with a 20-gauge needle was inserted into a brachial vein. Five ml of venous blood were obtained at rest and during the last min of each exercise workload. Samples were then centrifuged at 3,000 rpm for 10 min. Subsequently, plasma concentrations were isolated and stored at 5℃ until analysis.
Catecholamine concentrations were determined by reverse-phase high-performance liquid chromatography (HPLC). Extraction was performed by selective absorption from aluminum oxide (Plasma-Catecholamine-Kit, BIO-RAD, Korea). Samples were then added to a 200 µl internal standard solution+1 ml Tris Buffer. The solution was shaken for 12 min followed by centrifugation at 2,500 rpm for 5 min. Subsequently, the supernatant (minus the alumina) was aspirated using a vacuum aspirator. The samples were then centrifuged again at 2,500 rpm for 2 min. Subsequently, 200 µl of the supernatant was injected onto the HPLC column and eluted by mobile phase. The intra-assay coefficient of variation was 4.0% for norepinephrine and 4.0% for epinephrine.
Data analysis
Cardiac output measurements using impedance cardiography (i.e., averaging procedures in steady-state conditions) have been found to be reliable and valid in healthy subjects [8,18,19]. Accordingly, this technique accurately assesses the absolute values of CO at rest and during exercise. Effects of dynamic exercise on MAP, SBP, DBP, HR, SV, CO and TVC have been expressed as absolute values and as changes from baseline.
The average values of HR, SV, and CO at each 30 sec interval at rest and during mild and moderate exercise were used for comparison purposes. Blood pressure was assessed between the 4th and 5th min of each workload, just before collection of blood samples. Mean values of all variables were compared between EP and LP via the Student's paired t test. Means were considered to be statistically different at p<0.05.
RESULTS
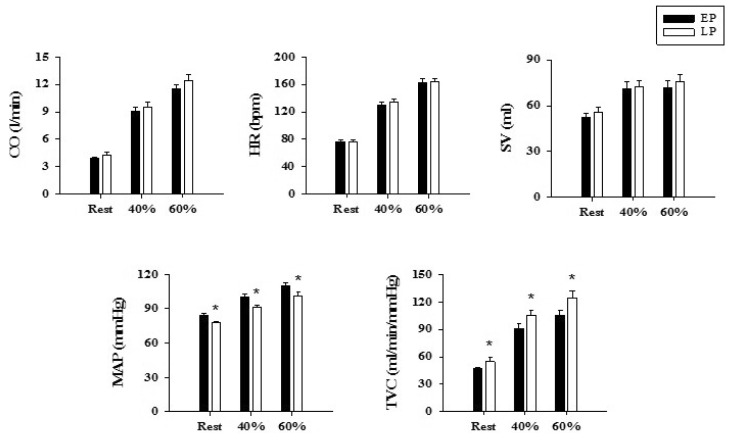
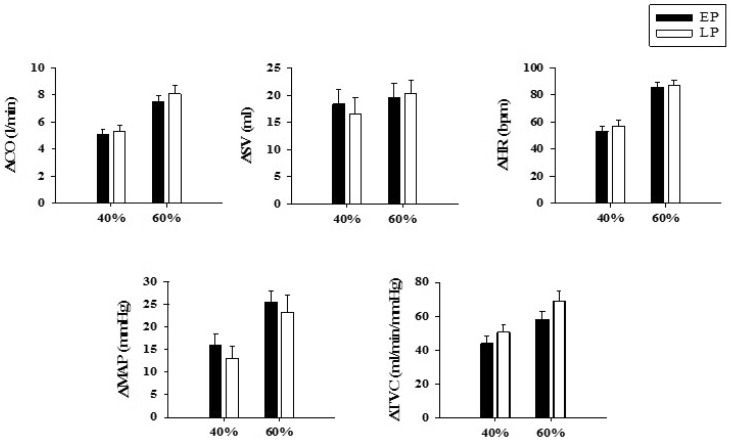
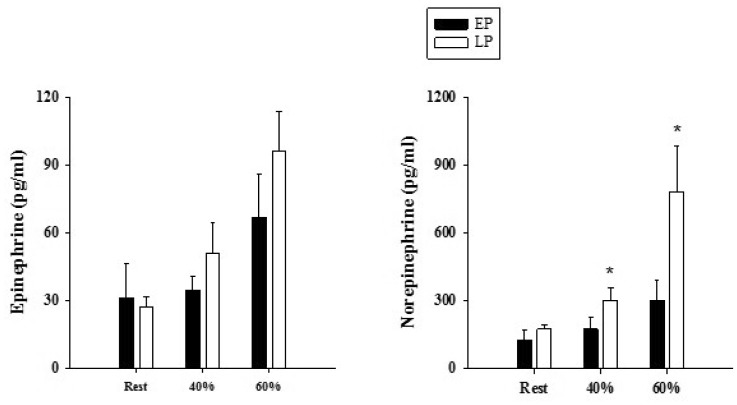
Subject characteristics are presented in Table 1, Fig. 1 depicts comparisons of the absolute values of the hemodynamic variables between the two menstrual phases at rest and during exercise. Resting SBP, DBP, and MAP were significantly higher in the early compared to the late follicular phase (p<0.05). TVC was also lower in the early follicular phase (p<0.05). Conversely, no statistically significant differences in resting HR, SV, or CO were found between these two phases. During exercise, absolute values of SBP and MAP were greater while those of TVC were lower during the early versus the late follicular phase of the menstrual cycle (p<0.05). This was the case for both exercise intensities (40% and 60% of VO2max). On the other hand, no differences between phases were found for DBP, HR, SV or CO during either work intensity. When the magnitude of the exercise-induced cardiovascular responses were compared (i.e., changes from rest to exercise) (Fig. 2), no differences between the two menstrual phases were found for any of the variables during either work load. Menstrual cycle phase had no effect on plasma concentrations of epinephrine at rest or during exercise (Fig. 3). Resting levels of norepinephrine also were not statistically different between the early and late follicular phases. However, 7 of the 9 subjects tested had higher levels during the late follicular phase, suggesting a trend for an increase in this catecholamine. During cycling exercise, norepinephrine values were higher during the late follicular phase in response to both cycling workloads (p<0.05) (Fig. 3). The magnitudes of the exercise-evoked increases in norepinephrine were also greater during the late follicular than the early follicular phases at both work intensities (40% VO2max: Δ175±49 vs. Δ48±9 pg/ml; 60% VO2max: Δ128±49 vs. Δ611±193 pg/ml) (p<0.05).
