

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Constipation refers to bowel movements that are infrequent or difficult passage of stools due to colonic slow transit, and is a common cause of painful defecation and fecal impaction [1]. Causes of colonic slow transit include diet, hormones, side effects of medications, and heavy metal toxicity. Its incidence ranges from 2% to 30% in the general population [2,3], and females are more often affected than males [4]. Gender differences in hormone concentration could affect the gastrointestinal transit time. An association of constipation or slow colonic transit time with pregnancy [5-7] and menstrual cycle [8,9] has been reported. Progesterone has been the hormonal explication for many gastrointestinal symptoms that occur in pregnancy, including intestinal constipation [5], and is the main hormone of the luteal stage, compared with other phases of the menstrual cycle [10]. Some studies have reported an increase in constipation in females in the luteal phase of the menstrual cycle [9], however, others have suggested that it is not affected by the luteal phase [11], and the same in both genders of colonic transit time [12,13]. Estrogen is produced primarily by the ovaries, and during pregnancy. Estrogen levels vary throughout the menstrual cycle, with the levels highest occurring near the end of the follicular phase just before ovulation.
Therefore, this study was conducted in order to determine of whether the female sex steroid hormone itself is responsible for development of constipation in both female and male mice.
Go to : 
METHODS
Animal
Specific pathogen-free male and female ICR mice (~10 weeks old) were purchased from Samtako, Inc. (Osan, Korea). Three animals were housed in a cage and fed with tap water and mouse chow diet (Nestle Purina PetCare Korea, Ltd., Seoul, Korea) for five days.
Groups
Mice (n=9 for each group) were randomly divided into three groups for the experiment on the effect of female sex steroid hormones on constipation in male or female mice. The first group, as the normal control group, was fed the chow diet only, and the second and third groups received daily oral administration of estrogen (β-estradiol, Sigma, St. Louis) 0.4 mg/kg or progesterone (Progynova, Schering SA, France) 1 mg/kg of body weight in 20 µl of corn oil for five days.
Examination of intestinal movement
To test the effect of female sex steroid hormones on gastrointestinal function, the animals were fasted for one day and as much as 1 ml/100 g of body weight of 10% barium sulfate solution was administered directly into the stomach. After 30 min, mice were anesthetized with urethane and the moving distance of barium sulfate from the duodenal sphincter to the large intestine was measured.
Feces wet weight and dry weight
Feces were collected and weighed daily. Dry weight of feces was measured from four days drying in the oven at 80℃.
Statistical analysis of data
Values are expressed as mean±SE. A one-way analysis of variance (ANOVA) was used for multiple comparisons. When ANOVA showed significant differences, post-hoc analysis was performed using the Newman-Keuls multiple range test by SPSS.
Ethics statement
This study protocol was approved by the institutional and governmental regulations concerning the ethical use of animals were followed, and this research was approved by Animal Care and Use Committee of Yeungnam University.
Go to :
RESULTS
Body weight
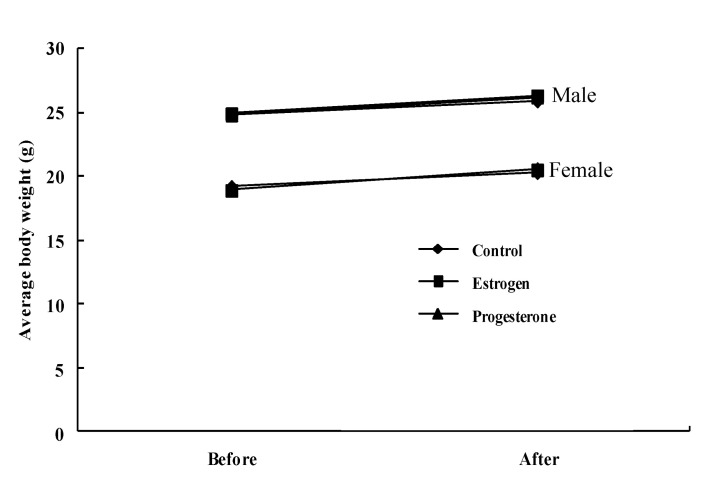
The body weight (g) of mice did not differ significantly among groups after sex steroid hormones administration for 5 days in both male (24.8±1.5, 24.9±1.6, and 24.8±1.6 of control, estrogen, and progesterone mice before hormone administration, respectively, and 25.9±1.7, 26.3±2.1, and 26.2±2.0, of control, estrogen, and progesterone mice after hormone administration, respectively) and female mice (19.2±1.3, 18.9±1.3, and 19.0±1.4 of control, estrogen, and progesterone mice before hormone administration, respectively, and 20.3±1.6, 20.5±1.7, and 20.6±1.7 of control, estrogen, and progesterone mice after hormone administration, respectively) (Fig. 1).
