

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ocular ischemic syndrome (OIS) is a disease characterized by ischemia of the anterior and posterior segments of the eye due to reduced blood flow and is associated with a variety of clinical symptoms. The incidence of this condition increases with age and rarely occurs in people under 50 years old. Previous studies have shown that there are no ethnic differences in the incidence rate and that the condition occurs twice as frequently in men as in women, re-flecting the higher rate of atherosclerosis in men. There is no difference in the incidence rate between the left and right eyes, and both eyes are simultaneously affected in approximately 20% of cases of OIS. Annually, 7.5 people per million are diagnosed with OIS [123456]. However, the actual prevalence is thought to be higher because OIS can be obscured by or misdiagnosed as retinal vein occlusion or diabetic retinopathy [234].
OIS occurs most frequently as a secondary condition to carotid artery atherosclerosis. As a result, it is necessary to examine the whole body when OIS is suspected [2]. More than 90% of patients with OIS have pre-existing ipsilateral carotid stenosis [3]. Additionally, occlusion of either the common or internal carotid artery is seen in the majority of cases. A complete occlusion of the carotid artery on the affected side is found in 50% of all patients with OIS, and 10% of patients show complete occlusion of the carotid artery bilaterally [1]. However, even in cases of complete occlusion, OIS may not occur if the collateral circulation is well developed. According to Magargal et al. [3], occlusion of the ipsilateral ophthalmic artery alone can cause OIS. They suggested that this possibility should be considered if OIS is suspected clinically, even if the test results for the carotid artery are normal. Generally, the prognosis for vision is very poor in patients diagnosed with OIS, and 90% or more of patients with neovascular glaucoma (NVG) will become legally blind.
Although some studies have been conducted in other ethnic groups to investigate the clinical features of OIS and the risk factors for NVG, there have been no such studies to date in a Korean population. In this study, we aimed to examine the clinical features and prognosis of OIS and to investigate the factors associated with the development of NVG.
Materials and Methods
We conducted a retrospective review of the medical records of patients who had been diagnosed with OIS at Chonnam National University Hospital between January 2011 and December 2014. The inclusion criteria were an OIS diagnosis confirmed by slit lamp biomicroscopy, fluorescein angiography (FAG), and evaluation of the carotid artery, as well as a follow-up period of at least 6 months. Patients were excluded if they had a history of intraocular surgery or other underlying ophthalmological diseases such as open angle glaucoma, closed angle glaucoma, secondary glaucoma (including pigmentary glaucoma, exfoliation glaucoma, and uveitis glaucoma), or other chorioretinal diseases (including macular degeneration and uveitis). Patients with mild diabetic retinopathy or age-related cataracts were included.
To diagnose OIS, the patients underwent a full ophthalmic examination including best-corrected visual acuity as the mean logarithm of the minimum angle of resolution (logMAR), manifest refraction, slit lamp biomicroscopy, measurement of the intraocular pressure (IOP) using Goldmann applanation tonometry, an anterior chamber angle examination using gonioscopy, a fundus examination using fundus photography (Canon, Tokyo, Japan), and FAG using a Heidelberg HRA (Heidelberg Engineering, Heidelberg, Germany). The presence or absence of various comorbidities, including hypertension, diabetes mellitus, dyslipidemia, cerebrovascular diseases, and other cardiovascular diseases, as well as smoking history, were also recorded. A diagnosis of OIS was made from the carotid artery evaluation and FAG if there was either a prolonged arm-to-choroid (>15 seconds) and arm-to-retina circulation time (>18 seconds), or a prolonged retinal arteriovenous time (>11 seconds). We defined NVG in subjects as an IOP higher than 21 mmHg (measured by Goldmann tonometry), angle neovascularization observed using a gonioscopy lens, or neovascularization of the iris (NVI).
All patients were evaluated by the Department of Neurology for the extent of carotid artery stenosis and by the Department of Cardiology for coronary artery stenosis. The extent of carotid artery stenosis in all patients was assessed with non-invasive, contrast-enhanced magnetic resonance angiography and classified according to the criteria of the North American Symptomatic Carotid Endarterectomy Trial Collaborators (NASCET) [7] into the following groups: grade 0 (stenosis of 29% or less), grade 1 (30%–49%), grade 2 (50%–69%), grade 3 (70%–80%), grade 4 (80%–90%), and grade 5 (90%–99%).
Statistical analysis was performed using PASW ver. 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Patients with OIS were divided into two groups, those with and those without NVG. The two groups were compared using the Mann-Whitney U-test and Fisher exact test, as appropriate. Logistic regression analysis was performed to examine the risk factors for development of NVG. Pretreatment and posttreatment visual function were compared using the Wilcoxon signed-rank test. A p-value of less than 0.05 was considered to have statistical significance.