DISCUSSION
The most interesting new finding of this study is that absolute MAP during dynamic exercise in healthy premenopausal women is greater in the early compared to the late follicular phase of the menstrual cycle. The enhanced blood pressure during cycling in the early follicular phase was most likely due to an additive effect of a concomitant elevation in resting blood pressure because the magnitude of the changes in the exercise-induced pressor responses were not different between the early and late follicular phases during either workload.
TVC at rest and during dynamic exercise was also lower in the early follicular phase, suggesting that peripheral vasoconstriction contributed to the higher blood pressure response seen during this phase of the menstrual cycle. It is not immediately clear why these apparent changes in peripheral vasoconstriction occurred. There is evidence that reactivity of peripheral arteries and microvascular arterioles improves significantly during the late follicular phase and then returns to baseline levels in early follicular phase [1,5]. This effect appears to be mediated by estrogen-induced increases in NO bioavailability and vascular reactivity that are associated with concurrent reductions in blood pressure [1,21]. Consequently, reductions in endothelial function during the early follicular phase may explain, in part, the concomitant attenuation of TVC at rest and during exercise.
Our observations differ from results of Lewandowski et al. [12], who found no differences in the blood pressure in response to progressive treadmill exercise between the pre-ovulatory follicular, (i.e., 2 days before ovulation) and the luteal (i.e., 2~3 days before menstruation) phases. However, no differences in plasma estrogen concentrations were seen and progesterone levels were over 20 fold greater during the luteal phase.
Kim et al. [14] and Hartwich et al. [13] also reported no menstrual effects on blood pressure during cycling when the early (1~5 days) and late (10~15 days) follicular phases were compared. Unlike our study and others [1-4], they saw no menstrual cycle effects on resting blood pressure. It is not clear why effects on resting blood pressure were not seen, especially since measurements were taken at the same time points during the menstrual cycle as ours were. One possible explanation is that our subjects were sedentary and had a relative low functional capacity (i.e., low maximal O2 uptake [VO2max: 32±1 ml·kg-1·min-1]) whereas the two previous studies enrolled subjects that had a higher functional capacity (VO2max: 37±2 ml·kg-1·min-1) and/or engaged in physical activity 2~3 days a week [13,14]. This is of note because even moderate levels of chronic physical activity can improve vascular compliance [22,23]. Consequently, the differential effects of the menstrual cycle on vascular conductance, which we observed in our sedentary subjects, may have been minimized in the more active subjects in the Kim et al. [14] and Havlik et al. [22] studies. This outcome may have offset or reduced differences in resting blood pressure between the early and late follicular phases in these subjects compared to ours.
Menstrual cycle related changes in the sympathetic nervous system also may have contributed to the differences in blood pressure and conductance during exercise that we found in our subjects. Estrogen can reduce blood pressure, and there is evidence that this effect is related to decreases in sympathetic nerve activity [24]. Unexpectedly, we found that concentrations of plasma norepinephrine during exercise were higher during the late than the early follicular phases and that a trend for this phenomenon was also seen at rest (i.e. 7 out of 9 subjects testing displayed higher norepinephrine concentrations during the LP phase). This finding suggests that sympathetic nerve activity was also augmented during this phase. While these outcomes seem counterintuitive, higher resting sympathetic nerve activity and concentrations of norepinephrine have previously been reported during the luteal versus the early follicular phases, even though luteal estrogen concentrations were also higher [25]. Since estrogen enhances the basal release of the nitric oxide [26], parallel increases in sympathetic outflow may indicate opposition to vasodilation evoked by estrogen-induced increases in nitric oxide.
Understanding differential effects of the menstrual cycle on the blood pressure response to dynamic exercise and the hemodynamic mechanisms underlying these differences may be beneficial for maximizing the effectiveness and safety of exercise interventions in premenopausal women. In this regard, results of maximal exercise testing for diagnosis of cardiovascular disease or determination of functional capacity will likely be less reliable if the phase of the menstrual cycle is not held constant. Moreover, blood pressure may reach unsafe levels in premenopausal women with preexisting hypertension or heart failure that undergo exercise testing during the late luteal or early follicular phases of the menstrual cycle. Thus, understanding intervening effects of the menstrual cycle on dynamic exercise may lead to safer and more effective exercise interventions that avoid abnormal cardiovascular responses.
Results of this study indicate that menstrual cycle effects on resting blood pressure carry over to dynamic exercise. The fact that the magnitudes of the exercised-induced increase in blood pressure were not affected by the menstrual cycle suggests that elevated absolute blood pressure during the early follicular phase is an additive effect of concomitant elevations in resting blood pressure. Elevated resting and exercise blood pressure in the early follicular phase occurred in concert with lower levels of vascular conductance, which suggests that low levels of estrogen also lead to increased peripheral vasoconstriction. The mechanism responsible for the reduced TVC (i.e., enhanced vasoconstriction) may be due to decreases in endothelial function, vascular compliance and nitric oxide availability by low levels of estrogen [1,17,27].
 XML Download
XML Download