Wet weight of feces
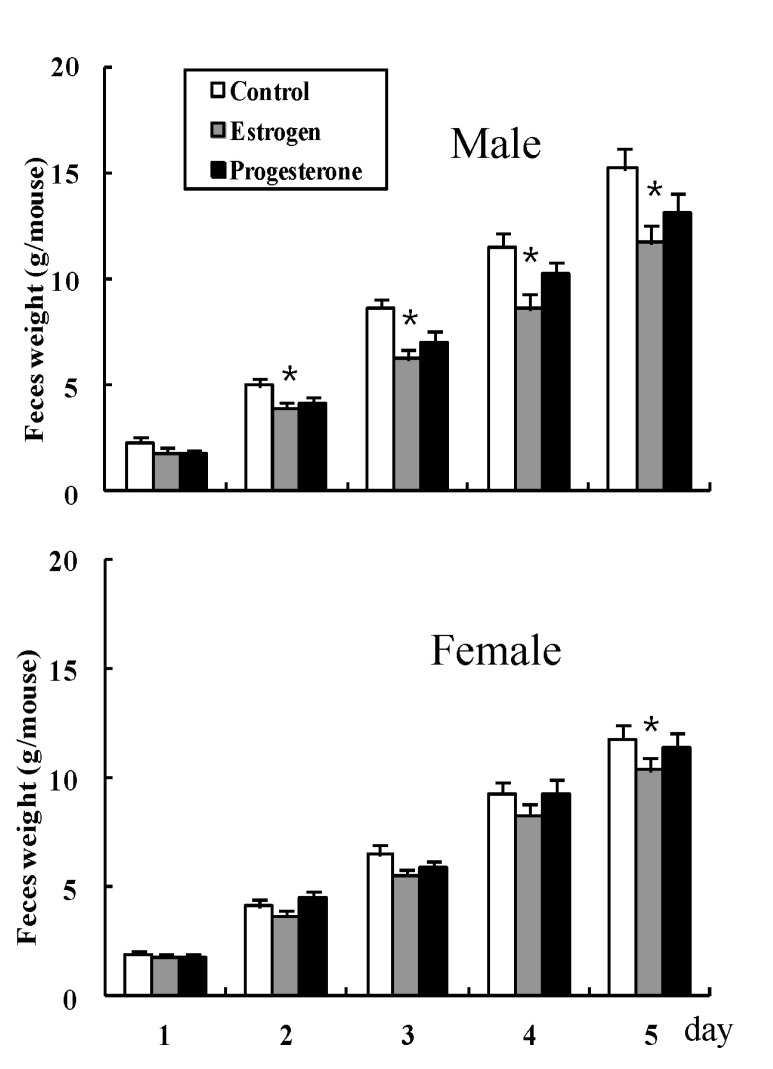
The weights of accumulated feces in male mice were 2.3±0.22, 5.0±0.35, 8.6±0.44, 11.5±0.62, and 15.2±0.93 on days 1, 2, 3, 4, and 5 (g) in the normal control mice group, respectively, 1.8±0.22, 3.9±0.32, 6.2±0.44, 8.6±0.65, and 11.7±0.78 on days 1, 2, 3, 4, and 5 (g) for estrogen administered mice, respectively, and 1.7±0.17, 4.1±0.29, 7.0±0.52, 10.2±0.62, and 13.1±0.88 on days 1, 2, 3, 4, and 5 (g) for progesterone administered mice, respectively. The accumulated weights of feces in female mice were 1.9±0.16, 4.1±0.27, 6.5±0.39, 9.3±0.53, and 11.8±0.91 on days 1, 2, 3, 4, and 5 (g) in the normal control mice group, respectively, 1.8±0.20, 3.7±0.28, 5.5±0.35, 8.3±0.54, and 10.4±0.83 on days 1, 2, 3, 4, and 5 (g) for estrogen administered mice, respectively, and 1.8±0.18, 4.5±0.28, 5.8±0.38, 9.3±0.61, and 11.4±0.84 on days 1, 2, 3, 4, and 5 (g) for progesterone administered mice, respectively (Fig. 2). Administration of estrogen resulted in a decrease in weight of accumulated feces on days 2, 3, 4, and 5 in male mice and day 5 in female mice, compared with the control group, but administration of progesterone did not (Fig. 2).