Results
Among the 30 patients diagnosed with OIS, 25 patients (25 eyes) were included in this study. Of the five eyes (of five patients) excluded from the analysis, four eyes had not received follow-up care and one eye had a comorbidity of glaucoma. The mean age at diagnosis of the 25 patients was 67.9 ± 12.50 years (range, 40 to 91 years), and there were 21 men and 4 women. The mean duration of symptoms was 54.96 ± 97.41 days. The most significant symptoms found at the initial examination were decreased visual acuity in 23 eyes and ocular or periorbital pain in five eyes. At the initial examination, the mean visual acuity was 2.11 ± 0.99 logMAR; and the mean IOP was 21.04 ± 10.33 mmHg (Table 1). Stenosis of the internal carotid artery was observed in all patients, and severe stenosis of the carotid artery of NASCET grade 4 or higher was diagnosed in 18 eyes (72%). Nine out of those 18 patients showed stenosis of 90% or more in the carotid artery that required surgical treatment, such as a carotid endarterectomy (Table 2). During a mean follow-up period of 12.60 ± 14.04 months, NVG developed in 17 eyes (68.0%). There were no significant differences in age, gender, visual acuity at initial examination, the incidence of comorbidities of cardiovascular and cerebrovascular diseases, smoking history, or time parameters of FAG between patients with and without NVG. However, there were significant differences in IOP at initial examination, the length of time between symptom occurrence and diagnosis, and the extent of ipsilateral carotid artery stenosis between the two groups (p = 0.027, p = 0.001, and p = 0.019, respectively). In addition, the incidence of hypertension, diabetes, and dyslipidemia was higher in the NVG group when compared with the non-NVG group (Table 3). The logistic regression analysis showed that the probability of NVG development was significantly higher if the time interval between the onset of symptoms and the initial hospital visit was longer than 7 days (p = 0.025; risk ratio, 0.064) or if the carotid artery stenosis was of NASCET grade 5 or higher (p = 0.032; risk ratio, 6.268) (Table 4).
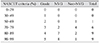
Various clinical features were found in patients with OIS, including NVI (48%), corneal edema (28%), narrowing of the retinal artery (92%), widening of the retinal vein (84%), macular cherry-red spots (16%), retinal hemorrhage (56%), and ischemic optic neuropathy (48%). In addition, delayed arterial filling (80%), delayed arteriovenous transit time (88%), and excessive fluorescence of the optic nerve (4%) were found using FAG. These findings in the anterior segment and the fundus were compared between the two groups; only NVI had a significantly higher rate (p = 0.002) in the NVG group (Fig. 1).
Among the 17 eyes with NVG, 13 eyes underwent panretinal photocoagulation and seven eyes were additionally treated with an intracameral injection of a vascular endo thelial growth factor inhibitor (Avastin; Roche Pharma, Switzerland). Six eyes with uncontrolled IOP and NVG underwent surgical management. One eye underwent a trabeculectomy, and Ahmed valve implantation was performed on the other five eyes. Carotid endarterectomy was performed in nine eyes with OIS in which the carotid artery was occluded. Despite these treatments, visual acuity was significantly decreased in any intervention groups (Table 5). At the last follow-up, the logMAR visual acuity was not significantly different between the NVG and non-NVG groups, and showed a poor prognosis in both groups. Blindness with no light perception developed in ten eyes (58.8%) from the NVG group and three eyes (37.5%) from the non-NVG group (p = 0.411).
Discussion
OIS is a disease in which ischemia occurs in the anterior or posterior segment of the eye due to reduced blood flow, and typically, 90% or more of the ipsilateral common carotid artery or internal carotid artery is narrowed [389101112]. If ischemia of the anterior or posterior segment persists as a result of carotid artery stenosis, NVG can develop [41314]. Occlusion of the carotid artery is the third most common cause of NVG, following central retinal vein occlusion and diabetes. According to Lazzaro [6], occlusion of the carotid artery is also found in approximately 50% of patients with retinal vein occlusion [5]. Therefore, the incidence of carotid artery occlusion as a cause of NVG may increase if the diagnostic methods used for the carotid artery are improved. This is the first study analyzing the associations between clinical characteristics, including the extent of carotid artery stenosis, of patients with OIS and the risk for NVG.
Decreased visual acuity is the most common symptom present at the initial hospital visit for OIS and is observed in more than 90% of cases [1]. Mizener et al. [2] reported that in 13% of the eyes with OIS, periorbital pain was also noted at the first hospital visit. In this study, four out of 17 patients with NVG (23.5%) and one out of eight patients without NVG (12.5%) complained of periorbital pain. Due to the relatively small sample size, the difference between the two groups did not reach statistical significance.