Dry weight of feces
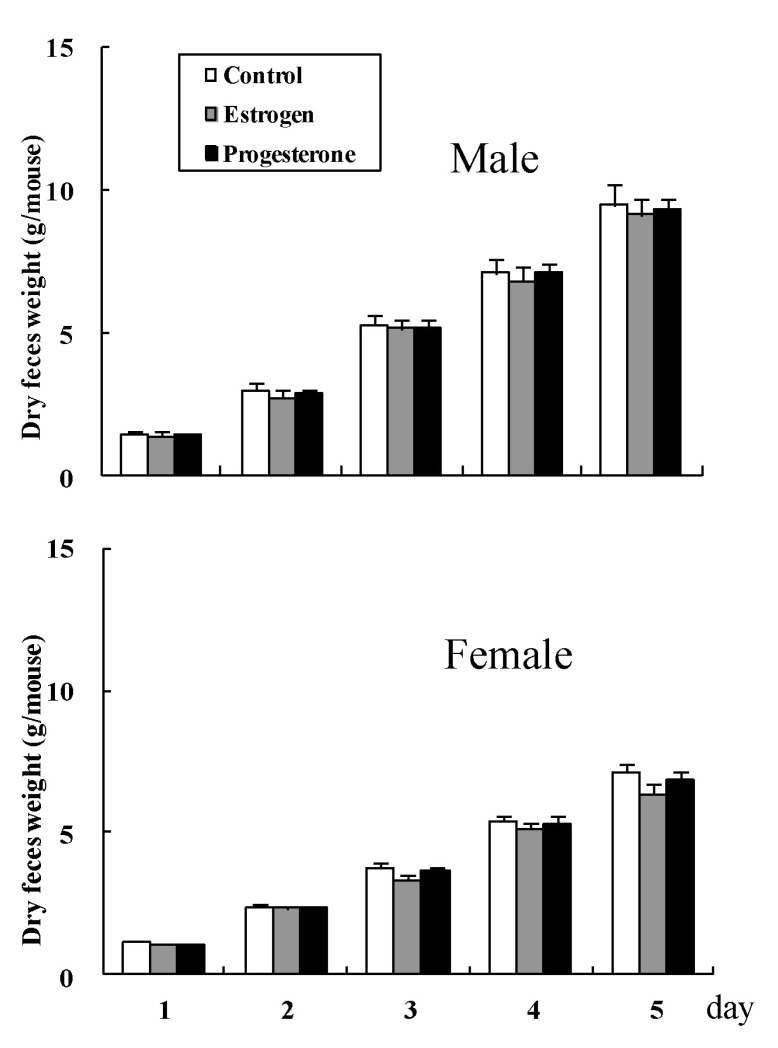
The accumulated dry weight (g) of feces did not differ significantly among groups in both male (1.4±0.06, 3.0±0.11, 5.3±0.25, 7.1±0.32, and 9.5±0.37 on days 1, 2, 3, 4, and 5 (g) for normal control mice, respectively, 1.4±0.06, 2.7±0.10, 5.1±0.28, 6.8±0.25, and 9.1±0.32 on days 1, 2, 3, 4, and 5 (g) for estrogen administered mice, respectively, and 1.4±0.05, 2.9±0.10, 5.2±0.31, 7.1±0.30, and 9.3±0.35 on days 1, 2, 3, 4, and 5 (g) for progesterone administered mice, respectively), and female mice (1.1±0.04, 2.4±0.08, 3.8±0.21, 5.4±0.24, and 7.1±0.29 on days 1, 2, 3, 4, and 5 (g) for normal control mice, respectively, 1.1±0.04, 2.3±0.08, 3.3±0.18, 5.1±0.23, and 6.4±0.31 on days 1, 2, 3, 4, and 5 (g) for estrogen administered mice, respectively, and 1.1±0.05, 2.3±0.07, 3.6±0.19, 5.3±0.28, and 6.8±0.32 on days 1, 2, 3, 4, and 5 (g) for progesterone administered mice, respectively) (Fig. 3).
Gastrointestinal movement
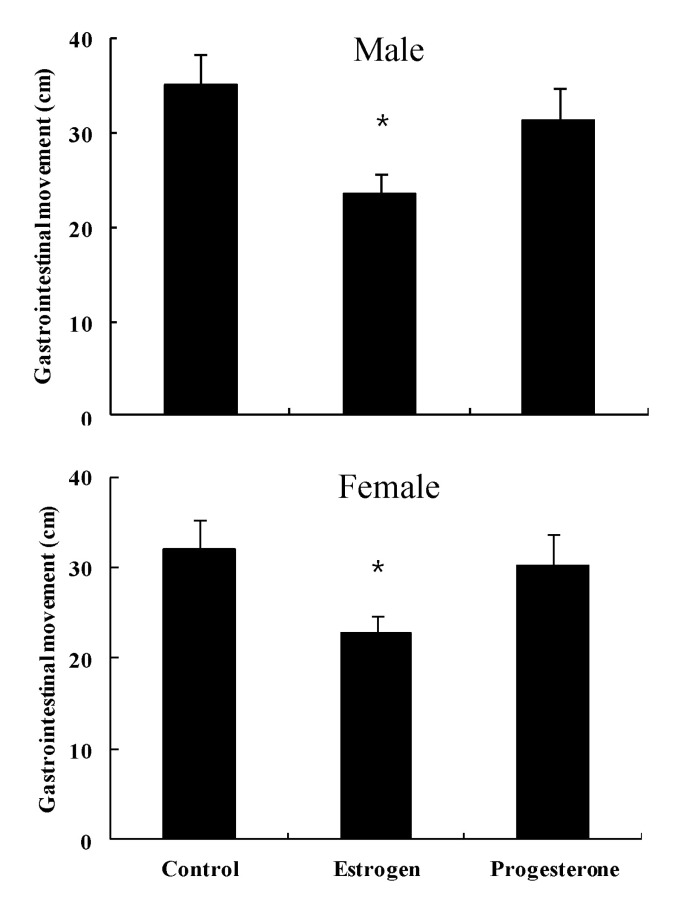
Length (cm) of barium transfer in normal control male mice was 35.2±3.3, and showed a decrease to 23.5±2.1 by administration of estrogen, but with no significant change (31.4±3.5) by administration of progesterone (Fig. 4). Length (cm) of barium transfer in normal control female mice was 33.1±3.1, and showed a decrease to 22.7±2.8 by administration of estrogen, but with no significant change (30.3±3.2) by administration of progesterone (Fig. 4).
Go to :
DISCUSSION
Constipation is a very common clinical problem [14] which may be associated with slow intestinal movement [15]. Women have a higher incidence of constipation than men, particularly in younger individuals [16]. The higher incidence is even more pronounced in female patients with slow transit constipation [17]. Ovarian hormones influence gastrointestinal function because estrogen receptors have been found in the gastric and small intestinal mucosa [18]. At the tissue level, female sex steroid hormones inhibit muscle contractility in a variety of sites, including lower esophageal sphincter [19], and colon [20]. Thus, alterations of progesterone and estrogen may be responsible. Although the association of female sex steroid hormones and constipation has been studied, it is still not clear. Incidence of constipation in females showed an increase [9] or did not change [11] in the luteal phase of the menstrual cycle. No significant difference in colonic transit time was observed between males and females [12]. The aim of this study was to clarify the effect of female sex steroid hormones on constipation. Our results showed that administration of estrogen induced constipation via a decrease in bowel movement in both male and female mice, but progesterone did not. This result suggests that estrogen, rather than progesterone, may be a detrimental factor of constipation caused by female sex steroid hormones, however, it does not show agreement with some reports [21-23] suggesting that progesterone is an important risk factor for constipation in women, and this hypothesis was supported by results indicating that females had greater frequency of constipation during menses [24,25] and pregnancy [5]. High progesterone levels contribute to inhibition of bowel motility and cause constipation [26]. However, findings of a recent study suggested the possibility that estrogen, rather than progesterone, may be responsible for the delay in gastric emptying and increase in colonic transit time observed in pregnancy [27]. Parenteral administration of estradiol, the predominant estrogen during reproductive years, to rats resulted in inhibited gastric emptying [28]. On the other hand, female rats treated with progesterone did not show a decrease in colon myoelectric signal, suggesting no constipation by female sex steroid hormones in virgin female rats [29]. Our study involving administration of female sex steroid hormones, such as estrogen and progesterone to male mice, appears to be the first study to evaluate the effect of these hormones on constipation. In conclusion, estrogen, rather than progesterone, may be a detrimental factor of constipation via decreased bowel movement in mice.
Go to :
 XML Download
XML Download