In this study, NVI was found in 12 out of 25 patients with OIS (48%). Ino-ue et al. [15] reported that NVI is a poor visual prognostic factor and that it is therefore essential to recognize the early stages of OIS associated with diabetes.
Posterior segment findings are more common than findings in the anterior segment of the eye. Both narrowing of the retinal artery and widening of the retinal vein are observed in almost all patients with OIS, and retinal hemorrhage is observed in approximately 80% of patients, while a macular cherry-red spot is observed in approximately 12% of patients [8]. In this study, narrowing of the retinal artery (92%) and widening of the retinal vein (84%) were observed in most patients, while a macular cherry-red spot (16%) was a less common finding.
The presence of an atheromatous plaque in the carotid artery is a major cause of OIS. According to a study by Sivalingam et al. [9], ischemic cardiovascular disease, a history of cerebrovascular accident, and peripheral arterial disease were observed in 48%, 27%, and 19% of patients, respectively, and hypertension and diabetes were observed in 73% and 56% of patients, respectively. According to a retrospective study by Brown and Magargal [10], hypertension was observed in 56% of patients, diabetes in 43%, cardiovascular disease in 35%, and a history of cerebrovascular accident or transient ischemic attack in 26%. These results are consistent with the findings of our study. These comorbidities might be explained by the pathogenic similarity between OIS and the aforementioned systemic conditions. An atheromatous plaque in the carotid artery leads to continuous ocular ischemia, making the eyes more susceptible to OIS.
In the present study, the extent of carotid artery stenosis was graded according to the NASCET criteria [7]. Carotid artery stenosis was significantly more severe in the NVG group compared with the non-NVG group, and a NASCET grade of 5 or higher was a significant risk factor for NVG. Since carotid artery stenosis progresses slowly, severe stenosis of the carotid artery might result in decreased blood flow to the eye over a long period of time and therefore predispose eye to NVG [161718192021222324]. The long-term decrease in blood flow could cause underlying structural changes, such as fibrovascular proliferation, in the anterior chamber angle.
The multivariate analysis also identified that a delay of 7 days or longer from the onset of symptoms to the patient seeking medical advice was a risk factor for developing NVG. As the length of time between symptom onset and the hospital visit increased, the incidence of NVG also increased. Karacostas et al. [19] reported a case of isolated OIS with no cerebral involvement and suggested that earlier referral for a simple carotid artery work-up can prevent both the carotid arterial occlusion and the development of severe ocular ischemia. Similarly, Wagner et al. [25] and Higgins [26] reported that although long-term ocular ischemia already exists before the first symptoms occur, early reperfusion interventions, including carotid endarterectomy, might play a crucial role in preventing NVG and can affect the long-term prognosis [27]. In the same manner, our results also suggest that an earlier visit (<7 days) after the initial ocular symptoms might prevent patients with OIS from developing NVG and could be the only control-lable factor for the prevention of NVG. We suggest that it is because the earlier the patient visits the hospital, the earlier the proper interventions can be achieved. Although an early diagnosis of OIS is generally challenging, and both the NVG and non-NVG groups had poor visual prognoses in our study, it is encouraging that we can give patients with suspected ocular ischemia attributable to cardiovascular or cerebrovascular diseases advice to decrease the development of NVG in the out-patient setting.
This study had some limitations. The sample size was relatively small, and because of the retrospective nature of our study, we could not collect adequate information to identify other possible risk factors. Additionally, the information regarding the duration of symptoms associated with OIS was obtained through self-reporting rather than by other objective medical findings, and this might have affected the interpretation of our results. Finally, the effects of collateral circulation and the possibility of combined ophthalmic artery occlusion were not considered. Several studies have evaluated the carotid siphon or ophthalmic artery using transcranial or transorbital Doppler ultrasonography in the analysis of carotid artery stenosis in patients with OIS [18212324]. However, we only analyzed stenosis of the common or internal carotid artery. In the future, longer-term and prospective studies, including the analysis of the relationship between ophthalmic artery occlusion or a carotid siphon and NVG, are needed for a more accurate analysis.
In conclusion, when patients visit the hospital more than 7 days after initially experiencing symptoms, or the carotid artery stenosis is of NASCET grade 5 or higher, the probability of NVG occurring in patients with OIS increases. Our results clearly show that a more proactive approach should be taken in the diagnosis and follow-up of patients with these risk factors.





 XML Download
XML Download